
Abstract
Objective
To investigate the relationship between angiotensin (AGT) rs2493132 gene polymorphism and the risk of developing non-alcoholic fatty liver disease (NAFLD) and coronary artery disease (CAD) in the Chinese Han population.
Methods
Polymerase chain reaction was performed to determine AGT genotypes. Anthropometric and clinical data were investigated and statistically analyzed in the clinical laboratory department of Qingdao Municipal Hospital.
Results
The AGT rs2493132 CT + TT genotype was an important risk factor for CAD in patients with NAFLD and NAFLD + CAD in healthy controls. The AGT rs2493132 T allele increased the risk of NAFLD + CAD in healthy controls. The AGT rs2493132 CT + TT genotype and T allele also significantly increased the risk of CAD in patients with NAFLD after adjustments for age, sex, and body mass index. In addition, AGT rs2493132 T allele carriers showed higher total cholesterol (TC) and low-density lipoprotein (LDL) levels compared with non-carriers.
Conclusions
The AGT rs2493132 CT + TT genotype and T allele significantly increased the risk of developing CAD in patients with NAFLD in the Chinese Han population. The AGT rs2493132 T allele was associated with increased serum TC and LDL levels.
Keywords
Introduction
Non-alcoholic fatty liver disease (NAFLD) is the most prevalent form of chronic liver disease, with an estimated prevalence as high as 29.62% in the Asian population. 1 As a hepatic manifestation of metabolic syndrome, NAFLD has been shown to be an independent risk factor for cardiovascular disease (CVD).2–5 The occurrence rate of coronary artery disease (CAD) has increased by 4.7-fold in adults with NAFLD, and the severity of CAD is significantly associated with the presence of NAFLD. 6 Multiple factors contribute to the pathogenesis of NAFLD and CAD. 7 Accumulated evidence suggests that gene polymorphism is an important risk factor not only for the occurrence of NAFLD or CAD in the general population but also for the incidence of CAD in patients with NAFLD.3,8 Simons et al. investigated the effect of three variants in NAFLD susceptibility genes on the risk of developing CAD in patients with NAFLD. 9 The results showed that some variants provided a protective effect for the development of CAD, whereas others exerted a neutral effect on CAD risk. Glucokinase regulatory protein (GCKR) participates in de novo lipogenesis, and previous case-control studies suggested that GCKR rs780094 was significantly related to NAFLD.10,11 A recent meta-analysis (including 274,625 individuals) demonstrated a significant association between GCKR rs780094 and the risk of CAD. 12 Therefore, the different effects of gene polymorphisms on plasma lipids may be a vital mediator between NAFLD and the risk of CAD. 3
Angiotensinogen (AGT) plays an essential role in blood pressure regulation.13–15 In addition, AGT is potentially involved in metabolic disorders. 14 , 16 For example, Tao et al. found that hepatocyte-specific AGT deficiency protected mice from western diet-induced liver steatosis and insulin resistance. 16 Recently, several clinical studies have reported a relationship between AGT gene polymorphism and the regulation of serum lipid metabolism. The AGT rs699 CC genotype was found to be significantly associated with high-density lipoprotein (HDL) levels in patients with peripheral arterial diseases. 17 Khamlaoui et al. reported that the AGT M235T genotype was associated with the serum levels of low-density lipoprotein (LDL) and total cholesterol (TC) and increased the risk of overweight-obesity. 18 Ji et al. suggested that AGT rs2493132 was associated with hypertension in the Chinese Han population, indicating that this polymorphism might be a risk factor for CAD. 19
Although the association of AGT gene polymorphisms with serum lipid metabolism and CAD has been investigated in several studies, the exact relationship between AGT gene polymorphism and the risk of NAFLD and CAD remains unclear. This study was designed to investigate the effect of AGT rs2493132 on the risk of developing NAFLD and CAD in the Chinese Han population and determine the influence of AGT rs2493132 on serum lipid profiles.
Materials and methods
Study subjects
This study was approved by the Ethics Committee of Qingdao Municipal Hospital (approval number: 2017LSZD20) and conducted in accordance with the principles of the Helsinki Declaration and its appendices. 20 All participants filled out an informed consent form before this study. From July 2017 to December 2018, patients with NAFLD and CAD (NAFLD + CAD), patients with NAFLD only, and healthy controls were recruited at Qingdao Municipal Hospital. The diagnosis of NAFLD was based on the guidelines of the American Association for the Study of Liver Disease. 21 CAD was diagnosed by a percutaneous coronary angiography and defined as ≥50% stenosis in at least one coronary artery. Subjects with other liver diseases, such as autoimmune hepatitis, drug-induced hepatitis, viral hepatitis, hepatocellular carcinoma, were excluded from this study.
