
Abstract
General anaesthesia with a muscle relaxant is usually performed for rigid bronchoscopy (RB), but ventilation is challenging due to large amounts of leakage. Optiflow™ supplies 100% humidified, warmed oxygen at a rate of up to 70 l/min and this high flow rate may overcome the leakage problem. This case report describes four patients that were scheduled for RB. The lung lesions were all located below the carina, so a bronchial tube was inserted under general anaesthesia. Once a large amount of leakage was confirmed by manual ventilation, Optiflow™ was connected to the bronchial tube (flow rate, 70 l/min). All of the ports of the bronchoscopy were left open to prevent the risk of outlet obstruction. Oxygenation was well maintained with stable vital signs throughout the procedures, which took up to 34 min without airway intervention. There were no occurrences of cardiac arrhythmia or changes in the electrocardiograms. Respiratory acidosis recovered after emergence, which was confirmed by arterial blood gas analysis in all cases. Apnoeic oxygenation using Optiflow™ was applied successfully during RB. Applying Optiflow™ could make cases of difficult ventilation during RB much easier for the anaesthetist. Larger studies need to demonstrate the efficacy and safety of this technique.
Introduction
Rigid bronchoscopy (RB) is more invasive and stimulatory than flexible bronchoscopy and requires deep sedation or general anaesthesia.1,2 In therapeutic interventions, RB is usually performed under general anaesthesia using a muscle relaxant.1,3 There are two types of tubes used for RB; bronchial and tracheal tubes. Bronchial tubes are longer and thinner than tracheal tubes and have multiple fenestrations for ventilation of the non-intubated lung (Figure 1). These fenestrations in addition to the uncuffed, thin tube make a large amount of leakage inevitable. Thus, it is more difficult to maintain ventilation with a bronchial than a tracheal tube. Furthermore, because of the open airway system shared with the bronchoscopist, ventilation during RB is more challenging.

The heated tube of the Optiflow™ was connected to the bronchial tube. The colour version of this figure is available at: http://imr.sagepub.com.
Optiflow™ (Fisher & Paykel Healthcare, Auckland, New Zealand), a commercial transnasal humidified rapid insufflation ventilatory exchange (THRIVE) device that supplies 100% humidified, warmed oxygen at a rate of up to 70 l/min, has been used during the perioperative period. 4 Optiflow™ could overcome the problem of leakage through high flow and enable apnoeic oxygenation during RB. When accompanied by a deep understanding of the physiological basis and complications of apnoeic oxygenation, Optiflow™ could be a viable alternative ventilatory strategy during RB. This case report describes four patients in whom apnoeic oxygenation using Optiflow™ was applied successfully during scheduled RB.
Case reports
Case 1
In December 2020, a 61-year-old female with diabetes mellitus was diagnosed with necrotizing aspergilloma in the left upper lobe of the lung and scheduled for bronchoscopic removal of the obstructing endobronchial lesion in the Department of Anaesthesiology and Pain Medicine, Soonchunhyang University Bucheon Hospital, Soonchunhyang University College of Medicine, Bucheon, Republic of Korea. Total intravenous anaesthesia (TIVA) was induced using propofol and remifentanil, and intubation was performed with an endotracheal tube. The surgeon inserted the bronchial tube using the ‘intubation over the endotracheal tube’ method. 5 Because a large amount of leakage had prevented adequate ventilation through manual ventilation, Optiflow™ was connected to the bronchial tube and oxygen was supplied at a rate of 70 l/min. In such a high flow, if leakage is not confirmed, excessive volume and pressure could lead to catastrophic complications, so all of the ports of the bronchoscopy were left unsealed and open (Figure 2). The oxygen supply was maintained for 17 min until the end of the procedure and peripheral oxygen saturation (SpO2) was maintained at 100% with stable vital signs. After the surgeon replaced the RB with an endotracheal tube, the patient was administered 200 mg sugammadex and awakened. The first end-tidal carbon dioxide (EtCO2) was 78 mmHg and an arterial blood gas analysis (aBGA) results 30 min after emergence were within the normal ranges (pH, 7.367; PaO2, 100 mmHg; PaCO2, 43 mmHg; bicarbonate, 24.3 mmol/l).

