
Abstract
Bacteroides caccae is an anaerobic bacterium with a reportedly high isolation rate; however, it rarely causes bloodstream infections. Patients with hypertension are at increased risk of developing anaerobic bacterial infection. In this study, we report a case of bacteremia caused by B. caccae in a patient with renal hypertension and gastrointestinal hemorrhage. This study describes the clinical manifestations of bloodstream infection involving B. caccae to provide guidance for laboratory technicians and clinicians. A 42-year-old Chinese man was admitted for gastrointestinal hemorrhage and subsequently diagnosed with anaerobic blood infection. The pathogenic bacteria isolated from anaerobic blood culture bottles were identified as B. caccae by using an automatic bacterial identification instrument and mass spectrometry (MS). B. caccae is an intestinal opportunistic pathogen that can invade the intestinal mucosa and cause anaerobic bloodstream infection. Two or more sets of blood cultures and MS identification can greatly improve the positive detection rate of blood cultures of anaerobic bacteria. Furthermore, the increased drug resistance of anaerobic bacteria necessitates drug sensitivity tests for anaerobic bacteria in many hospitals. Thus, the early prevention and control of primary diseases with appropriate diagnoses and timely anti-infection therapies are necessary to reduce B. caccae bloodstream infection.
Keywords
Introduction
Bacteroides caccae is a gram-negative anaerobic bacterium without spores. The representative strain of Bacteroides is B. fragilis. 1 B. fragilis is a conditional pathogen that grows in anaerobic environments such as the oral cavity, intestinal tract, and female reproductive tract. 2 It mainly causes endogenous infection, and can invade the human bloodstream and cause bacteremia or septicemia. 3 Bacteremia, or the presence of bacteria in the blood, is an infectious disease with high mortality rates, and it can be directly diagnosed using blood culture. 4 In recent years, multiple cases of bacteremia caused by B. fragilis have been reported. When considered alongside multidrug resistance trends, these cases represent a key development for microbiology and clinical practice, and they should be examined by laboratory technicians and clinicians. 5 , 6 B. caccae is a species that was previously classified in the “Other” category of the Bacteroides genus; however, it is currently being isolated with higher frequency and listed separately. 7 Reports have suggested that B. caccae and outer membrane protein are bacterial targets for immune responses associated with inflammatory bowel disease. 1 In this study, we report a case of bacteremia caused by B. caccae (which was detected using blood culture) in a patient with renal hypertension.
Case presentation
Clinical data
This study was reviewed and approved by the Ethics Committee of Jiangsu Taizhou People’s Hospital, Taizhou, Jiangsu, China. The requirement for informed consent was waived because we de-identified patient details. A 42-year-old Chinese man was hospitalized on November 30, 2018, with a history of uremia and secondary hypertension (renal) for more than 13 years. At the time of hospitalization, he had been undergoing dialysis for right arteriovenous fistula (three times a week on Monday, Wednesday, and Friday), and his blood pressure was controlled by oral drugs. Three hours before admission, the patient exhibited no obvious signs apart from the development of persistent and dull pain (with the sensation of pressure) in the periumbilical and lower abdominal region. The patient also did not experience any diarrhea, nausea, or vomiting. However, he reported experiencing hematochezia twice and observing bright red unformed bloody stool of unknown quantity. He also reported feeling dizzy but did not experience any palpitations, sweating, violent coughs, or syncope. He presented at our hospital for emergency treatment and was admitted for gastrointestinal bleeding. During the course of the disease, no nose or gum bleeding, cold, or fever was observed, and the patient exhibited normal sleep, urinary, and fecal patterns but poor food intake. Furthermore, no recent significant weight loss was reported.
In the physical examination, the patient exhibited clear consciousness and a pale and puffy face, and his abdomen was flat and soft. We did not detect any rash or varicose veins of the abdominal wall or gastrointestinal type and peristaltic wave but observed mild and rebound tenderness around the umbilicus and lower abdomen. The liver, spleen, and ribs were not palpated, and no percussive pain was observed in the liver or kidney area. We observed negative mobile dullness, normal bowel sounds, absence of seismic water sound, external hemorrhoids, and normal external genitalia. The patient’s muscle strength and limb tension were normal. An arteriovenous fistula with palpable tremor was observed in the right upper limb. No edema was observed in the lower extremities. The patient’s physiological and pathological reflex results were normal and negative, respectively, and his meningeal stimulation result was negative.