Biochemical analyses
Demographic characteristics (age and sex) were assessed by a questionnaire, and anthropometric parameters (height and weight) and blood pressure were measured using standard methods. Body mass index (BMI) was calculated as weight (kg)/height (m) 2 . Blood samples were collected from each subject’s median vein for biochemical analysis following 12 hours of fasting. Serum aspartic aminotransferase (AST), alanine aminotransferase (ALT), alkaline phosphatase (ALP), gamma-glutamine transpeptidase (GGT), triglyceride (TG), TC, HDL, LDL, and fasting blood glucose (FPG) were detected in the clinical laboratory department of our hospital.
Genomic DNA extraction and genotyping
Genomic DNA was extracted from ethylenediaminetetraacetic acid-anticoagulated whole blood using a TIANamp Blood DNA Kit (Tiangen Biochemical Technology, Beijing, China) and stored at −20°C until use. AGT rs2493132 was genotyped by polymerase chain reaction with the corresponding primers 5ʹ-
Statistical analysis
All analyses were performed using IBM SPSS Statistics for Windows, Version 21.0 (IBM Corp., Armonk, NY, USA). The Pearson’s χ2 test was used to analyze the Hardy–Weinberg equilibrium in the distributions of genotypes among subjects. Continuous variables were compared by an unpaired Student’s t-test and expressed as the mean ± standard deviation when normally distributed. Categorical variables were compared using the Chi-square test. The association between AGT rs2493132 and the risk of NAFLD and NAFLD + CAD was determined by calculating the crude and adjusted odds ratios (ORs) and 95% confidence intervals (CI) from the logistic regression analyses. Statistical significance was considered at P < 0.05.
Results
Clinical characteristics of the study population
The clinical characteristics of 142 patients with NAFLD (mean age: 40.95 ± 5.96 years), 109 patients with NAFLD + CAD (mean age: 59.05 ± 7.95 years), and 246 healthy controls (mean age: 47.40 ±11.52 years) were summarized in Table 1. Patients with NAFLD had higher BMI, ALT, AST, GGT, TG, systolic blood pressure (SBP), and diastolic blood pressure (DBP) than the healthy controls (all P < 0.05). Additionally, patients with NAFLD + CAD exhibited higher BMI, ALT, ALP, TG, and SBP and lower serum levels of TC, HDL, and LDL compared with the healthy controls (all P < 0.05). Last, patients with NAFLD + CAD had lower BMI, GGT, TC, HDL, and LDL and higher serum ALP levels and SBP than patients with NAFLD (all P < 0.05).
Basic characteristics of the study population.
P1, NAFLD group vs control group; P2, NAFLD + CAD group vs control group; P3, NAFLD + CAD group vs NAFLD group.
BMI, body mass index; ALT, alanine aminotransferase; AST, aspartate aminotransferase; GGT, gamma-glutamine transpeptidase; ALP, alkaline phosphatase; FPG, fasting blood glucose; TG, triglyceride; TC, total cholesterol; HDL, high-density lipoprotein; LDL, low-density lipoprotein; NAFLD, non-alcoholic fatty liver disease; NAFLD + CAD, NAFLD with coronary artery disease; SBP, systolic blood pressure; DBP, diastolic blood pressure.
