
Abstract
Arteriovenous fistula between the left vertebral artery and the inferior thyroid vein is a rare entity. This condition can change the blood supply of the basilar artery system, and then lead to an abnormal blood supply of the vertebral body. Therefore, this rare condition may be misdiagnosed in the clinic. We report an arteriovenous fistula between the left vertebral artery, which was found during an interventional operation of a 49-year-old Asian man. He was non-diabetic and an ex-smoker, and presented with a 1-month history of pain in the neck, shoulder, waist, back, and right lower limb. Vascular angiography showed an arteriovenous fistula, and coils were placed in the fistula. In this setting, coil embolization was effective, and a 1-year follow-up suggested that a good long-term result was likely.
Introduction
A vertebral arteriovenous fistula is characterized by anomalous connections between the vertebral artery, or its branches. 1 Vertebral arteriovenous fistulas can be caused by accidents, such as blunt trauma with a vertebral fracture and an iatrogenic origin. These fistulas always present as pulsatile bruits and tinnitus, which result from disturbed blood flow within an abnormal arteriovenous connection. 2 Because of the specific characteristics of this clinical presentation, few surgeons and vascular centers have developed any considerable experience with managing vertebral arteriovenous fistulas. 3
Arteriovenous fistula between the left vertebral artery and the inferior thyroid vein is exceedingly rare. We report here a case of a male patient with an arteriovenous fistula between the left vertebral artery and the inferior thyroid vein.
Case report
A 49-year-old Asian man who was non-diabetic and an ex-smoker presented with a 1-month history of vertigo, pain in the neck, shoulder, waist, back, and right lower limb. He presented to the Department of Pain. His family history was unremarkable. He had negative pathological signs and no history of alcohol abuse or use of neuropsychiatric drugs.
Initially, we suspected that he had protrusion of the intervertebral discs. However, spinal magnetic resonance imaging (MRI) showed no evidence of protrusion of the intervertebral discs, but a peripheral vascular malformation of the spinal cord was observed (Figure 1). He was then transferred to the Department of Interventional Therapy. Vascular angiography showed steal syndrome, and the right vertebral artery was thickened. The basilar artery and its branches were normal, and the steal phenomenon was observed in the left vertebral artery (Figure 2). We observed that the left vertebral artery was tortuous and thickened, and communicated with the left inferior thyroid vein (Figure 3). We also found that the blood flowed into the left inferior thyroid vein and the left brachiocephalic vein through a fistula of the V1 segment of the left vertebral artery.

Spinal magnetic resonance image shows peripheral vascular malformation of the spinal cord.
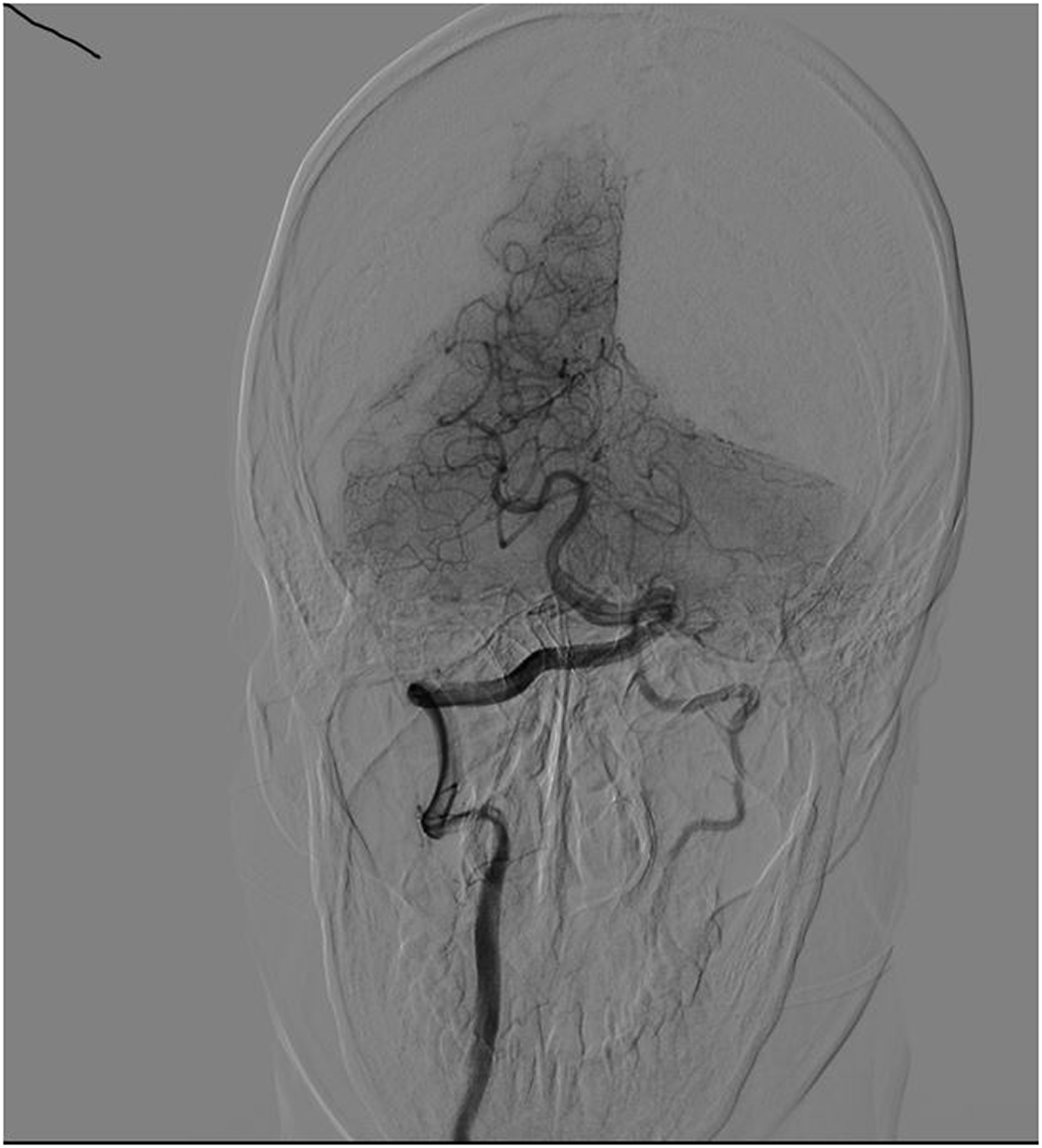
Vascular angiography shows steal syndrome.