Admission examination:
The results of the routine blood examination were as follows: red blood cell count, 3.6 × 1012/L; hemoglobin, 117 g/L; erythrocyte specific volume, 35.6%; white blood cell count: 7.85 × 109/L; neutrophil count, 62.4%; and platelet count, 182 × 109/L.
The results of the renal function test were as follows: urea nitrogen, 28.31 mmol/L; and creatinine, 1200.2 mmol/L.
On the day of admission, aerobic and anaerobic blood cultures were each performed in duplicate by using a BACT/ALERT 3D incubator.
Culture and identification
In the aerobic culture, no bacterial growth was observed over 5 days. The anaerobic culture, the blood culture instrument indicated positive results within 28 hours. The culture bottles were removed, and the blood samples were transferred to two blood plates and two chocolate agar plates. One set (one blood plate and one chocolate plate) was cultured in an anaerobic environment (anaerobic bag), whereas the other set was cultured in an aerobic environment. Concurrently, the blood was smeared directly, and gram-negative bacilli were detected through gram-staining microscopy. No bacterial growth was observed in the aerobic culture, whereas bacterial growth was observed in anaerobic culture after 24 hours at 35°C. The colony had a diameter of approximately 1 mm. It was grayish white, translucent, nonhemolytic, moist, and smooth, and it exhibited neat edges (Figure 1A). The colony smear staining indicated gram-negative bacilli of medium size, uneven staining with round and thick staining at both ends, and shallow staining in the middle that exhibited pleomorphism (Figure 1B). An ANC card and VITEC mass spectrometer with VITEC 2 Compact (BioMérieux, Marcy-l’Étoile, France) were used for identification. The identification rates for B. caccae obtained using the VITEC 2 Compact (identification code: 7143507061360) and VITEC mass spectrometer were 98.0% and 99.9%, respectively (Figure 2A). The reporting of this study conforms to CARE guidelines. 8
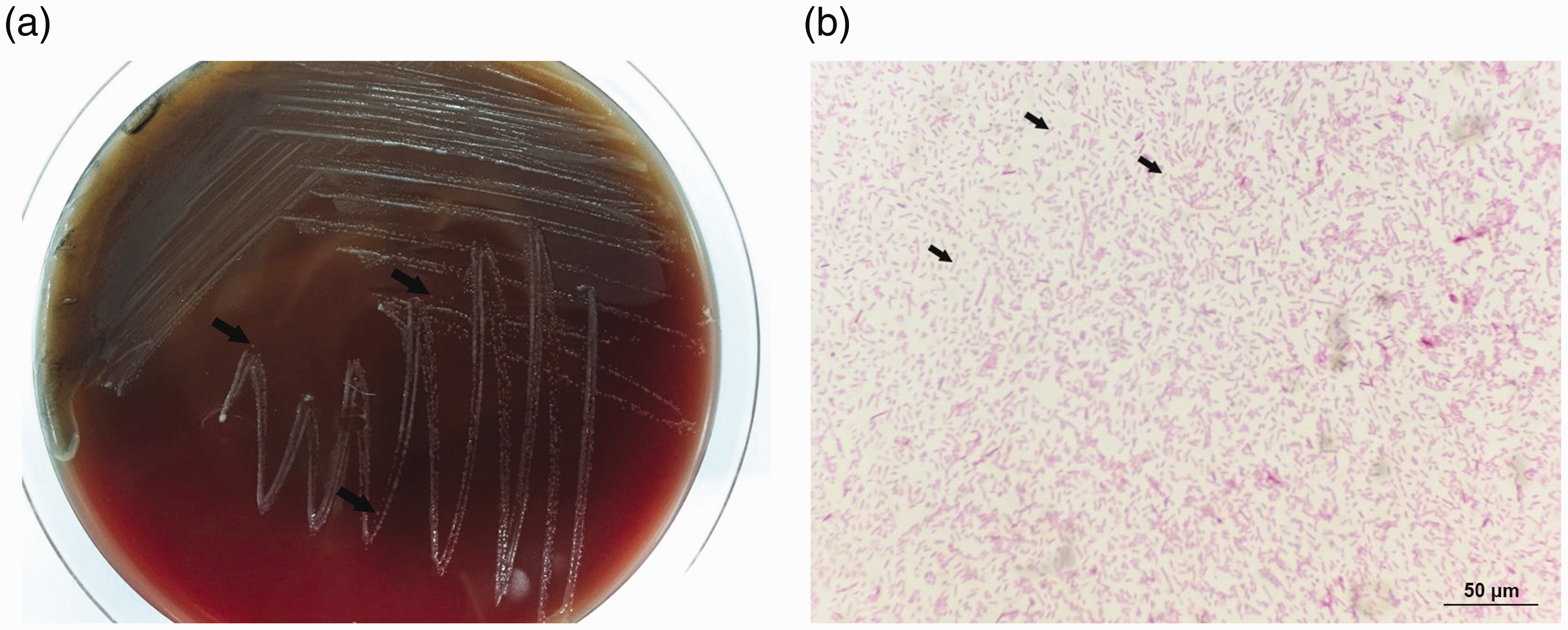
Bacteroides caccae in blood. (a) Colony morphology distribution of Cryptococcus neoformans on a plate. (b) Typical fungal spores under an oil microscope with gram staining.
