
Abstract
Delayed neurological deficits secondary to percutaneous vertebroplasty caused by cement leakage is a rare condition. Although cement extravasation during percutaneous vertebroplasty is not uncommon, most cases are clinically asymptomatic, and symptomatic cement extravasation that requires surgical excision is rarely reported. Herein, a case of L4 radiculopathy secondary to cement leakage is reported that involved the delayed onset of neurological symptoms. The patient was treated using a minimally invasive transforaminal endoscopic approach. The clinical and imaging findings and treatment methods are discussed.
Keywords
Introduction
Thoracolumbar osteoporotic vertebral compression fracture (OVCF) is common in older patients and can be managed by conservative or surgical treatment. However, in patients with severe and disabling back pain, it is difficult to achieve satisfactory clinical efficacy using conservative treatment. Percutaneous vertebroplasty (PVP) is a surgical procedure that is widely used in the clinical management of acute OVCF because of its minimal invasiveness and good clinical effects. 1 Nevertheless, the potential for complications is not negligible. For example, cement leakage has been reported to occur in 30% to 65% of patients with osteoporotic vertebral collapse. 2 Although most cases of cement leakage are clinically asymptomatic, cement leakage into the spinal canal or intervertebral foramen can cause canal stenosis as well as spinal cord and nerve root compression.3,4 Cement leakage that results in a neurological deficit often causes immediate symptoms.5–7 Herein, we present a case of L4 radiculopathy secondary to PVP cement leakage that involved the delayed onset of neurological symptoms, without any deficits in the immediate postoperative period. The patient was treated using a minimally invasive transforaminal endoscopic approach. This case report conforms to the CARE guidelines (for CAse REports). 8
Case report
An 82-year-old man who had been previously diagnosed with osteoporosis was admitted to our hospital with L2 to L4 compression fractures without neurological deficits. The PVP procedure was planned as the treatment. The patient agreed to the treatment and signed his informed consent before the operation. Three segment PVPs were performed under local anesthesia for the L2 to L4 vertebral compression fractures. The operative course was uneventful and the patient’s lumbar back pain was improved immediately after surgery. C-arm fluoroscopy during injection did not detect any leakage of cement into the spinal canal. X-ray imaging demonstrated the filling of the vertebral body 1 day after the operation (Figure 1). The patient was discharged after 2 days. One week postoperatively, the patient began to complain of severe right leg pain radiating to the hip, anterior thigh, and medial aspects of the knee and calf. Neurological examination revealed a loss of sensation in the right L4 dermatome, accompanied by a