
Abstract
We report the case of a 47-year-old male patient with pigmentation of the head, face and hands, who was initially diagnosed as having primary adrenal insufficiency (Addison’s disease). Laboratory testing, imaging and physical examination revealed subclinical hypothyroidism, high circulating prolactin and oestradiol concentrations, gynaecomastia, lymphadenopathy, splenomegaly and weakness of both lower limbs. These findings led us to consider whether a single or multiple diseases were present in this patient. Indeed, Addison’s disease can represent one aspect of a wider systemic disease. Therefore, we performed further examinations, and found high serum M protein (5.1%) and vascular endothelial growth factor [1005.30 pg/mL (normal range 0 to 142 pg/mL)] concentrations. As a consequence, we diagnosed polyneuropathy, organomegaly, endocrinopathy, monoclonal gammopathy and skin changes (POEMS) syndrome. Consequently, when a single disease cannot fully explain the multiple symptoms and signs of one patient, clinicians should consider the possibility of the presence of a wider syndrome and undertake more detailed diagnostic testing.
Keywords
Introduction
Primary adrenal insufficiency (PAI), also called Addison’s disease, is the clinical manifestation of chronic glucocorticoid and/or mineralocorticoid deficiency that results from damage to the adrenal cortex, and may lead to a life-threatening adrenal crisis or have other potentially serious consequences 1 in some severe cases. There are a number of potential causes and contributors to Addison’s disease, including infection (most commonly tuberculosis in China), autoimmune diseases, adrenal resection, neoplastic and genetic disorders (most commonly in children), and other iatrogenic conditions, such as the side effects of anticoagulants and novel anti-cancer target spot inhibitors. 2 Therefore, the cause of the disease should initially be sought, to facilitate aetiologically-focused treatment, but glucocorticoid/mineralocorticoid replacement therapy should also be provided. 3
POEMS syndrome is a rare systemic disease that is caused by clonal plasma cell proliferation, and is named after its features: polyneuropathy, organomegaly, endocrinopathy, monoclonal gammopathy and skin changes. The prevalence of the syndrome was found to be 0.3 per 100,000 in a large national survey in Japan conducted in 2003 4 and it is approximately 2.5 times commoner in men than women. The median age of onset is usually 50 to 60 years of age. 5 Because of its gradual onset, patients with POEMS syndrome may be asymptomatic or present with symptoms related to nervous system and multi-endocrine dysfunction. Therefore, the condition may not be diagnosed at an early stage, which seriously affects the prognosis of the patients.
In the present case report, we describe a middle-aged male patient who presented with pigmentation of the head, face and hands, and was initially diagnosed as having Addison’s disease. After excluding other causes of adrenocortical damage, it was found that the serum concentrations of myeloma (M) protein and vascular endothelial growth factor (VEGF) were high. On the basis of these and the findings of other haematological and bone marrow examinations, a diagnosis of POEMS syndrome was made. The purpose of the report is to aid clinicians’ understanding of POEMS syndrome and increase awareness regarding approaches to the diagnosis of systemic diseases.
Case report
A 47-year-old male patient presented to the outpatient clinic of the Department of Endocrinology and Metabolism, West China Hospital of Sichuan University with a 2-year history of pigmentation of the head, face and hands, fatigue, and hyperhidrosis. Analysis of his circulating hormone concentrations revealed his cortisol concentration at 08:00 to be 421.5 nmol/L (normal range 147.3 to 609.3 nmol/L) and his adrenocorticotropic hormone (ACTH) concentration to be 29.18 pmol/L (normal range 1.01 to 17.18 pmol/L). Six months prior to presentation, his symptoms had become more severe and were accompanied by weakness and symmetrical pitting oedema of both lower extremities. The patient had also experienced low appetite, poor sleep, a loss of 5 kg in mass, and hyposthenia during the preceding 6 months. The patient was born and lived in Nanbu County and was a high-school teacher. He stated no knowledge of any relevant family history or the occurrence of analogous problems in his local area. He had not knowingly been exposed to toxic or radioactive substances and he had no history of smoking or alcohol consumption. Moreover, the patient had no history of hepatitis, tuberculosis or other serious infectious diseases.