Genotypes and allele distribution of AGT rs2493132
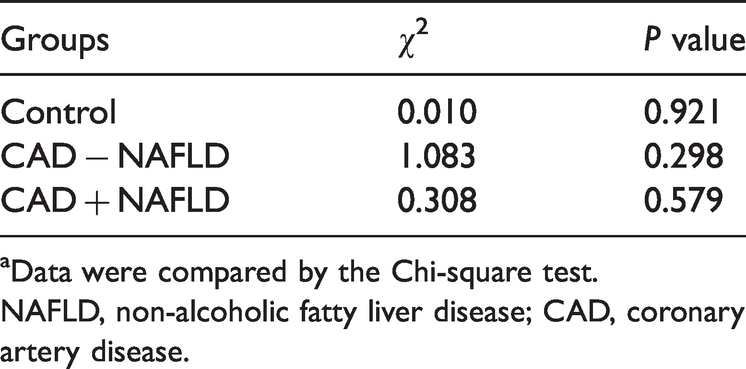
The genotype distributions of AGT rs2493132 in the healthy control, NAFLD, and NAFLD + CAD groups were confirmed to be in Hardy–Weinberg equilibrium (Table 2). There was no significant difference in the genotype distributions of AGT rs2493132 between the NAFLD and healthy control groups or between the NAFLD + CAD and NAFLD groups. In addition, the distributions of the AGT rs2493132 allele between the NAFLD and healthy control groups and between the NAFLD + CAD and NAFLD groups were not significantly different. However, the genotype and allele distributions of AGT rs2493132 between the NAFLD + CAD and control groups were significantly different (P = 0.048 and P = 0.015, respectively) (Table 3). The results of logistic regression analysis suggested that the AGT rs2493132 CT+TT genotype was an important risk factor for CAD in patients with NAFLD (OR = 1.785, 95%CI: 1.061–3.003, P = 0.029) and NAFLD + CAD in healthy controls (OR = 1.738, 95%CI: 1.082–2.793, P = 0.022). The AGT rs2493132 T allele did not show a significant association with the risk of CAD in patients with NAFLD but did increase the risk of NAFLD + CAD in healthy controls (OR = 1.501, 95%CI: 1.081–2.084, P = 0.015). After adjustments for age, sex, and BMI, both the AGT rs2493132 CT+TT genotype and T allele were identified as significant risk factors for the development of CAD in patients with NAFLD (OR = 4.718, 95%CI: 1.502–14.824, P = 0.008; OR = 2.436, 95%CI: 1.184–5.011, P = 0.016, respectively) (Table 4).
Results of the Hardy–Weinberg Equilibrium analysisa.
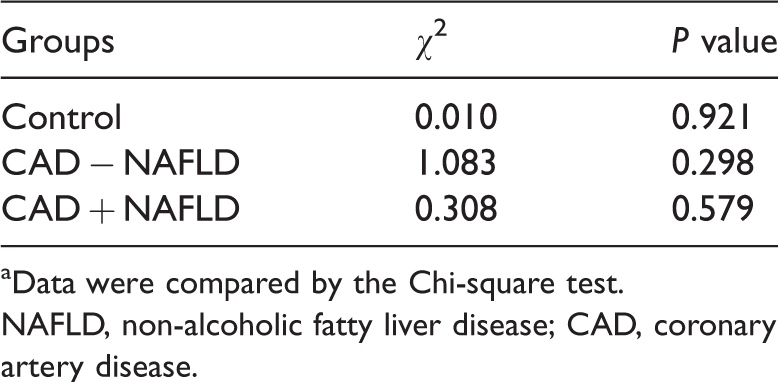
aData were compared by the Chi-square test.
NAFLD, non-alcoholic fatty liver disease; CAD, coronary artery disease.
Distribution of AGT rs2493132 genotypes and alleles in the study group.

P1, NAFLD group vs control group; P2, NAFLD + CAD vs NAFLD; P3, NAFLD + CAD vs. control group.
NAFLD, non-alcoholic fatty liver disease; CAD, coronary artery disease.
Odds ratios according to AGT rs2493132 genotypes in the study group.

aBinary logistic regression model was used for the adjustment of age, sex, and body mass index.
OR, odds ratio; CI, confidence interval; P1, NAFLD group vs control group; P2, NAFLD + CAD vs NAFLD; P3, NAFLD + CAD vs. control group.
Association of the AGT rs2493132 polymorphism with clinical characteristics in the overall patient series
To investigate the effect of AGT rs2493132 polymorphism on the clinical parameters of the enrolled subjects, we compared the differences in clinical parameters of the AGT rs2493132 T allele carriers and non-carriers among all patients. As shown in Table 5, the serum levels of TC and LDL in the T allele carriers were higher than those in non-carriers (P = 0.045 and 0.044, respectively). There was no significant difference in the other parameters, such as ALT, AST, GGT, ALP, TG, or HDL, between the T allele carriers and non-carriers. The above results suggest that the AGT rs2493132 T allele variant may increase serum TC and LDL levels in the general population.
Clinical characteristics of AGT rs2493132 T allele carriers and non-carriers in the overall study group.
