
Abstract
Synovitis, acne, pustulosis, hyperostosis, and osteitis (SAPHO) syndrome is an umbrella term covering a constellation of bone lesions and skin manifestations, but has rarely been clarified in the clinic. We report a 28-year-old woman who had initial onset of SAPHO syndrome with involvement of the femur, and she experienced a tortuous diagnostic course. We also performed a literature review of SAPHO syndrome cases involving the femur and summarize several empirical conclusions by integrating previous findings with our case. Furthermore, we propose our perspective that ailment of the skin caused by infection of pathogens might be the first hit for triggering or perpetuating the activation of the immune system. As a result, musculoskeletal manifestations are probably the second hit by crosstalk of an autoimmune reaction. The skin manifestations preceding bone lesions can be well explained. Current interventions for SAPHO syndrome remain controversial, but drugs aiming at symptom relief could serve as the first preference for treatment. An accurate diagnosis and appropriate treatment can cure patients in a timely manner. Although the pathogenesis of SAPHO syndrome remains to be determined, physicians and surgeons still need to heighten awareness of this entity to avoid invasive procedures, such as frequent biopsies or nonessential ostectomy.
Keywords
Introduction
In 1987, Chamot et al first described synovitis, acne, pustulosis, hyperostosis, and osteitis (SAPHO) syndrome, which is mainly characterized by osteoarticular disorders and dermatological lesions. 1 Nonspecific inflammation is the major manifestation throughout the whole course of this syndrome.2–5 Some of these patients are still misdiagnosed because of the sparse incidence of SAPHO syndrome and the initial poor interpretation of this syndrome by physicians in the clinic.6,7 Musculoskeletal disorders are the chief complaints commonly presented in patients with SAPHO syndrome.8–10 This rare disease generally involves the anterior chest wall. Therefore, SAPHO syndrome is often observed in the sternoclavicular joints according to a bone scan showing a “bull’s horn” appearance.7,11 Osseous lesions are mainly classified as necrosis, fibrosis, hyperostosis, and aberrant calcification, and these lesions always appear to be the combination of these findings.12,13 The difficulty of diagnosis of this syndrome is increased in patients with only a single bone or skin symptom because symptomatic manifestations of two sites are not merged simultaneously.10,14,15 Moreover, representative cutaneous symptoms with an average rate of 63.5% are ordinary. 16
We report the atypical case of a 28-year-old woman with SPAHO syndrome. In this case, the patient complained of pain in the right thigh as the chief complaint when admitted to the Department of Orthopedics. However, she was ultimately found to suffer from SAPHO syndrome as identified by a series of subsequent examinations. Additionally, we reviewed previously published studies on SAPHO syndrome with femoral involvement with the aim of proposing some analogous features of this syndrome.
Case presentation
A 28-year-old woman was admitted to the outpatient orthopedic clinic in Shandong Provincial Qianfoshan Hospital in September 2016 because of persistent pain in the right outside thigh for 4 months. The reporting of this study conforms to the CARE guidelines. 17 On presentation, the patient complained of considerable soreness in this site without any vagrant pain or ambulation limitations during the most recent week. The symptoms of pain were aggravated with long-term walking and she had insomnia. This pain could be abated by inert activity. She denied a history of trauma or other additional determinate nosogenetic factors, and showed a weight loss of approximately 10 kg since the onset of her symptoms. A physical examination was unremarkable. The extension and flexion of bilateral low extremities were normal.