Physical examination revealed a body temperature of 36.4°C, heart rate of 83 beats/minute, respiratory rate of 20 breaths/minute, blood pressure of 103/67 mmHg, height of 166 cm, body mass of 65 kg, body mass index (BMI) of 23.59 kg/m2 and waist circumference of 93 cm. The patient displayed a normal level of consciousness. His body hair was sparse, and skin pigmentation of the face, back of the hands and palms (shown in Figure 1), and especially of the areolae, was apparent (shown in Figure 2). Nodules were palpable in the upper inner quadrants of both breasts, and these were firm, mobile, clearly demarcated, and approximately 2 cm in diameter. Lymph nodes of approximately 1 cm in diameter were palpable in both armpits and in the groin, and these were hard, clearly demarcated and mobile. He had oedema of the eyelids and pitting oedema of both lower extremities. Cardiopulmonary and abdominal examinations revealed no abnormalities. The patient’s muscle strength in his upper and lower limbs was grade 5. Physiological reflexes were present and pathological signs were not elicited on neurological examination. The examinations performed in this patient were approved by the Ethics Committee of West China Hospital, Sichuan University, and the patient provided his written informed consent.
The principal laboratory test results for the patient are shown in Table 1. His free testosterone (FT) concentration was estimated using his total testosterone, sex hormone-binding globulin (SHBG) and albumin concentrations, and this approach closely mirrors the results of equilibrium dialysis 6 . An ACTH stimulation test was performed to further evaluate the patient’s adrenal reserve. Two hundred and fifty micrograms of ACTH were intravenously injected and the patient’s serum cortisol concentration was then measured 0, 30 and 60 minutes later. As shown in Table 2, the peak concentration of cortisol was below 500 nmol/L, suggesting insufficient adrenal reserve. Therefore, a diagnosis of Addison’s disease was considered.
Laboratory data for the patient.

HGB, haemoglobin; PLT, platelet count; GLU, glucose; TSH, thyroid-stimulating hormone; FT4, free tetraiodothyronine; LH, luteinising hormone; FSH, follicle-stimulating hormone; PRL, prolactin; E2, estradiol; TT, total testosterone; FT, free testosterone; DHEA-S, dehydroepiandrosterone sulfate; PRA, plasma renin activity; AT-II, angiotensin II; ALD, aldosterone; ACTH, adrenocorticotropic hormone; PTC, plasma total cortisol.
Fast ACTH stimulation testing results.
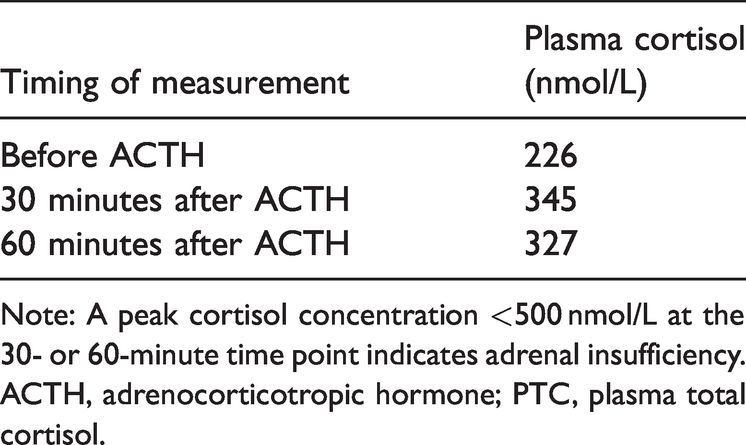
Note: A peak cortisol concentration <500 nmol/L at the 30- or 60-minute time point indicates adrenal insufficiency.
ACTH, adrenocorticotropic hormone; PTC, plasma total cortisol.
Infection, autoimmune diseases, adrenal resection, and neoplastic and genetic disorders can all cause Addison’s disease.7,8 The findings of a large study conducted at a single centre in China (131 cases) showed that adrenal tuberculosis was the most frequent cause of Addison’s disease, accounting for 32.1% (42/131) of cases. 8 In the present case, there were no definite findings of active tuberculosis in the chest, abdomen or other parts of the body of the patient, and adrenal-enhanced computed tomography (CT) revealed bilateral adrenal hyperplasia. We have not been able to locate reports of any other similar cases of POEMS syndrome. The patient may have been manifesting hyperplasia in compensation for insufficient adrenocortical reserve, but the evidence regarding tuberculosis was not definitive. In addition, the anti-adrenal autoantibody titre should be measured to exclude the possibility of autoimmune damage to the adrenals.