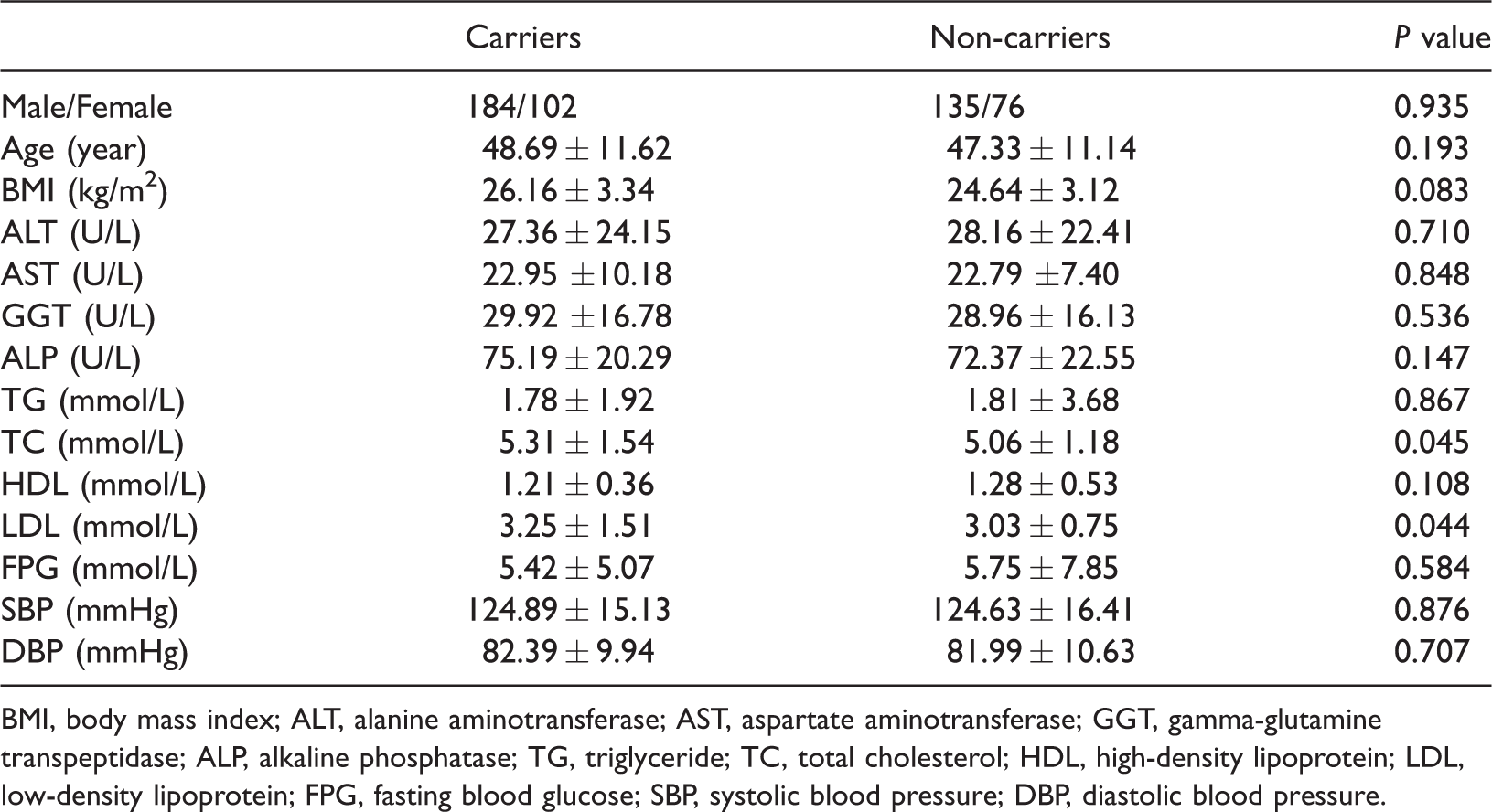
BMI, body mass index; ALT, alanine aminotransferase; AST, aspartate aminotransferase; GGT, gamma-glutamine transpeptidase; ALP, alkaline phosphatase; TG, triglyceride; TC, total cholesterol; HDL, high-density lipoprotein; LDL, low-density lipoprotein; FPG, fasting blood glucose; SBP, systolic blood pressure; DBP, diastolic blood pressure.