Apnoeic oxygenation using Optiflow™. The high flow of Optiflow™ can overcome a large amount of leakage. All of the ports of the bronchoscopy were left unsealed and open to confirm the leakage and prevent the risk of outlet obstruction. The colour version of this figure is available at: http://imr.sagepub.com.
Case 2
In December 2020, a 91-year-old male patient with hypertension and diabetes mellitus was scheduled for removal of a foreign body in the left main bronchus via RB due to failed flexible bronchoscopy in the Department of Anaesthesiology and Pain Medicine, Soonchunhyang University Bucheon Hospital, Soonchunhyang University College of Medicine, Bucheon, Republic of Korea. Anaesthesia was induced with TIVA. After muscle relaxation, the surgeon inserted a rigid bronchial tube via the ‘laryngoscope method’ 5 and a large amount of leakage was confirmed by manual ventilation. Optiflow™ was connected to the bronchial tube and the oxygen flow was maintained at 70 l/min during the procedure without using the sealing cap. Total procedure time was 22 min without any airway intervention and vital signs were stable without desaturation or electrocardiogram (ECG) changes. The patient recovered from anaesthesia without any adverse events. An aBGA performed in the post-anaesthesia care unit (PACU) revealed values within the normal ranges (pH, 7.44; PaO2, 120 mmHg; PaCO2, 40 mmHg; bicarbonate, 27.2 mmol/l).
Case 3
In January 2021, a 38-year-old female patient that takes levothyroxine because of Hashimoto’s thyroiditis was scheduled for a bronchoscopic biopsy due to diffuse interstitial lung disease in both lower lobes in the Department of Anaesthesiology and Pain Medicine, Soonchunhyang University Bucheon Hospital, Soonchunhyang University College of Medicine, Bucheon, Republic of Korea. The initial SpO2 was 95%, and a rigid bronchial tube was inserted using the ‘intubation over endotracheal tube’ method after inducing anaesthesia. After checking the large amount of leakage with manual ventilation, oxygen was supplied at a rate of 70 l/min using Optiflow™. The SpO2 decreased to 93% but was maintained above 91% during the entire procedure without any ECG changes. Total procedure time was 34 min without airway intervention and an aBGA performed at the end of the procedure showed severe respiratory acidosis (pH, 6.97; PaO2, 79 mmHg; PaCO2, 132 mmHg; bicarbonate, 27.2 mmol/l). A supraglottic airway device was inserted after removing the rigid bronchial tube and the first EtCO2 was 70 mmHg. After emergence, an aBGA performed in the PACU revealed values in the normal ranges (pH, 7.38; PaO2, 138 mmHg; PaCO2, 39 mmHg; bicarbonate, 23.1 mmol/l).
Case 4
In February 2021, a 53-year-old male patient with asthma was scheduled for RB and endoscopic excision of an obstructing lesion in the right intermedius bronchus in the Department of Anaesthesiology and Pain Medicine, Soonchunhyang University Bucheon Hospital, Soonchunhyang University College of Medicine, Bucheon, Republic of Korea. He did not complain of dyspnoea and the initial SpO2 was 98%. After arterial cannulation, a baseline aBGA was performed. Preoxygenation was performed with 20 l/min of oxygen using Optiflow™ for 3 min, with his mouth closed. After anaesthesia induction using propofol and remifentanil, a bronchial tube was inserted into the bronchus and leakage was confirmed by manual ventilation. Oxygen was supplied at a rate of 70 l/min using Optiflow™ and the SpO2 was well maintained at 100%. After 5 min after intervention, laser ablation was planned to dissect the lesion. For lowering the inspired fraction of oxygen (FiO2), the Optiflow™ was stopped and manual ventilation was started with FiO2 of 0.3 and flow rate of 10 l/min. A large amount of leakage prevented adequate manual ventilation and the SpO2 decreased to 96%. Laser ablation was ended after 3 min (10 min after intervention). Optiflow™ was resupplied at a rate of 70 l/min and the SpO2 immediately recovered to 100%. The procedure was terminated after 5 min without airway intervention (15 min after intervention). An aBGA performed in the PACU was within the normal range (Table 1).
