
Abstract
Objective
To investigate the utility of 18F-fluorodeoxyglucose (18F-FDG) positron emission tomography/magnetic resonance imaging (PET/MRI) for the preoperative diagnosis of cervical cancer.
Methods
We retrospectively analyzed 114 patients who were diagnosed with cervical cancer and underwent PET/MRI (n = 59) or PET/computed tomography (PET/CT) (n = 65) before surgery. The maximal standardized uptake value (SUVmax) and mean SUV (SUVmean) were determined for regions of interest in the resultant radiographic images.
Results
Relative to PET/CT, 18F-FDG PET/MRI exhibited higher specificity and sensitivity in defining the primary tumor bounds and higher sensitivity for detection of bladder involvement. The SUVmax and SUVmean of PET/MRI were remarkably higher than those of PET/CT as a means of detecting primary tumors, bladder involvement, and the lymph node status. However, no significant differences in these values were detected when comparing the two imaging approaches as a means of detecting vaginal involvement or para-aortic lymph node metastasis.
Conclusions
These outcomes may demonstrate the capability of 18F-FDG PET/MRI to clarify preoperative cervical cancer diagnoses in the context of unclear PET/CT findings. However, studies directly comparing SUVs in different lesion types from patients who have undergone both PET/MRI and PET/CT scans are essential to validate and expand upon these findings.
Keywords
Introduction
Cervical cancer is among the most common malignancies in women, with more than 50 million newly reported cases and 27 million cervical cancer-related deaths occurring worldwide each year. 1 When restricted to the lower pelvis, cervical cancer is generally curable through chemoradiotherapy and/or surgery. 2 Several preoperative prognostic factors, including the clinical stage, diameter, and volume of the tumor, are helpful for prediction of the prognosis in patients with cervical cancer.3–5 However, traditional imaging modalities are limited in their ability to measure such prognostic parameters. In comparison with surgical staging, clinical staging based on the criteria of the International Federation of Gynecology and Obstetrics (FIGO) can insufficiently stage as many as 30% of patients with stage IB and 64% of patients with stage IIIB cervical cancer. 6 The use of more advanced imaging approaches, including magnetic resonance imaging (MRI), computed tomography (CT), and fluorine-18-labeled fluorodeoxyglucose positron emission tomography (18F-FDG PET), can improve clinicians’ ability to accurately diagnose and treat cervical cancer.7,8
Since their advent, PET/CT imaging technologies have continued to advance, leading to major improvements in image quality.9,10 Although combination PET/CT imaging has been highly successful, researchers have explored its replacement with combination PET/MRI11,12 because MRI scans provide higher resolution, reduce patient radiation exposure, and expand functional and molecular imaging options relative to CT. MRI scans cannot readily replace CT components in existing PET/CT scanners; however, technical modifications of MRI and PET instruments are required to obtain fully integrated PET/MRI scans. MRI and PET can also interfere with one another through field gradients or MR radiofrequency.13,14 However, PET/MRI may be a valuable technique for patients with endometrial and cervical cancer. 15 It is also essential that accurate MRI-based approaches be used for PET emission data attenuation correction, specifically for quantitative PET. Whereas CT scans measure tissue attenuation coefficients in response to X-ray exposure, MRI signals are impacted by hydrogen density and relaxation within target tissues,16,17 making 511-keV photon attenuation coefficient derivation more challenging for MRI than for CT. Many researchers to date have highlighted the clinical feasibility of whole-body PET/MRI scans in patients with various types of cancers by comparing these scan results to those derived from PET/CT scanning.18–21 Such whole-body PET/MRI scans can yield high-quality images that are associated with small but significant differences in tracer dosage.
In the present study, we compared the outcomes of whole-body 18F-FDG PET/MRI and PET/CT in an effort to understand the potential of 18F-FDG PET/MRI for the preoperative evaluation of patients with cervical cancer and to summarize the clinical significance of quantitative indicators associated with this imaging approach.
Materials and methods
Patients
This study was approved by the ethics committee of Beijing Anzhen Hospital (approval no.: 2019079X). The ethics board in the hospitals waived the requirement for obtaining informed consent from the patients because this was a retrospective investigation. However, we obtained patient consent for treatment, and all patient details have been de-identified. This study involved 124 patients who received a histological diagnosis of primary cervical cancer and underwent PET/MRI or PET/CT from January 2013 to December 2017 in the Obstetrics and Gynecology Department of Chinese PLA General Hospital. For this study, we selected patients who had cervical cancer that had been positively diagnosed via biopsy, had undergone preoperative PET/MRI or PET/CT evaluation, underwent radical or modified radical hysterectomy, had complete case data, and provided written informed consent.
We excluded patients who were claustrophobic, were unable to satisfactorily control their breathing, declined to undergo PET/MRI or PET/CT imaging, were allergic to the 18F-FDG contrast agent, had coagulation disorders, had other concomitant tumors, had other serious medical conditions, or were unable to tolerate anesthesia or surgery. Fifty-nine patients underwent whole-body 18F-FDG PET/MRI scanning and 65 patients underwent 18F-FDG PET/CT scanning; these latter 65 patients served as the control group in the present analysis. Cancer staging was conducted based on the FIGO cancer staging system. Patients with stage IA, IB1, IIA1, and IIA2 disease were treated via modified radical hysterectomy, while those with stage IB2 and IIB disease were treated via radical hysterectomy. The overall demographic information of the patients in the present study is shown in Table 1.