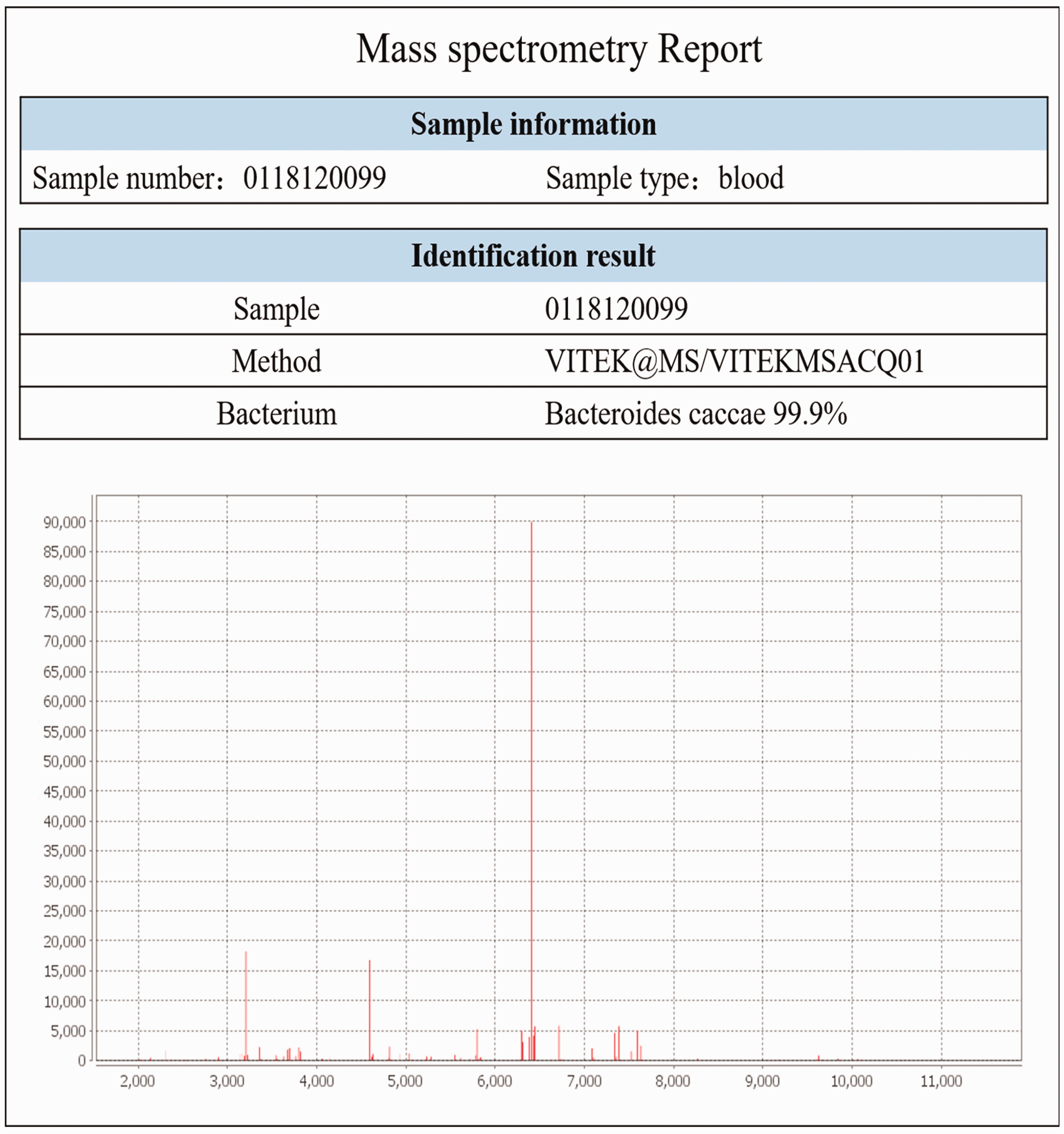
Colony identification through mass spectrometry.