Arterial blood gas analysis (aBGA) over time in a 53-year-old male patient (case 4) with asthma that was scheduled for rigid bronchoscopy and endoscopic excision of an obstructing lesion in the right intermedius bronchus.
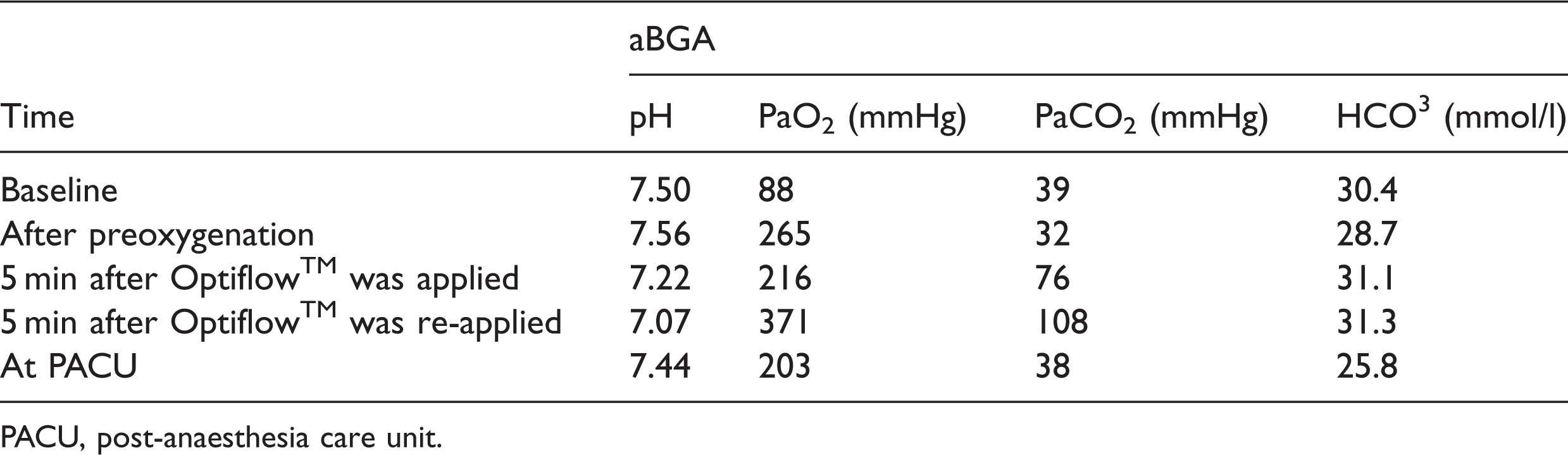
PACU, post-anaesthesia care unit.
These case studies were approved by the Institutional Review Board of Soonchunhyang University College of Medicine (IRB No. 2021-02-013) and the requirement for informed consent was waived because all data were obtained by retrospective chart review. The reporting of this study conforms with CARE guidelines. 6 All patients were informed about the anaesthesia method that they would receive before the surgery.
Discussion
An inappropriate ventilatory strategy during RB can lead to fatal complications, such as hypoxaemia, hypercapnia and hypotension, which extends the procedure time. A leakage is inevitable during RB, particularly when using a bronchial tube, so adequate ventilation can be difficult. Apnoeic oxygenation using Optiflow™ was successfully used in four patients scheduled for RB, where the entire procedure time was 17–34 min. The bronchial tube acted as a conduit for direct delivery of oxygen and the large amount of leakage was overcome by using a high flow rate of 70 l/min.