Magnetic resonance imaging (MRI) showed an abnormal increased signal intensity that appeared on the right upper and middle femur, which suggested a malignant bone tumor (Figure 1). MRI also suggested that the local inner wall of the bone cortex was destroyed and protruded from the periosteum, which appeared to be accompanied by a periosteal reaction. To further investigate the primary malignant carcinoma, an open femoral biopsy (Figure 2a) was performed under general anesthesia. A histopathological examination with hematoxylin and eosin staining showed nonsuppurative osteitis and chronic osteomyelitis (Figure 2b). A blood culture result for bacteria and fungi was negative. Laboratory findings showed an elevated C-reactive protein (CRP) concentration of 55.5 mg/L (normal: <3.48 mg/L) and an erythrocyte sedimentation rate (ESR) of 50 mm/hour (normal: <20 mm/hour) at the second week after admission. Conventional anti-inflammatory strategies were then applied but the outcome was poor. The patient complained of dermatological lesions on both soles, but we did not initially consider that this was related to her other symptoms. A dermatologist was then consulted, and she was diagnosed with palmoplantar pustulosis (Figure 2c). Notably, the patient subsequently mentioned that her toenails were soft with cutaneous deterioration on her soles for the past 4 months (Figure 3a–f). Therefore, these findings suggested SAPHO syndrome, and she was transferred to the Department of Rheumatology. A computed tomography (CT) scan showed hyperostosis of both clavicles with overt cortical sclerosis. A whole-body technetium-99m methylene diphosphonate bone scintigraphy scan demonstrated intense tracer uptake of bilateral sternoclavicular joints, bilateral shoulder joints, the T10 vertebra, bilateral sacroiliac joints, the iliac bone, the hip joint, and bilateral knee joints, which is known as an atypical “bull’s horn” appearance. Additional typical increased uptake in the right proximal femur was also observed (Figure 4a). The patient was subsequently diagnosed with SAPHO syndrome.
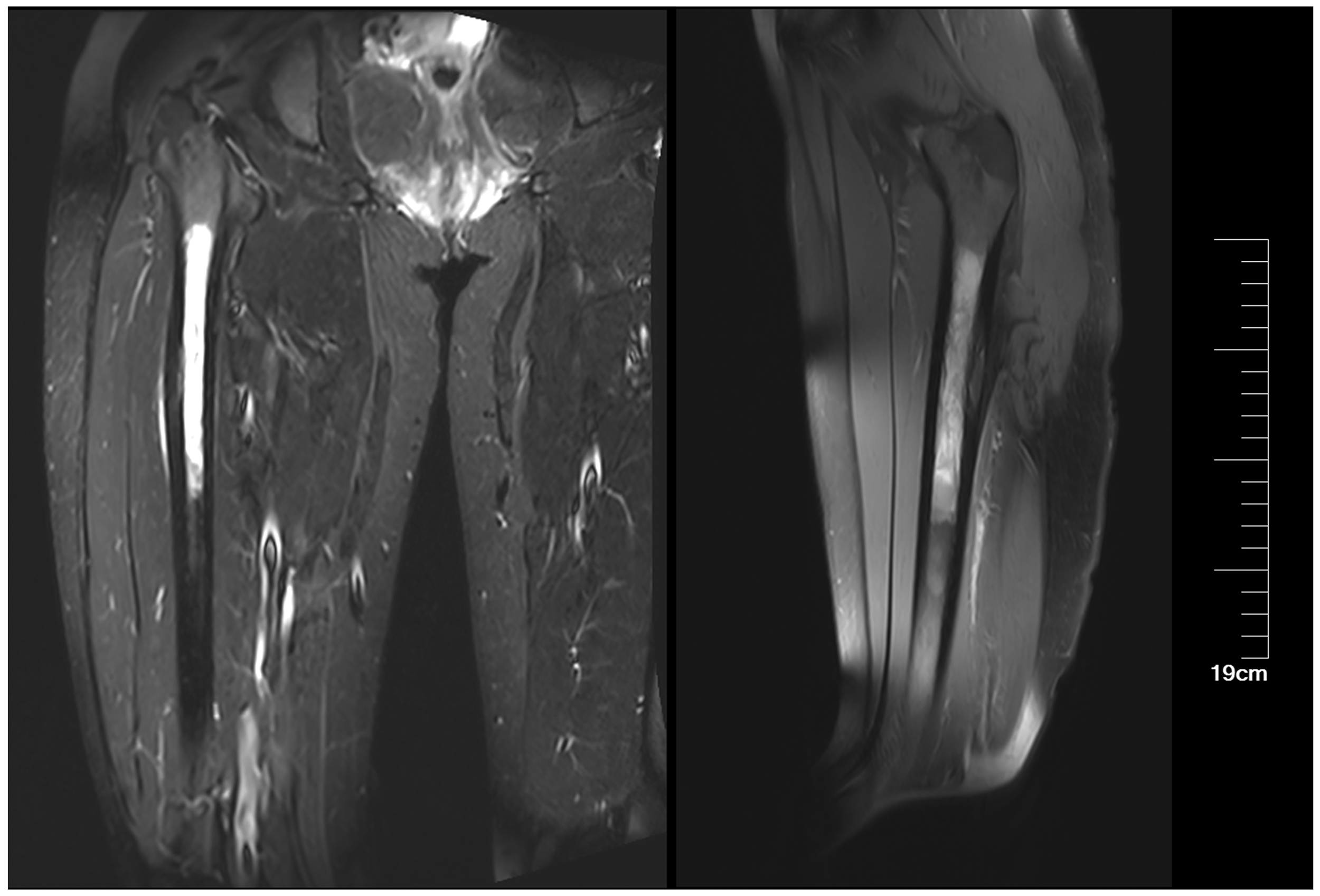
Magnetic resonance imaging shows high abnormal signal intensity in the right proximal femur in the sagittal and coronal positions.