muscle strength grading of 3/5 (weakness) in the right quadriceps. A lumbar computed tomography (CT) scan demonstrated that cement fragments had leaked into the spinal canal, especially in the lateral recess. The caudal spread of the cement leak along the epidural plexus is shown in a sagittal reconstruction image (Figure 2). The patient’s symptoms were relieved with steroid and anti-inflammatory drug therapy in the short term, but returned when he stopped drug therapy. The patient still complained of intermittent radiating pain in the right lower extremity after 1 month of conservative treatment; hence, a minimally invasive transforaminal endoscopic procedure was performed.
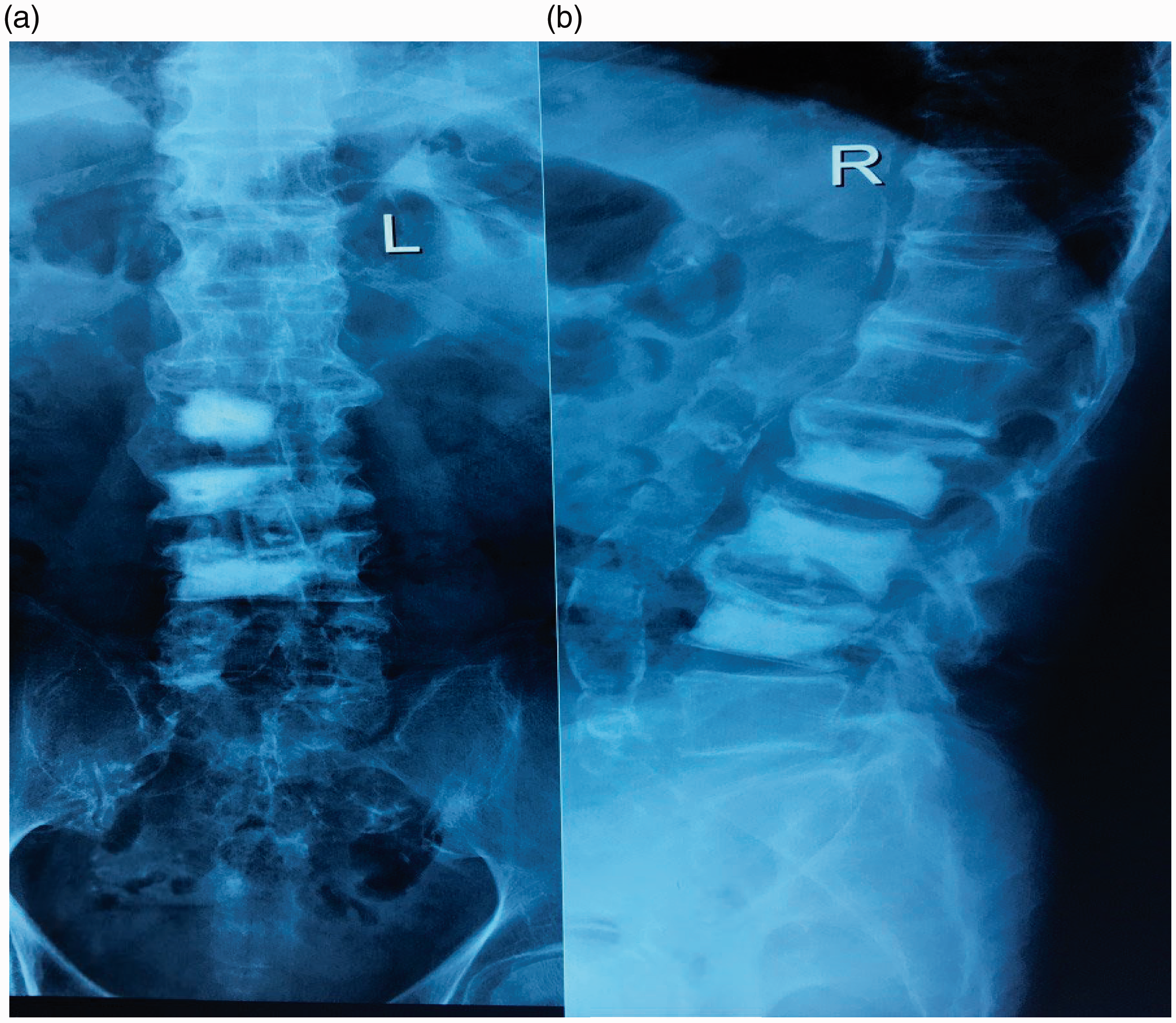
Anterior–posterior (a) and lateral (b) views of lumbar spine X-ray, demonstrating good filling of the vertebral body after percutaneous vertebroplasty, with no cement leaking into the spinal canal.

Preoperative sagittal reconstruction (a) and axial (b) computed tomography scan demonstrating cement leaking into the spinal canal, extending caudally along the epidural venous plexus, and in the lateral recess (red arrow).
The patient was placed in the left lateral position on a radiolucent table, and surgery was performed under local anesthesia. The TESSYS endoscopic system (Joimax GmbH, Karlsruhe, Germany) was used for the surgery. Intermittent fluoroscopic guidance allowed for lateral and anterior–posterior views, which facilitated the insertion of an 18-gauge needle downward into the neuroforamen, with the tip slipping along the neck of the superior articular process. Next, the needle was replaced with a 2.5-mm guiding rod, and sequential dilators were placed over this rod. Sequential reamers were used to enlarge the neural foramen by removing the ventral aspect of the superior articulating process of L4. The working channel was then placed over the sequential dilators, the dilators were removed, and the endoscope was introduced. Lateral and anterior–posterior fluoroscopy views were observed to ensure that the working channel was correctly placed. Under endoscopic visualization, the right L4 nerve root was identified on the medial side, and the bone cement that compressed the nerve root was observed on the lateral side. The cement fragment close to the lateral aspect of the right L4 nerve root in the lateral recess was taken as the cause of the patient’s right L4 radicular symptoms (Figure 3). The right L4 nerve root and bone cement were separated using a hook, and the bone cement was isolated and removed piecemeal using bone punches. Figure 4 shows the decompressed right L4 nerve root, which traversed freely in the epidural space. The removed cement fragment is shown in Figure 5. A sagittal reconstruction image shows the osteotomized state of the right superior articular process after endoscopic partial facetectomy (Figure 6). The cement fragment in the spinal canal had been removed in this postoperative sagittal reconstruction image.