The patient’s symptoms improved after replacement therapy with prednisone 2.5 mg per os daily. However, a series of clinical features and test results in the present patient could not be explained by Addison’s disease alone, including his gynecomastia, lymphadenopathy, splenomegaly, oedema of the lower limbs, and high oestradiol and prolactin concentrations. For example, some physiological factors, including dietary, sleep, emotional and environmental problems, can induce hyperprolactinemia. Therefore, it is reasonable to question whether a single disease could have fully explained all the patient’s symptoms.
To identify any other causes of the patient’s symptoms and signs, we conducted a series of further relevant examinations. The results of pituitary-enhanced magnetic resonance imaging and bone scanning were negative. Pulmonary CT revealed nodules in the lower lobe of the right lung and enlargement of the axillary lymph nodes. Ultrasonographic examination of his abdomen and breasts revealed splenomegaly (5.2-cm thickness) and gynecomastia. Ultrasonographic cardiography showed the presence of a small amount pericardial effusion and an ejection fraction of 67%. Electroneuromyography identified polyneuropathy of both lower extremities. Serum protein electrophoresis (SPE) showed that M protein accounted for 5.1% of the total, and immunofixation electrophoresis revealed a monoclonal IgA λ peak, with an immunoglobulin (Ig)A concentration of 24.99 µmol/L (normal range 5.23 to 18.13 µmol/L) and a light-chain λ concentration of 7.03 g/L (normal range 3.80 to 6.50 g/L). Bone marrow smear and biopsy showed that plasma cells accounted for 2.5% of the total blood cell count. His serum VEGF concentration was 1005 pg/mL (normal range 0 to 142 pg/mL). Chest CT revealed no osteosclerosis. On the basis of the above symptoms, signs and auxiliary examination data, we considered a diagnosis of POEMS syndrome, and the patient was transferred to the Department of Haematology, where he was treated with lenalidomide 25 mg (D1-21) in combination with dexamethasone 40 mg on days 1, 8, 15 and 22. After three courses of chemotherapy, the skin colour, breasts and lymph nodes of the patient gradually returned to normal (shown in Figure 3), his VEGF concentration decreased to 470 pg/mL, his M protein proportion on SPE was 0% and he was weakly positive for IgA λ immunoglobulin on immunofixation electrophoresis.
Discussion
In 1980, Bardwick et al. combined the initials of five of the main clinical features of the syndrome (polyneuropathy, organomegaly, endocrinopathy, M-protein and skin changes) and christened it POEMS syndrome. It is a rare paraneoplastic syndrome that results from a clonal plasma cell disorder. 9 Other features of the syndrome involve papilloedema, extravascular volume overload, sclerotic bone lesions and thrombocytosis/erythrocytosis. POEMS syndrome has a variety of clinical characteristics, and we show a comprehensive summary of the clinical features of POEMS syndrome, derived from several large retrospective series conducted in various countries,10–17 in Table 3. The diagnostic criteria for POEMS syndrome were updated by Dispenzieri in 2019 (shown in Table 4 18 ). The patient described in this report displayed two mandatory major clinical criteria, a third major criterion, in the form of high circulating VEGF concentration, and several minor criteria (including splenomegaly, lymphadenopathy, oedema of the eyelids and lower extremities, endocrinopathy and skin pigmentation). Therefore, the diagnostic criteria of POEMS syndrome were fulfilled. In addition, the absence of evidence obtained from lymph node biopsy does not exclude the possibility of POEMS syndrome with Castleman disease. 19
Prevalences of the documented features of POEMS syndrome, as recorded during several large retrospective case series.