Discussion
Most anaerobic bacteria are harmless or even beneficial to health, particularly Bacteroides species with probiotic effects, which provide multiple benefits for the host.9–12 With the development of medical technology and the aging of the population, the prevalence of anaerobic bacterial infections is increasing because of the increased use of invasive operations, overuse of antibiotics, bodily trauma, tissue ischemia, and necrosis combined with other aerobic bacterial infections; furthermore, the types of drug resistance relating to pathogenic bacteria are changing constantly. 13 , 14 Approximately 50% to 60% of surgical infections observed in clinical practice are related to anaerobes, and blood flow infection caused by anaerobes is particularly severe and associated with high mortality. 15 , 16
Bacteroidetes species are the most common gram-negative obligate anaerobes detected in clinical practice. They exist as normal bacteria in the oral cavity, intestinal tract, and female genital tract of humans and animals, and they are opportunistic pathogens. For example, B. fragilis can cause local tissue infection or abscesses and infections in the female reproductive system, thoracic cavity, and intracranial region. 16 It is the most common anaerobe that causes bacteremia. B. caccae is a member of the B. fragilis group, 17 and it is a major component of the normal flora in the body that colonize the gastrointestinal tract. 18 , 19 It is also a conditional pathogen; therefore, when the intestinal mucosa of the host is damaged, it may invade the blood and cause bloodstream infection. 20 Clinical sepsis caused by bloodstream infection is rare, although B. caccae isolates have been reported. 21 A case of periodontal abscess leading to filamentous Streptococcus infection combined with B. caccae infection was reported by Mark, and an infection caused by B. caccae was recently reported in China. 22 , 23
We have reported the case of a patient with renal hypertension who experienced a bloodstream infection caused by B. caccae. The patient was suspected to have digestive tract tumors and was tested for serum tumor markers. The results for all tumor markers were normal, excluding CYFRA211 (a fragment of cytokeratin 19) and SCCA, for which slightly high levels were obtained. Therefore, the possibility of digestive tract tumors was excluded. Studies have reported that some B. fragilis strains can produce enterotoxin and parenteral enterotoxin, which lead to multiple pathological changes in the intestinal mucosa. 24 The patient had a history of renal hypertension and an even longer history of uremia, and was admitted to our hospital with gastrointestinal bleeding. Our examination revealed an elevated neutrophil gelatinase-related protein level and the presence of hepatitis B. Because of the patient’s complex medical history, long disease course, and severe underlying diseases, normal intestinal flora entered his bloodstream through damaged the intestinal mucosa after intestinal mucosal injury, causing bloodstream infection. The widespread application of antibiotics and presence of immunodeficiencies increase the risk of anaerobic bacteremia caused by opportunistic pathogens invading the bloodstream, and anaerobic bacteremia is becoming a primary cause of death in patients with chronic diseases. 25 Thus, the early prevention and control of primary diseases can reduce the occurrence and development of anaerobic-bacteria bloodstream infection.