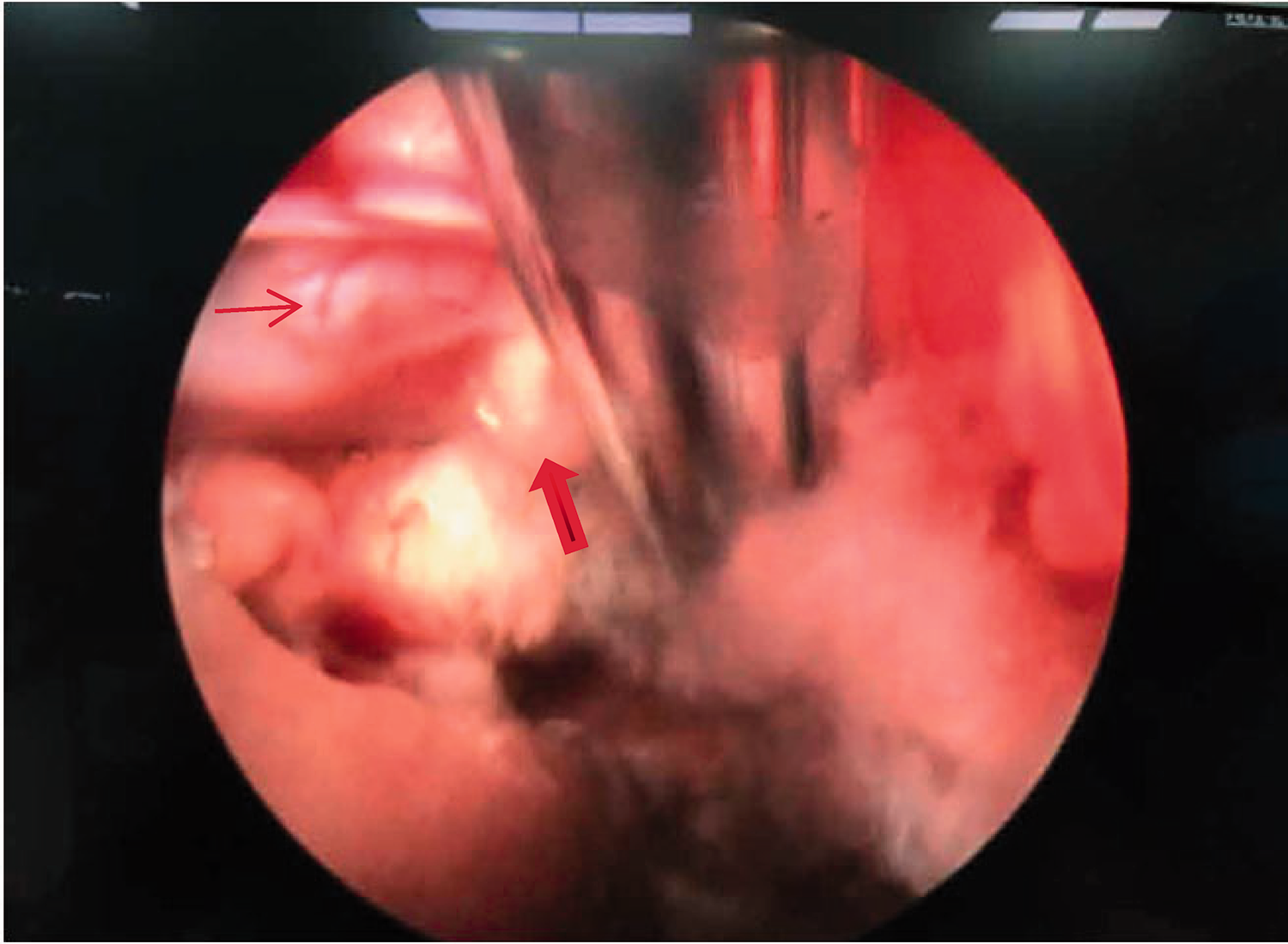
Endoscopic view of the cement fragment and L4 nerve root, showing the cement fragment close to the upper lateral aspect of the right L4 nerve root. The thick red arrow indicates bone cement, while the thin red arrow indicates the right L4 nerve root.

The decompressed right L4 nerve root traversing freely in the epidural space. The red arrow shows the right L4 nerve root.

Free cement fragment after removal.

Postoperative sagittal reconstruction computed tomography scan showing the osteotomized state of the right superior articular process (red arrow) (a). The cement fragment in the spinal canal has been removed (b).
Following endoscopy, the patient’s pain improved immediately, and his muscle strength increased gradually. The patient was discharged after 3 days. After 1 month, his neurological deficits had normalized. At the 6-month follow-up, the patient was pain-free without any neurological deficits.
Discussion
Although PVP and kyphoplasty are widely used for the treatment of OVCF, their effectiveness remains controversial. In 2009, Kallmes et al. 9 and Buchbinder et al. 10 reported that vertebroplasty was no better than a sham procedure in randomized controlled trials. Anderson et al. 11 then presented conflicting data in a meta-analysis of vertebroplasty compared with the nonsurgical management of OVCF. The results of this meta-analysis suggested that cement augmentation is a valid treatment option for a specific subset of patients with OVCF. In a review of the topic, Savage et al. 12 concluded that vertebroplasty is worth considering for patients with acute vertebral compression fractures, as evidenced by edema on magnetic resonance imaging (MRI). The case in the present report also had acute compression fractures, and in accordance with the recommendations of Savage et al., the acuity of these compression fractures was confirmed using MRI.