(a) Femoral biopsy. (b) Histopathology shows nonsuppurative osteitis and chronic osteomyelitis (hematoxylin and eosin staining). (c) Dermatopathological results show palmoplantar pustulosis after the patient complained of skin lesions.

Photographs of the whole body. There are mild psoriatic lesions on bilateral palms (a, c) and soles (e, f), and severe collapse of soft nails on the back of both hands can be seen (b, d).

(a) Bone scintigraphy shows intense tracer uptake of bilateral sternoclavicular joints, bilateral shoulder joints, the T10 vertebra, bilateral sacroiliac joints, the iliac bone, the hip joint, and bilateral knee joints. There is also typical increased uptake in the right proximal femur. Concentrations of inflammatory parameters (CRP and ESR) (b) and sera biochemical parameters (HGB and PLT) (c) in the entire course of disease indicate the typical acute inflammatory phase in synovitis, acne, pustulosis, hyperostosis, and osteitis syndrome.
In hindsight, the previous application of conventional anti-inflammatory drugs caused a large reduction CRP concentrations and the ESR (Figure 4b), with a fluctuation in the platelet count and baseline hemoglobin value (Figure 4c). These findings suggested an effect in the acute inflammatory phase. However, this drug treatment failed because the disease still persisted without any symptomatic remission. After the positive diagnosis, the treatment for this patient was palliative and uneventful. For the osseous involvement, she was administered nonsteroidal anti-inflammatory drugs (diclofenac sodium 75 mg/day) orally and received a single intravenous injection of biophosphonates (Aclasta 5 mg). Minocycline hydrochloride (100 mg/day) was prescribed for the treatment of palmoplantar pustulosis. The patient’s condition was gradually ameliorated, and she was finally discharged after relief of her symptoms. There was no evidence of recurrence over the next 6 months. However, she re-visited the hospital owing to the regression of SAPHO syndrome because of her poor compliance with the drug medication after the first 6 months. Her condition has been well controlled for the last 4 years, and her current status is satisfactory.