Vascular angiography shows that the left vertebral artery is tortuous and thickened, and communicates with the left inferior thyroid vein.
On the basis of these vascular images, the diagnosis of a fistula (Yakes classification: type I arteriovenous malformation) between the left vertebral artery and the inferior thyroid vein was made. Under local anesthesia, a guiding catheter was placed into the fistula via the femoral artery. Coils were placed in the fistula via a catheter, which was transferred over the guide wire, and it achieved shunt occlusion with coil embolization (Figure 4). During a 1-year follow-up, he remained stable with no communication between the left vertebral artery and the inferior thyroid vein on follow-up angiography. Postembolization MRI and postoperative three-dimensional vascular reconstruction based on computed tomography angiography showed that most of the dilated vessels had disappeared and a good effect was achieved (Figures 5, 6).

Coils were placed in the fistula, achieving shunt occlusion with coil embolization.

Postembolization magnetic resonance imaging shows that most of the dilated vessels have disappeared.

Postoperative three-dimensional vascular reconstruction based on computed tomography angiography shows that most of the dilated vessels have disappeared with a good effect.
Discussion
A fistula between the left vertebral artery and the inferior thyroid vein is exceedingly rare. To the best of our knowledge, only one case was reported in French in 1961. 4 Therefore, our case may be the first to be reported in English and diagnosed with angiography. The pathophysiology of a fistula is that arterial perfusion in the ipsilateral vertebral artery is diminished, leading to a pressure gradient and flow diversion from the ipsilateral vertebral to the subclavian artery. This situation leads to the steal phenomenon. Steal syndrome is defined as a decrease in the mean flow velocity in the affected artery with a simultaneous increase in the mean flow velocity in the contralateral, nonaffected artery.5,6 Patients with a fistula who are symptomatic often have complaints or symptoms associated with an insufficient blood supply of the basilar artery. 7 In this setting, vertigo may occur owing to transient ischemia of the inferior cerebellum or lateral medulla.
Digital subtraction angiography remains the gold standard for the diagnosis of most vascular diseases. Nevertheless, because digital subtraction angiography is an invasive method requiring considerable iodine-containing contrast, it should be reserved for situations where suspicion is high, rather than as a screening test. 8 Therefore, a digital subtraction angiography examination should be established when computed tomography and MRI suggest hemodynamic changes.
Generally, the treatments for brain arteriovenous fistula include endovascular treatment, open surgical resection, and radiosurgery. A characteristic feature of surgical resection is wide exposure of the relevant anatomy and occlusion of the arteriovenous fistula. However, the use of surgical resection should be based on preoperative vascular imaging (e.g., angiography). Derdeyn et al. found that open surgery has a high rate of complete obliteration and long-term durability, 9 but the disadvantages of surgical resection include open craniotomy, which adds the risk of perioperative neurological morbidity. 10 Therefore, surgical resection is controversial. Radiosurgery is not considered the first choice and it is reserved as a last salvage option for treatment. 11 Our patient received endovascular treatment because the formation time of the arteriovenous fistula was long, the local blood vessels were tortuous and greatly dilated, the anatomical structure of normal blood vessels had disappeared, and the surrounding tissues were compressed and displaced. Therefore, open surgery would have been difficult and the risk was high.
With regard to endovascular treatment, different agents, including balloons, coils, and glue, have been reported in clinical practice. 12 However, in this case, balloon-assisted glue embolization was not the optimum choice because of the high blood flow. Additionally, balloon-assisted glue is irritating to some patients, and it often requires general anesthesia. Coil embolization is an effective option in the treatment of other complex conditions.13,14 Coil embolization was effectively used in our patient, allowing exclusion of the fistula without complications. A 1-year follow-up suggested that a good long-term result was likely.
In conclusion, arteriovenous fistula between the left vertebral artery and the inferior thyroid vein is a rare condition. The findings from our case suggest that coil embolization is effective in treating this condition. This case may be helpful for interpreting the diagnosis and for treating patients with vertebral arteriovenous fistula.
Footnotes
Acknowledgements
We thank Prof. Komoda Nobutaka, who is a radiologist at Osaka, for his comments on the revised manuscript.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Ethics statement
This article was approved by the Ethics Committee of the Affiliated Hospital of Qinghai University. The patient and his parents agreed to the use of his imaging and clinical data for publication and academic research, and they provided written informed consent.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.