The major complications of PVP are related to the leakage of cement. The majority of studies have described cement extravasation as being asymptomatic in most cases. Even if cement occupies about 25% of the spinal canal, it is possible that no neurological complications occur. 13 However, neurological complications have been infrequently reported with percutaneous cement augmentation procedures.14,15 Moreover, most neurological lesions occur immediately after such procedures.5–7,16,17 From 2007 to date, only three incidents of delayed symptomatic lesions have been reported in the literature. Cosar et al. 18 reported one delayed neurological lesion event in seven cement leakage cases after vertebroplasty. In this case, a subligamentous cement leak was observed during the cement injection, but patient did not present neurological deficits immediately after the operation. One day postoperatively, the patient reported mild pain extending to the right leg, without any motor deficits. The control images revealed cement leakage into the right neural foramen between the L3 and L4 vertebrae. In this patient, steroid treatment was administered and the pain was resolved after 6 hours. In addition, Ross et al. 19 reported two cases with delayed symptomatic lesions after kyphoplasty or vertebroplasty. One of the patients underwent vertebroplasty and had a significant improvement in pain after the procedure. However, 3 days later, he presented intermittent, severe pain that radiated into the right leg, as well as numbness. A CT scan showed aberrant bone cement in the spinal canal, and laminectomy was then performed to remove the epidural and intradural bone cement. In both cases, the delayed neurological lesions were directly associated with cement leakage. Patel et al. 20 also reported a series of cases with neurological deficits following percutaneous vertebral stabilization. However, the delayed onset of neurological deficits was associated with persistent spinal instability and further fracture fragment displacement, displacement of the implanted cement, or a new vertebral body fracture occurring at either the treated level or another level.
In the present case, no cement leakage was noted during the cement injection under C-arm fluoroscopy, and the patient’s lumbar back pain was improved immediately after the surgery. Postoperative X-rays did not reveal any cement leakage. However, the patient began to complain of severe radiating pain in the right leg 1 week after surgery. A CT scan showed cement leakage in the spinal canal, located in the right L4 lateral recess. The early detection of a leak is difficult using C-arm fluoroscopy or lateral radiographs, especially when there is relatively little cement leakage. Furthermore, the quality of images using C-arm fluoroscopy is worse than that of plain radiographs. Thus, leaks into the spinal canal may be missed. However, C-arm fluoroscopy is the only means by which cement leakage can be monitored during an injection. Nonetheless, in clinical practice, cement leakage should be suspected in patients who develop uninterpretable symptoms with delayed onset after vertebroplasty. A CT or MRI scan may be necessary to arrive at the correct diagnosis. In the current case, cement spread along the epidural plexus, and was a type B leakage according to the classification by Yeom et al. of cement leakage patterns. 13 Type B leaks do not usually cause neurological complications because the distribution of the cement resembles that of normal local venous engorgement. Whether cement leakage causes neurological lesions depends on the location of extravasated cement, the amount of extruded cement, and the rate of cement injection. 21 Although the leakage was relatively small in our case, cement was present in the lateral recess, adjacent to the L4 nerve root. This phenomenon was similar to that of osteophytes pressing on a nerve root, thus resulting in lateral recess stenosis and causing neurological symptoms.
In previous studies, decompression with or without stabilization has been recommended for cases of symptomatic cement leakage.19,22 In some cases, neurological deficits were associated with persistent spinal instability, such as the displacement of fracture fragments or the implanted cement. In such cases, decompression surgery and spinal reconstruction are necessary. 23 However, because OVCF commonly occurs in older patients because of its degenerative nature, we should consider its invasiveness, prolonged surgical durations, and large amounts of blood loss during surgery, as well as the surgical risks associated with spinal instrumentation, such as surgical site infection, screw misplacement, screw loosening, and adjacent segment diseases. 24 Less invasive procedures might therefore be favorable because they avoid the potential risks associated with spinal instrumented fusion. Wagner et al. 25 presented a minimally invasive transforaminal endoscopic solution for PVP and kyphoplasty cement leakage, and their patient’s pain was improved immediately after the surgery. Senturk et al. 26 also presented a minimally invasive endoscopic translaminar technique for removing cement leakage fragments after the PVP procedure. Subsequently, their patient’s complaints were resolved completely. The current case also highlighted the effectiveness of minimally invasive techniques in the treatment of intraspinal cement leakage after PVP.
Medical practitioners need to remember that the neurological complications of vertebroplasty do not always manifest immediately after the procedure. Moreover, plain X-rays might not reveal aberrant bone cement. Our experience with the present case suggests that patients with delayed neurological deficits caused by cement leakage can be treated using a minimally invasive procedure and experience good outcomes.
Footnotes
Ethics statement
No ethical approval was required for this case report. Patient details were de-identified; therefore, patient consent for publication was not required.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.