
Abstract
Objective
To identify independent risk factors for diabetic neuropathy (DN) in patients with type 2 diabetes mellitus (T2DM).
Methods
We retrospectively analyzed 376 patients with T2DM at the First Affiliated Hospital of Fujian Medical University, China between January 2013 and October 2016. Multivariate logistic regression was used to explore potential risk factors for progression of DN in patients with T2DM. Effect sizes were estimated using odds ratios (ORs) and 95% confidence intervals (CIs).
Results
The prevalence of DN in patients with T2DM was 43.1%. Multivariate logistic regression indicated that retinopathy (OR: 2.755, 95% CI: 1.599–4.746); diabetic nephropathy (OR: 2.196, 95% CI: 1.279–3.772); longer duration of T2DM (OR: 1.081, 95% CI: 1.045–1.120); use of insulin (OR: 1.091, 95% CI: 1.018–1.170); longer history of alcohol consumption (OR: 1.034, 95% CI: 1.010–1.059); and higher blood urea nitrogen (OR: 1.081, 95% CI: 1.009–1.159) were associated with increased risk of DN in patients with T2DM.
Conclusions
Retinopathy, diabetic nephropathy, longer duration of T2DM, use of insulin, longer history of alcohol consumption, and higher blood urea nitrogen were independent risk factors for DN. These findings should be verified in large-scale prospective studies.
Keywords
Introduction
In 2014, the International Diabetes Federation reported that there were approximately 387 million people living with diabetes mellitus (DM) worldwide and that this number could increase to approximately 592 million people by 2035. 1 Diabetic neuropathy (DN) is a major microvascular complication in patients with DM. The most common types of DN include distal symmetrical neuropathy and polyneuropathy. Nearly two-thirds of patients with DM who develop DN have poor quality of life. 2 Previous studies have demonstrated the effects of intensive glucose control on DN progression in patients with type 1 DM.3–5 However, the impact of individual characteristics on DN progression in patients with type 2 DM (T2DM) remains unclear.6,7 There is a need to identify independent predictors of DN progression in patients with T2DM.
A prior study explored the roles of lipid profiles in patients with type 1 DM and found that after 7.3 years of follow-up, DN progression was associated with levels of total cholesterol (TC) [odds ratio (OR) 1.26], low-density lipoprotein (LDL, OR 1.22), and triglycerides (TGs, OR 1.35). 8 These associations remained unchanged after adjusting for hemoglobin A1c (HbA1c) level and DM duration. Another study followed patients with T2DM for 52 weeks and found that plasma TG levels were associated with DN risk, while other factors did not significantly affect DN progression. 9 In the Utah Diabetic Neuropathy Study, plasma TG levels of ≥150 mg/dL in patients with T2DM were associated with increased risk of DN (relative risk 2.3). 10 Moreover, abnormal lipid profiles have been identified as independent risk factors for atherogenic dyslipidemia, which may affect neuropathy progression. 11 Although numerous studies have illustrated the potential roles of patient characteristics in T2DM, independent risk factors for DN progression remains uncertain. Therefore, we performed a retrospective study to explore the potential roles of patient characteristics in the progression of DN in T2DM.
Materials and methods
Population
This study was approved by the ethics committee of the First Affiliated Hospital of Fujian Medical University, China (approval number MTCA, ECFAH of FMU [2015] No. 084). The study was conducted and reported according to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. 12 Between January 2013 and October 2016, a cohort of 376 patients was enrolled in the study after explaining the study purpose and procedures. The requirement for informed consent was waived because of the retrospective nature of the study. The inclusion criteria were T2DM with duration longer than 1 year and age >18 years. The definition of T2DM was based on the World Health Organization guidelines and was confirmed by a clinician. The exclusion criteria were serum creatinine level of >2 mg/dL, alcoholism, stroke, other causes of neuropathy, or loss of the dorsalis pedis artery pulse.
Data collection
The baseline characteristics of patients with T2DM were obtained from electronic medical records. The following information was collected: sex; age; length of hospital stay; retinopathy; diabetic nephropathy; diabetic foot; DM duration; use of biguanide, sulfonylurea, sulfonation-promoting agents, dextranase, thiazolidine, traditional medicines, and insulin; smoking status; alcohol consumption; hypertension; history of fracture; systolic blood pressure (SBP); diastolic blood pressure (DBP); heart rate; body mass index (BMI); alkaline phosphatase (ALP); blood urea nitrogen (BUN); serum creatinine; uric acid; TC (low: <2.9 mmol/L, normal: 2.9–6.0 mmol/L, high: >6.0 mmol/L); TGs (low: <0.6 mmol/L, normal: 0.6–1.7 mmol/L, high: >1.7 mmol/L); high-density lipoprotein (HDL) (low: <0.7 mmol/L, normal: 0.7–2.0 mmol/L, high: >2.0 mmol/L); LDL (low: <2.08 mmol/L, normal: 2.08–3.12 mmol/L, high: >3.12 mmol/L); fasting plasma glucose (FPG); glomerular filtration rate (GFR); urinary protein; HbA1c; and urinary creatinine.