Discussion
In this case report, we describe an atypical case of SAPHO syndrome with involvement of the femur in a patient with a long diagnostic process. This case was initially suspected as a malignant bone tumor, but this was ruled out by a biopsy. Features for diagnosing SAPHO syndrome were proposed by Nguyen et al. 18 in 2012 and are as follows: 1) osteoarticular manifestations of acne conglobata, acne fulminans, or hidradenitis suppurativa; 2) osteoarticular manifestations of palmoplantar pustulosis; 3) hyperostosis of the anterior chest wall, limbs, or spine with or without dermatosis; and 4) chronic recurrent multifocal osteomyelitis involving the axial or peripheral skeleton with or without dermatosis. These authors emphasized that the diagnosis of SAPHO syndrome should include one of four inclusion features shown above. In this case, the confirmation of SAPHO syndrome was determined from the identification of palmoplantar pustulosis through a detailed medical interview. She was finally discharged after the relief of her symptoms by a symptomatic treatment.
We systematically reviewed the literature to identify all relevant reports of patients with SAPHO with involvement of the femur (1999–2020).14,15,19–23 In summary, 12 of these patients with detailed records and demographic features were identified by consulting previously published studies (Table 1). There were three male patients and nine female patients, with ages ranging from 6 to 68 years old and a female sex predominance. 7
Previous reports of femur involvement in patients with synovitis, acne, pustulosis, hyperostosis, and osteitis syndrome.

*The patient was treated with anti-inflammatory drugs, but other details were not described in this article.
#The pain in this patient disappeared after a biopsy, but the following treatment strategy is unknown.
y, years; F, female; M, male; NA, not available; R, right; L, left; B, bilateral; CT, computed tomography; NSAIDs, non-steroidal anti-inflammatory drugs; MRI, magnetic resonance imaging; GS, glucocorticoid.
Osseous lesions in SAPHO syndrome are commonly found in the anterior chest wall, especially in the sternoclavicular and sternocostal joints.15,24,25 Spinal complaints are the second most common symptom in SAPHO syndrome and lesions are located in axial bone sites. 26 However, peripheral long bone involvement, such as the femur, in SAPHO syndrome is rare. Collectively, unilateral and bilateral femurs could be simultaneously involved. The diaphysis of the femur is the most common site of manifestation, followed by the metaphysis, but the region of the epiphysis appears to be unaffected. Involvement of the femur in SAPHO syndrome comprises various bone lesions, such as hyperostosis, osteomyelitis, bone marrow fibrosis, osteonecrosis, osteolysis, mineralization, osteosclerosis, and bone resorption and formation.14,15,24 In fact, osseous lesions emerging from the femur are a mixture of the above-mentioned factors. In our case, osteomyelitis and cortical sclerosis were found in the right proximal femoral diaphysis. Histological progression can be classified as early, intermediate, and late critical phases during the whole course of SAPHO syndrome. 8 At the beginning of this syndrome, early infiltration of leukocytes inducing an acute inflammatory reaction with concomitant bone marrow edema is difficult to differentiate from infectious osteomyelitis. This gradually progresses to the intermediate phase presenting with bone remodeling and chronic inflammation, and finally leads to bone trabecular sclerosis and prominent bone marrow fibrosis. Our literature review showed that nearly two thirds of femur-involved patients showed the later period of bone lesions when the correct diagnosis was obtained.
Patients with SAPHO syndrome commonly experience a long process of misdiagnosis before an accurate diagnosis because of the deficient perception of physicians or asynchronous skin and bone implications. 27 Accordingly, a differential diagnosis is mainly prone to bone malignancies, bacterial infections, and Paget’s disease.19,28 Our femur-involved case was initially admitted to the Department of Orthopedics and was then thought to be afflicted by a bone tumor. In most previously reported cases, the patients were also first referred to orthopedics specialists and they complained of severe pain in the thigh.14,15,19,20,22 The duration of pain was able to be traced back to several days, months, or years before admission, with no specific duration. Intriguingly, many patients with SAPHO syndrome suffer from preceding skin eruptions, which suggests that cutaneous manifestations appear before musculoskeletal lesions.14,15,19,20,23 Therefore, a fastidious and meticulous medical history interview may help prompt the integration of cutaneous manifestations and musculoskeletal lesions, and would be advantageous to the diagnosis of SAPHO syndrome. Orthopedic surgeons should be aware that a medical history interview could be important during daily clinical work.