The identification of B. caccae can be challenging because the clinical symptoms of B. caccae infections are similar to those of other bloodstream infections. 26 , 27 The use of two or more sets of blood cultures substantially improves the positive testing rate of blood cultures such that patients can receive timely treatment and have a lower risk of death from the condition. 28 The blood samples of our patient exhibited no bacterial growth in the two aerobic blood culture bottles for 5 days; conversely, bacterial growth was detected in the two anaerobic bottles using the automatic bacterial identification instrument after only 28 hours. Therefore, conducting aerobic and anaerobic blood cultures concurrently in clinical practice improves the detection rate of pathogenic bacteria. Our results demonstrated that mass spectrometry is an excellent diagnostic tool for the identification of rare anaerobes such as B. caccae. 29 , 30 The daily blood work revealed positive blood culture results, and bacteria was observed in the gram-staining smear; however, no bacterial growth was observed in the cultures. In such a case, the presence of anaerobic bacteria should be considered. Our experience also alerted us to the essential role of anaerobic cultures in clinical practice.
B. fragilis is widely distributed in clinical specimens, and it requires appropriate antibiotic management for patients with anaerobic infection. Notably, anaerobic bacteria are resistant to various commonly used antibiotics. Among anaerobes, the most common mechanism of antimicrobial resistance to β-lactams is the production of β-lactamase enzymes. 31 The resistance of B. caccae to 5-nitroimidazole is related to its nim gene. 15 , 32 , 33 Carbapenems are widely used in the treatment of clinical infectious diseases and carbapenem-resistant strains of B. fragilis have been identified, which is related to the cfiA gene encoding a metallo-lactamase.34–36 In addition to symptomatic treatment, our patient was administered empirical medication after admission. He initially received a combination therapy of omeprazole sodium and cefodizime, which failed to control the infection. Subsequently, linezolid was added to the medication regimen. However, the severity of the patient’s condition and rapid progression of the disease caused him to reject further rescue therapy. The patient was discharged, and we were unable to ascertain the therapeutic effects of the administered antibiotics. Therefore, hospitals should perform drug sensitivity tests for anaerobic bacteria to increase the precision of treatments.
Given the increasing prevalence of hypertension and presence of primary diseases of poverty in China, anaerobic bacterial infection should be considered in differential diagnosis for patients with hypertension who present with gastrointestinal hemorrhage. The early prevention and control of primary diseases can reduce the occurrence and development of anaerobic bloodstream infection. Furthermore, two or more sets of blood culture greatly improves the positive test rate of blood cultures of anaerobic bacteria, and identification through mass spectrometry can play a role in B. caccae diagnosis. With the increasing drug resistance of anaerobic bacteria, drug sensitivity testing for anaerobic bacteria must be conducted in more hospitals.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605211047277 - Supplemental material for Bloodstream infection caused by Bacteroides caccae in a patient with renal hypertension: a case report
Supplemental material, sj-pdf-1-imr-10.1177_03000605211047277 for Bloodstream infection caused by Bacteroides caccae in a patient with renal hypertension: a case report by Yang Yang, Qingfang Zhang, Haitao Hu, Wenyun Zhang and Taohong Lu in Journal of International Medical Research
Supplemental Material
sj-pdf-2-imr-10.1177_03000605211047277 - Supplemental material for Bloodstream infection caused by Bacteroides caccae in a patient with renal hypertension: a case report
Supplemental material, sj-pdf-2-imr-10.1177_03000605211047277 for Bloodstream infection caused by Bacteroides caccae in a patient with renal hypertension: a case report by Yang Yang, Qingfang Zhang, Haitao Hu, Wenyun Zhang and Taohong Lu in Journal of International Medical Research
Footnotes
Ethics approval and consent to participate
This study was reviewed and approved by the Ethics Committee of Jiangsu Taizhou People’s Hospital, Taizhou, Jiangsu, China. The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Consent to treatment
The patient consented to treatment.
Availability of data and material
All remaining data are available within the article, or available from the authors upon request.
Acknowledgments
We acknowledge the generous support of the Clinical Laboratory Center, Jiangsu Taizhou People’s Hospital, School of Medicine, Jiangsu University. This work was supported by the Natural Science Foundation of Jiangsu Province (H2018072) and Taizhou social development project (TS201623).
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Natural Science Foundation of Jiangsu Province (H2018072) and Taizhou social development project (TS201623).
Authors’ contributions
Conception and design: All authors; Administrative support: QZ, HZ, TL; Provision of study materials or patients: QZ, HZ, TL; Collection and assembly of data: YY, WZ; Data analysis and interpretation: YY, WZ; Manuscript writing: All authors; Final approval of manuscript: All authors. The authors would also like to thank Wallace Academic Editing for the English language editing.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.