Patients with T2DM were screened for DN using the Michigan Neuropathy Screening Instrument and through nerve conduction studies using an evoked potential recorder (RMS EMG EP MARK-11; RMS, Panchkula, India).13,14 After 8 to 12 hours of fasting, 5 mL of venous blood was collected. Serum creatinine, FPG, GFR, HbA1c, and lipid profiles were assessed. Systems with SYNCHRON CX MULTI™ calibrators (Beckman Coulter, CA, USA) were used along with their respective reagents and methods to assess biochemical parameters. The diagnostic criteria for DN were based on the following parameters: abnormal clinical symptoms, including patient-reported discomfort, pain, or numbness in the lower limbs; Neuropathy Symptom Score (NSS); Neuropathy Disability Score (NDS); nerve conduction velocities; and quantitative sensory test results.15,16 DN was defined as a NDS score of ≥6 or a NDS score of 3 to 5 in conjunction with a NSS score of ≥5.
Statistical analysis
The baseline characteristics of patients were presented as medians and quartiles or as percentages. Continuous variables were compared between groups using Kruskal–Wallis tests because of non-normality. differences between categorical variables were assessed using chi-square or Cochran–Mantel–Haenszel tests. Multivariate logistic regression analyses were used to explore potential risk factors for DN progression in patients with T2DM after adjustment. All P values were two-sided. P values of <0.05 were considered statistically significant. Data were analyzed using IBM SPSS Statistics 19.0 for Windows (IBM Corp., Armonk, NY, USA).
Results
The baseline characteristics of patients are presented in Table 1. Overall, 162 patients with DN (89 men and 73 women) and 214 patients without DN (115 men and 99 women) were enrolled in this retrospective study. The prevalence of DN among patients with T2DM was 43.1%. Significant differences were observed between patients with and without DN in terms of retinopathy (P < 0.001), diabetic nephropathy (P = 0.004), DM duration (P < 0.001), insulin use (P = 0.004), alcohol consumption (P = 0.004), urinary protein (P = 0.049), and urinary creatinine (P = 0.038). No significant differences were observed between patients with and without DM in terms of sex (P = 0.817), mean age (P = 0.939), length of hospital stay (P = 0.190), diabetic foot (P = 0.053), biguanide use (P = 0.753), sulfonylurea use (P = 0.255), sulfonation-promoting agent use (P = 0.063), dextranase use (P = 0.377), thiazolidine use (P = 0.834), traditional medicine use (P = 0.434), smoking status (P = 0.149), hypertension (P = 0.781), history of fractures (P = 0.109), SBP (P = 0.259), DBP (P = 0.685), heart rate (P = 0.739), BMI (P = 0.329), ALP (P = 0.456), BUN (P = 0.067), serum creatinine (P = 0.630), uric acid (P = 0.527), TC (P = 0.689), TGs (P = 0.418), HDL (P = 0.429), LDL (P = 0.153), FPG (P = 0.273), GFR (P = 0.244), or HbA1c (P = 0.208).
Comparison of baseline characteristics between patients with and without diabetes neuropathy.