The pathogenesis of SAPHO syndrome is still poorly understood because of its enigmatic etiology.13,18 Numerous experimental studies have shown that the development and progression of this entity is induced by multifarious factors of which genetics, environmental effects, and bacterial or viral pathogens might be involved. 29 To date, two major hypotheses of the pathogenesis of SAPHO syndrome have been proposed. One hypothesis postulates that SAPHO syndrome, which is accompanied by untraceable rheumatic indices in patients, is regarded as a latent seronegative spondyloarthropathy.30–32 However, mounting evidence has favored the second hypothesis of infection-mediated autoimmune disorders for the pathogenesis of SAPHO syndrome in the past two decades. 29 Infection-mediated autoimmune disorders have the potential for molecular mimicry, indicating a high homology between cutaneous and osseous components that play a predominant role in the involvement of this syndrome. Our literature review showed that numerous patients initially presented with pustulosis SAPHO syndrome with involvement of the femur.14,15,19,20,23 In these cases, most patients had pustulosis, which may support the second hypothesis. Ailment of the skin caused by infection of a microorganism may be the first hit for triggering or perpetuating activation of the immune system. As a result, musculoskeletal manifestations are probably the second hit by crosstalk of the autoimmune reaction. The issues raised above might explain why several bone biopsies are unremarkable for bacteria and why skin manifestations precede bone lesions. In our case, such proposed concepts were also confirmed in the acute inflammatory phase by evaluating the parameters of CRP and the ESR.
Therapeutic strategies for patients with SAPHO syndrome are palliative and conventional, but diagnosis is difficult because of the complicated pathogenesis of this entity.5,26 Non-steroidal anti-inflammatory drugs as the first-line option have appropriate efficacy in treating SAPHO syndrome by relieving symptoms. 33 Bisphosphonates such as pamidronate effectively inhibit bone resorption and turnover, and have strong anti-inflammatory and lymphopenic effects, which correspond to the feature of new bone formation in SAPHO syndrome. 22 The administration of biological agents could be an effective option to treat the pathological mechanism of SAPHO syndrome. 34 Antibiotic therapy appears to control the skin lesions during the acute phase of this disease. 35 However, in our patient, regression of her disease was observed after she discontinued antibiotics. In patients without acute dermatological manifestations, antibiotic therapy may lose effectiveness in improving SAPHO syndrome. 21 Despite pain often having an extreme influence on the quality of life of patients, SAPHO syndrome usually has an optimal prognosis. 7 Nevertheless, attenuating the effects of the disease burden and deleterious treatment in patients are still a major challenge.
In conclusion, the initial onset of SAPHO syndrome with involvement of the femur is commonly observed in the femoral diaphysis or metaphysis. These patients can be misdiagnosed, especially as malignancy, in the clinic. Current interventions for SAPHO syndrome are still controversial, but drugs aiming at relieving symptoms can serve as the first preference. An accurate diagnosis and appropriate treatment are required for patients with SAPHO syndrome in a timely manner. Physicians and surgeons need to know about the mechanisms of this disease to avoid invasive procedures, such as frequent biopsies or nonessential ostectomy.
Footnotes
Author contributions
Cheng Qiu, Lin Cheng, and Haodong Hou performed the literature review and co-drafted the manuscript. Cheng Qiu, Bohan Xu, Xing Xiao, Zhankui Wang, and Qing Wang participated in diagnosing and treating the patient. Tianyi Liu, Zhankui Wang, and Qing Wang revised the manuscript. All authors approved the final version of the manuscript.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Ethics statement
The study protocol was examined and approved by Shandong Provincial Qianfoshan Hospital, but as this was a retrospective study, the need for approval was waived. The patient participating in the study provided verbal informed consent.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.