Discussion
NAFLD is a multisystem disease and is significantly associated with the risk of CVD. 22 Previous studies demonstrated that NAFLD is an independent risk factor for CAD, and CAD is the leading cause of death among patients with NAFLD. 2 , 4 , 22 In a study conducted in Korea, Lee et al. showed that NAFLD was an independent predictor of CAD, and the presence of coronary artery stenosis was significantly correlated with fatty liver disease in a grade-dependent manner (P = 0.025). 23 Accumulated studies have demonstrated that gene polymorphisms are significant risk factors for NAFLD and CAD. In the Chinese Han population, Liu et al. reported that genetic variants of tribbles-1 rs17321515 increased the risk of CAD in patients with NAFLD. 24 Cheng et al. showed that tumor necrosis factor-α-238 gene polymorphism also increases the risk of developing CAD in patients with NAFLD in the Chinese Han population. 25 Moreover, variants in patatin-like phospholipase domain-containing protein (PNPLA3) and transmembrane 6 superfamily member 2 (TM6SF2) in patients predisposed to NAFLD conferred a mild protective effect for CAD, and both TM6SF2 and PNPLA3 gene polymorphisms were associated with lower plasma lipid levels.3,26 These results suggested that gene polymorphisms play an important role in the development of CAD in patients with NAFLD.
A previous study showed that the AGT M35T gene polymorphism was strongly associated with an increased risk of heart failure. 27 A study in Saudi Arabia reported that AGT variants (rs5051C and rs7079G) were related to CAD. 28 In the current study, we investigated the effect of the AGT rs2493132 polymorphism on the risk of NAFLD in the general population and the risk of CAD in patients with NAFLD for the first time. We found that the AGT rs2493132 CT+TT genotype but not the AGT rs2493132 T allele was significantly associated with the risk of developing CAD in patients with NAFLD. After adjustments for age, sex, and BMI, the AGT rs2493132 CT+TT genotype remained associated with the risk of CAD. In addition, the AGT rs2493132 T allele significantly increased the risk of developing CAD in patients with NAFLD after adjustments for these parameters.
Dyslipidemia is a common feature of patients with both NAFLD and CAD and is characterized by elevated plasma triacylglycerol and circulating LDL particles and reduced HDL.29–32 Brouwers et al. suggested that plasma lipids act as major mediators of the relationship between NAFLD and CVD. 3 The analysis of patient characteristics in this study revealed that patients with NAFLD exhibit higher BMI, AST, ALT, TG, LDL, and GGT and decreased HDL levels compared with healthy controls, consistent with the results in previous studies.30,33–35 In the overall patient group in this study, we found that AGT rs2493132 T allele carriers were more likely to have higher serum TC and LDL levels compared with non-carriers. A previous study suggested that decreased LDL levels protected patients with NAFLD from CVD, and NAFLD susceptibility genes contributed to the strong relationship between plasma lipids and the risk of CAD.36,37 These data suggested that AGT rs2493132 gene polymorphism may increase the risk of CAD in patients with NAFLD by affecting serum TC and LDL levels.
There were several limitations to this study. First, the diagnosis of NAFLD was determined by ultrasonography rather than liver biopsy due to the limited acceptability of patients to liver biopsies during clinical examinations. Second, CAD usually occurs more often in elderly patients; therefore, the mean age in patients with NAFLD + CAD was higher than in patients with NAFLD and healthy controls. Third, all study subjects in the study were Han Chinese in Qingdao. Therefore, the effects of AGT rs2493132 on the risk of NAFLD and CAD should be studied in other countries and ethnicities.
Conclusion
This study investigated the effect of AGT rs2493132 polymorphism on the risk of NAFLD and CAD in the Chinese Han population. The results showed that the AGT rs2493132 CT+TT genotype was significantly associated with the risk of CAD in patients with NAFLD and NAFLD + CAD in healthy controls. The AGT rs2493132 T allele increased the risk of NAFLD + CAD in healthy controls. After adjustments for age, sex, and BMI, the AGT rs2493132 CT+TT genotype and T allele remained as significant risk factors for CAD in patients with NAFLD. In addition, AGT rs2493132 T allele carriers showed higher LDL and TC levels compared with non-carriers among all subjects. Our study was the first to investigate the effect of AGT rs2493132 polymorphism on the risk of developing NAFLD and CAD. Our results should be verified in other countries and ethnicities in future studies.
Footnotes
Author contributions
Study concept and design: Shiying Xuan and Yongning Xin
Data acquisition: Mengzhen Dong, Shousheng Liu, Mengke Wang, and Yifen Wang
Drafting of the manuscript: Mengzhen Dong, Shousheng Liu, Mengke Wang, and Yifen Wang
Critical revision of the manuscript for important intellectual content: Shiying Xuan and Yongning Xin
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This study was supported by a grant from the National Natural Science Foundation of China (31770837).