Optiflow™ produces oxygenation via ‘aventilatory mass flow’. 7 A previous report stated that apnoea was maintained for up to 65 min during upper airway surgery. 8 Airway patency should be secured to ensure a high oxygen flow rate to the alveoli. Several studies have reported that pharyngeal catheters deliver oxygen more effectively to alveoli by reducing the distance from the oxygen outlet to the pharyngeal inlet.9–11 A bronchial tube is inserted through the trachea into the bronchus, so that direct delivery of oxygen to the alveoli is possible. An open airway system produces a large amount of leakage, but this can be overcome by using a 70 l/min oxygen flow rate. Since the amount of leakage was unpredictable, as high as possible flow rate was applied in these current four cases.
However, if no leakage is present, catastrophic complications may occur, such as barotrauma and volutrauma generated by the high oxygen flow rate. This is why leakage was confirmed by manual ventilation in the current cases before applying Optiflow™. In addition, all of the ports of the bronchoscopy were left open to confirm the leakage and prevent the risk of outlet obstruction, which allowed the sound of leakage to be heard while applying Optiflow™. Since all procedures were performed using flexible bronchoscopy through rigid bronchoscopy, the risk of outlet obstruction could also be excluded by watching the video displayed on the monitor. In the PACU, postoperative chest X-ray was performed to check for problems such as pneumothorax.
Jet ventilation is commonly used during RB 1 because it enables adequate ventilation and provides access to the airway. 12 However, jet ventilation requires special equipment and familiarity with this technique. A motionless operative field is also considered beneficial for high-frequency jet ventilation, 1 but this can be achieved via apnoeic oxygenation using Optiflow™. Apnoeic oxygenation using Optiflow™ makes the anaesthetist operate in a hands-free manner, so they can focus on other aspects of anaesthesia aside from ventilation.
Apnoeic oxygenation carries a risk of hypercapnia; this can be also caused by the Optiflow™ device, although the rate is lower compared with conventional apnoea. 8 The high flow of oxygen can flush out the expired CO2, thereby reducing the CO2 accumulation. 13 Because EtCO2 cannot be monitored during apnoea, serial aBGA or transcutaneous capnography should be used to monitor CO2. This was a limitation in this current case series. Because there is the risk of acidosis and cardiac arrhythmia, the ECG should be monitored more carefully. In these current cases, acute respiratory acidosis disappeared after the end of anaesthesia, as confirmed by aBGA after emergence. However, further studies on the rate of increased CO2 are required when direct delivery of oxygen to the alveoli is applied.
Several precautionary measures are required before applying Optiflow™ during RB. First, leakage should be confirmed. A high oxygen flow can itself cause catastrophic complications. Therefore, for safety reasons, it is necessary to continuously check for leakage. Secondly, Optiflow™ cannot be used in procedures with a risk of airway fire, such as laser ablation. In these procedures, another type of THRIVE device that allows adjustment of FiO2 or another ventilatory strategy should be employed. Thirdly, the anaesthetist should consider alternative ventilatory strategies and the equipment must be prepared meticulously. It is also important to consider the basal lung function of the patient, extension of the lesion and type of intervention. Finally, monitoring the level of CO2 should be undertaken throughout entire procedure.
In conclusion, skilled anaesthetists are required for successful ventilation during RB. If the anaesthetist applies the Optiflow® device properly, it may be a good ventilatory option during RB. Optiflow™ may overcome a large amount of leakage and allow the anaesthetist to ventilate more easily without airway intervention in a setting of the shared airway. In addition, it should be kept in mind that meticulous attention is needed for possible complications that may occur due to apnoeic oxygenation using the high flow of oxygen. As these current findings are based on four cases, it would be improper to recommend this technique until further larger efficacy and safety studies have been published.
Footnotes
Author contributions
Jaewoong Jung helped with the study conception, protocol design, administered the anaesthesia and wrote/revised the manuscript. Misoon Lee helped with the protocol design and collected the data. Juhui Park helped with conducting the study and collected the data. Yang-Hoon Chung helped with the study conception, protocol design and revised the manuscript. All authors provided approval for the final version of the manuscript.
Acknowledgements
We would like to thank the nurses in the PACU at Soonchunhyang University Bucheon Hospital for their help.
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and publication of this article: This work was supported by the Soonchunhyang University Research Fund.