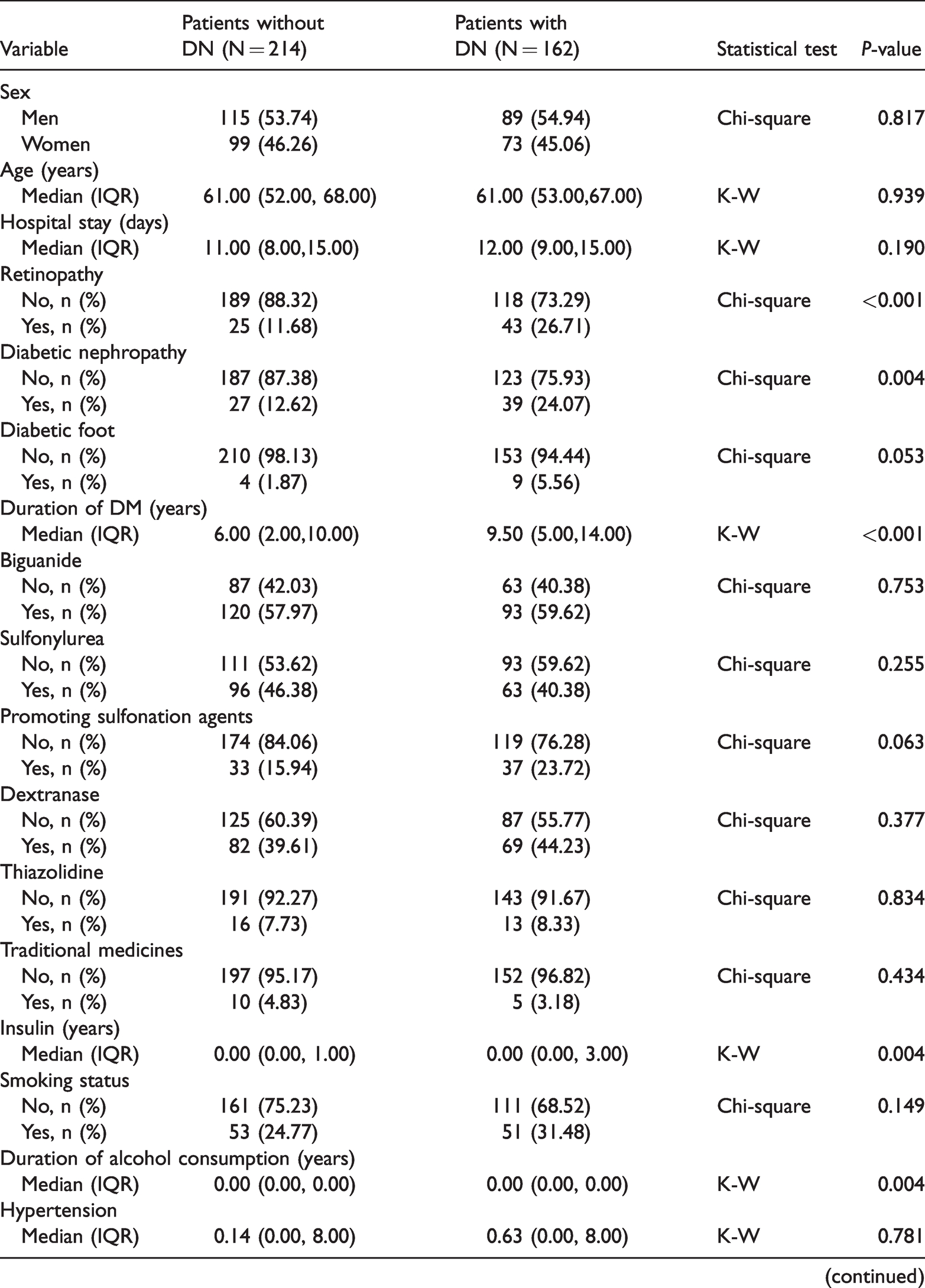
ALP: alkaline phosphatase; BMI: body mass index; DBP: diastolic blood pressure; DM: diabetes mellitus; DN: diabetes neuropathy; FPG: fasting blood glucose; GFR: glomerular filtration rate; HDL: high-density lipoprotein; LDL: low-density lipoprotein; K-W: Kruskal–Wallis; SBP: systolic blood pressure; TC: total cholesterol; TG: triglyceride; IQR, interquartile range; HbA1c, hemoglobin A1c; BUN, blood urea nitrogen; CMH, Cochran–Mantel–Haenszel.
Table 2 summarizes the results of multivariate logistic regression analyses of risk factors for DN progression in patients with T2DM. Independent risk factors for DN in patients with T2DM included retinopathy (OR: 2.755, 95% CI: 1.599–4.746, P < 0.001); diabetic nephropathy (OR: 2.196, 95% CI: 1.279–3.772, P = 0.004); longer duration of DM (OR: 1.081, 95% CI: 1.045–1.120, P < 0.001); use of insulin (OR: 1.091, 95% CI: 1.018–1.170, P = 0.014); longer duration of alcohol consumption (OR: 1.034, 95% CI: 1.010–1.059, P = 0.005); and higher BUN (OR: 1.081, 95% CI: 1.009–1.159, P = 0.028). However, the following factors were not associated with risk of DN in patients with T2DM: sex; age; hospital stay; diabetic foot; use of biguanide, sulfonylurea, sulfonation-promoting agents, dextranase, thiazolidine, and traditional medicines; smoking status; hypertension; history of fracture; SBP; DBP; heart rate; BMI; ALP; serum creatinine; uric acid; TC; TGs; HDL; LDL; FPG; GFR; urinary protein; HbA1c; and urinary creatinine.