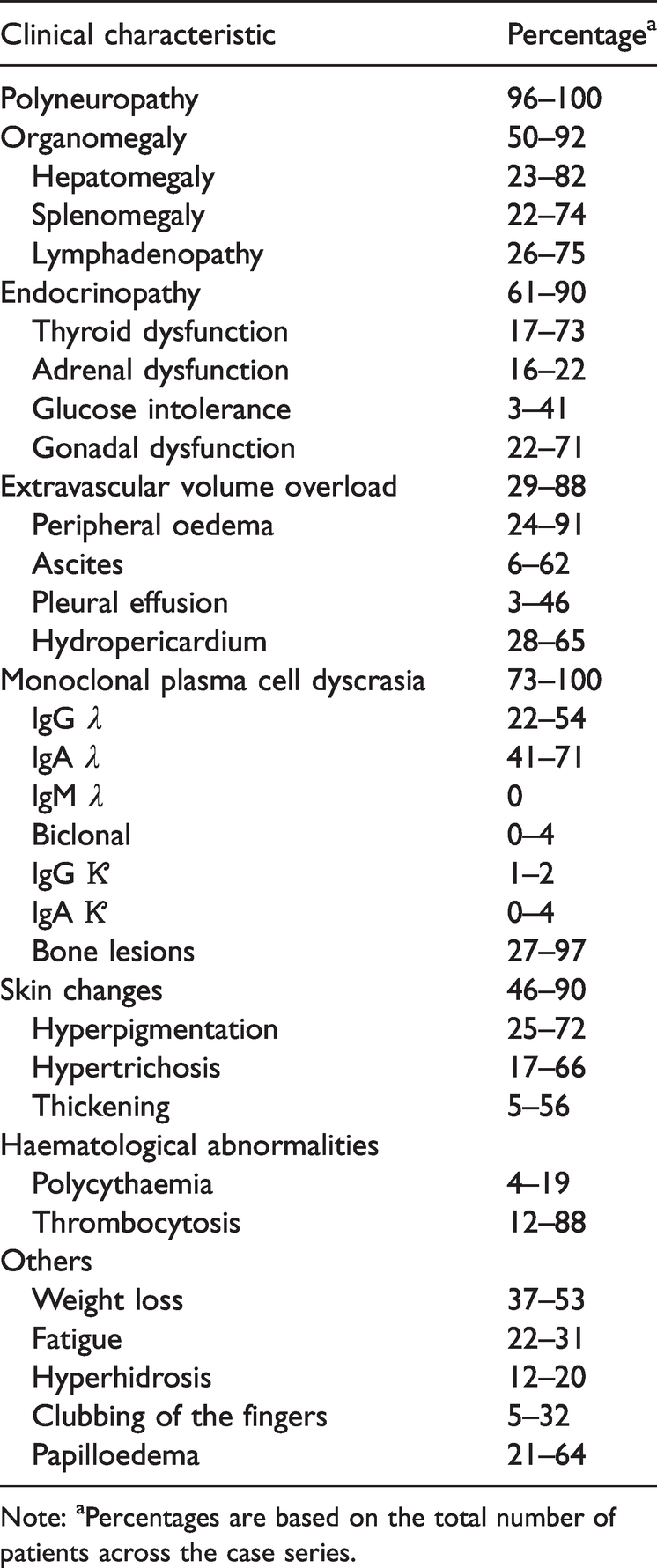
Note: aPercentages are based on the total number of patients across the case series.
Criteria for the diagnosis of POEMS syndrome.

Note: A diagnosis of POEMS syndrome is made when both of the mandatory major criteria, one of the three other major criteria and one of the six minor criteria are met.
POEMS syndrome involves multiple organs and it is caused by the proliferation of monoclonal plasma cells. The pathogenesis of this syndrome is not well understood, but the greater production of VEGF and proinflammatory cytokines by plasma cells is a critical element.20–22 VEGF is a regulator of angiogenesis and osteogenesis that targets endothelial cells and contributes to the ascites, oedema, organomegaly, pleural effusion and neuropathy that characterise the syndrome. VEGF concentration is also associated with disease progression, 23 therapeutic efficacy and survival. 20 However, anti-VEGF therapy alone does not achieve effective clinical remission, 24 suggesting that VEGF contributes to disease progression, rather than being a key cause of POEMS syndrome. Some previous studies have also shown that its pathogenesis may be associated with changes in other inflammatory factors, such as fibroblast growth factor, hepatocyte growth factor, tumour necrosis factor α, interleukin-6, interleukin-12, hypoxia-inducible factor 1α and N-terminal peptide of type I collagen. 25
Endocrinopathies are common in POEMS syndrome, but the exact mechanism is poorly understood. Monika et al. proposed that POEMS syndrome is an antibody-mediated immune disorder. Autopsy results suggest that specific antibodies binding directly to hypophyseal proteins may lead to endocrine disorders. 26 Gandhi et al. reported that 84% of 64 patients with POEMS syndrome had endocrine disease and 54% had multiple endocrine disorders. 27 Two large retrospective studies10,12 showed that 67% to 84% of patients with POEMS syndrome had at least one endocrine system disorder. However, there have been few large-scale analyses of the deficiencies in adrenal function that account for a large proportion of the endocrine abnormalities in POEMS syndrome. We collated the relevant research reports and found that hypogonadism was the most common endocrine abnormality in POEMS syndrome.10,27,28 Male patients tended to have erectile dysfunction and gynaecomastia, while amenorrhoea or menstrual disorders were typical features in female patients.28,29 The second most common abnormality was adrenal insufficiency, followed by hypothyroidism and subclinical hypothyroidism, and finally diabetes or impaired glucose tolerance. Notably, Dispenzieri found that patients with POEMS syndrome and impaired adrenocortical function had a higher mortality rate. 29 The present patient was ultimately diagnosed with POEMS syndrome following an initial diagnosis of Addison’s disease.
Peripheral neuropathy is usually the first symptom of POEMS syndrome, and can sometimes be the only feature of the disease. 4 The typical electrophysiological manifestations are demyelination and axonal degeneration. The severity of axonal loss in the upper and lower limbs varies significantly, but it tends to be more severe in the lower limbs. 30 The most common neurological symptoms are subacute, symmetrical touch-evoked pain and hyperalgesia. These symptoms cannot be alleviated by plasma exchange or plasma immunoglobulin therapy, thereby distinguishing the syndrome from chronic inflammatory demyelinating polyneuropathy. 31 The patient described herein did not present with typical neurological signs, but electromyography showed polyneuropathy of his lower limbs. Therefore, in some patients with suspected POEMS syndrome, even though neurological signs are absent, electrophysiological examination should be performed.
POEMS syndrome is treatable. 18 The key to successful treatment is early recognition, rapid diagnosis and early intervention before the onset of irreversible neurological disease. The treatment of POEMS syndrome involves controlling the development of clonal hematologic diseases by targeting cytokines, such as VEGF and proinflammatory cytokines, and supportive care for the neurological and endocrine system disorders 32 . The evidence for the existing treatment regimens is derived from the results of large retrospective cohort studies and the key treatment modalities are chemotherapy and autologous stem cell transplantation (ASCT).33–35 The chemotherapy regimens include melphalan in combination with dexamethasone, thalidomide/lenalidomide in combination with dexamethasone, and bortezomib in combination with cyclophosphamide and dexamethasone.33–38 Bevacizumab is a monoclonal antibody that targets VEGF24 and can be used in combination with other treatments, such as cyclophosphamide and dexamethasone. 5 Previous studies have shown that the short-term use of bevacizumab, alone or in combination with thalidomide, can act as a bridge to other treatments, such as ASCT. 39
Currently, ASCT is the only treatment that induces nearly 100% remission of clinical symptoms. Systemic chemotherapy can either be used as a long-term treatment or as a maintenance therapy to optimise the physical condition of patients for subsequent ASCT. The median survival time of patients with untreated POEMS syndrome is 33 months. Two recent studies conducted at the Mayo Clinic (N = 291) 40 and by Wang et al. (N = 362) 41 stratified the risk factors for POEMS syndrome and yielded 5-year overall survival rates of 79% and 84%, and 10-year overall survival rates of 62% and 77%, respectively. Three factors were associated with superior overall survival: youth, serum albumin concentration <481.5 µmol/L, and a complete haematological response to treatment. 41
POEMS syndrome is a rare condition that involves multiple systems and is characterised by complex clinical manifestations. The present patient was first diagnosed with Addison’s disease, but after further analysis of his clinical symptoms and signs and targeted auxiliary examinations, he was ultimately diagnosed with POEMS syndrome. The purpose of the present report is to improve awareness of the approaches required for the diagnosis of complex systemic diseases among clinicians in various specialties. Clinicians should involve paying more attention to basic questions, physical examination and the appropriate auxiliary examinations to reduce the incidences of misdiagnosis and missed diagnosis.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Ethics statement
The manuscript was prepared and revised according to the CARE Checklist (2013).
42
Written informed consent was obtained from the patient for the publication of this report and any accompanying images, and the data were de-identified. The Medical Ethics Committee of West China Hospital of Sichuan University exempts the report of a single case from the necessity for ethics approval.
Pigmentation of the patient’s areolae.
Funding
This work was funded by 1?3?5 project for disciplines of excellence?Clinical Research Incubation Project, West China Hospital, Sichuan University (grant number 2021HXFH040).