Findings of multivariate logistic regression.

OR: odds ratio; CI, confidence interval; DM, diabetes mellitus; SBP, systolic blood pressure; DBP, diastolic blood pressure; BMI, body mass index; ALP, alkaline phosphatase; BUN, blood urea nitrogen; TC, total cholesterol; TG, triglyceride; HDL, high-density lipoprotein; LDL, low-density lipoprotein; FPG, fasting plasma glucose; GFR, glomerular filtration rate; HbA1c, hemoglobin A1c.
Discussion
DN can lead to nerve damage and is associated with increased risks of foot ulcers and foot amputation. The present study included 162 patients with DN and 214 patients without DN. The study population had a broad range of baseline characteristics. The adjusted results of multivariate logistic regression indicated that retinopathy, diabetic nephropathy, longer duration of DM, use of insulin, longer duration of alcohol consumption, and higher BUN were associated with increased risk of DN in patients with T2DM. These factors should be monitored in T2DM patients to prevent progression of DN.
The risk factors for DN identified in this study could be explained by several reasons. First, diabetes complications are significantly associated with severity of T2DM. Because longer duration of DM and use of insulin are associated with severe cases, the prevalence of DN was relatively high in these patients. Second, the effect of alcohol intake on insulin sensitivity and resistance likely contributed to the risk of DN in patients with T2DM. 17 Third, retinopathy and nephropathy are common underlying pathogenic mechanisms in DN. 18
This study did not identify any significant associations between age and risk of DN in patients with T2DM. In contrast, a prior study suggested that age was an independent risk factor for progression of DN in patients with T2DM and was related with accumulation of molecular and cellular damage over time; this axonal damage or demyelination could lead to progression of DN. 19 One potential reason for the lack of association in the present study could be the relatively uniform distribution of age in the study population. Moreover, contrary to our results, Raman et al. found that increased SBP and HbA1c were risk factors for DN in patients with T2DM. 20 One potential reason for this discrepancy could be differences in analytical techniques. Our study treated SBP and HbA1c as continuous variables, whereas Raman et al. stratified patients into SBP and HbA1c categories.
We did not identify any significant associations between plasma lipid profiles and DN in patients with T2DM. Abnormal plasma lipid profiles are associated with the risks of cardiovascular diseases in patients with DM. Furthermore, increased LDL and TC levels are significantly associated with severity of DN. The increased risks of DN associated with lower HDL and higher TG levels and with lower LDL/HDL ratios in patients with type 1 DM have been reported; intensive therapy was shown to effectively reduce the risk of clinical neuropathy by 60%. 3 Moreover, in a case–control study, Booya et al. reported that age, sex, diabetes quality of life, and DM duration were significantly associated with DN progression, whereas high blood pressure, hyperlipidemia, and cigarette smoking were not associated with DN risk. 21 Potential mechanisms underlying the associations between lipid profile and DN risk include insulin signaling in peripheral nerves; however, glucose uptake in the nervous system is largely insulin independent. 22 Higher LDL and TG levels have been associated with faster progression to end-stage renal disease, blindness, and peripheral neuropathy in patients with T2DM. 23 The effects of background therapy with statins or fibrates on lipid profiles could explain our inability to detect associations between plasma lipid profiles and DN in patients with T2DM. Finally, we found that diabetic foot in patients with T2DM was not associated with risk of DN. One potential explanation for this result could be the relatively low proportion of patients with diabetic foot and insufficient power to detect an association.
The present study had several limitations. First, it was designed as a retrospective cohort study, and patients were recruited from a single center. Therefore, selection or recall bias could have affected the results. Moreover, the evidence supporting our conclusions was weaker because of the retrospective design of the study. Second, stratification was not conducted because all patient characteristics were identified. Furthermore, stratified analyses based on the baseline characteristics of the study cohort were not performed because of the limited numbers of patients and wide 95% CIs. Finally, because severity of T2DM in the study cohort was associated with DN progression, this variable should be stratified in future studies.
In conclusion, this study indicated that retinopathy, diabetic nephropathy, longer duration of DM, use of insulin, longer duration of alcohol intake, and higher BUN could increase risk of DN in patients with T2DM. However, the analysis was of a retrospective cohort; therefore, further investigations using large-scale prospective cohort studies should be conducted to verify these results. Furthermore, assessment of the dependence of these associations on patient characteristics may be necessary for better understanding and management of T2DM.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Scientific and Technological Innovation Foundation of Fujian Province (grant numbers 2017Y9091, 2019Y9107, and 2020J01120422).