Patient demographics.

Data are presented as mean ± standard deviation or n (%).
*p > 0.05 was not considered statistically significant.
PET: positron emission tomography, MRI: magnetic resonance imaging, CT: computed tomography, BMI: body mass index, FIGO: International Federation of Gynecology and Obstetrics.
18F-FDG PET/CT
All patients fasted for a minimum of 6 hours before 18F-FDG PET/CT imaging. The scan was then performed with a 64-row multidetector PET/CT system (Biograph™ TruePoint™ 64; Siemens AG, Munich, Germany) equipped for a four-ring PET scanner and a 40-section CT scanner. PET images were collected following intravenous administration of 18F-FDG (555 MBq) for 50 to 70 minutes from the vertex to mid-thigh, and a 1.5-minute scan time per table position was used (matrix size, 512 × 512). This PET scanner had a spatial resolution of 4.4-mm full width at half maximum (FWHM) at 1 cm and 5.2-mm FWHM at 10 cm from the transverse field of view (FOV), with a sensitivity of 9.7 kcps/MBq at the center of the FOV. Prior to PET acquisition, a standard helical low-dose CT scan (120 kV, 80 mA, 0.8 s/rotation, pitch 1.5, 3.75-mm slice thickness) was acquired from the head to the proximal thigh using the CARE kV and CARE Dose 4D dose reduction software provided by the manufacturer. Intravenous iodinated contrast was not administered to any patients. Following scanning, PET image reconstruction and CT attenuation correction were completed through the use of an ordered-subset expectation maximization iterative reconstruction algorithm (2 iterations and 21 subsets).
18F-FDG PET/MRI
18F-FDG PET/MRI scans were conducted in 59 patients using a Magnetom Biograph mMR instrument (Siemens Healthineers, Erlangen, Germany) equipped with a strength of the 3T magnetic field, whole-body imaging matrix coil technology with radiofrequency surface coils having multiple integrations, and a PET system of fully functional condition with embedded avalanche photodiode technology in the MR gantry. Three hybrid PET/MRI platforms have been marketed to date: simultaneous PET/MRI, sequential PET/MRI, and sequential PET/CT-MRI 22 ; the instrument used in this study was a simultaneous PET/MRI instrument. All patients fasted for 6 hours prior to scanning, after which they were intravenously administered a body weight-appropriate dose of 18F-FDG (4 MBq/kg; mean, 285 ± 70 MBq; range, 154–456 MBq). Following a 2-hour period of 18F-FDG administration, PET/MRI was initiated.
The PET scanner had a 4.4-mm FWHM spatial resolution at 1 cm, with a resolution of 5.3-mm FWHM at 10 cm from the transverse FOV. We conducted the whole-body PET scanning in four bed positions from the vertex to the mid-thigh, with an acquisition time of 5 minutes per position. Simultaneous whole-body MRI scanning was also conducted in the same positions with a sagittal short tau inversion recovery (STIR) sequence and a breath-holding half-Fourier single-shot turbo spin echo (HASTE) sequence. Regional PET was conducted with a 10-minute acquisition time. Pelvic MRI was conducted using previously reported sequences 23 as follows (Table 2): a transverse T2 turbo spin echo (TSE) sequence, a sagittal T2 TSE sequence, a transverse T1 TSE sequence, a transverse fat-saturated T1 TSE following intravenous contrast administration (0.1 mmol/kg gadobutrol (Gadavist; Bayer Healthcare, Germany)), a sagittal post-contrast T1 TSE, and a transverse diffusion-weighted echo-planar imaging sequence using two b-values: b0 and b1000 s/mm2. Following scan completion, an ordinary Poisson ordered-subset expectation maximization approach (3 iterations, 21 subsets, a 4-mm Gaussian post-processing filter, and matrix size of 512 × 512) was used for image reconstruction.
Comparison of diagnostic indicators between imaging detection technology and surgical pathology.

*p < 0.05 was considered statistically significant.
PET: positron emission tomography, MRI: magnetic resonance imaging, CT: computed tomography, Sens: diagnostic sensitivity, Spec: diagnostic specificity.
Image analyses and reference standards
Fellowship-trained nuclear medicine physicians and radiologists respectively analyzed the PET/MRI and PET/CT images with a dedicated program (syngo.via; Siemens Healthineers). Focal lesions in PET images exhibiting enhanced glucose uptake in comparison to surrounding tissue were deemed suspicious. To effectively identify every region of possible microscopic disease, all submucosal abnormalities in MRI were presumed to be associated with tumor infiltration consistent with current clinical standards aimed at encompassing all abnormal parts within the imaged field. 24 Regional lymph nodes were deemed metastatic when extracapsular spread or necrosis was detected or when a cluster of borderline size 3+ lymph nodes was detected. The diagnosis of distant metastases was based upon morphological lesion and contrast enhancement patterns.
When assessing the scan results, the reviewers were requested to evaluate both technical feasibility and diagnostic performance parameters, rating the overall PET image quality for PET/CT and PET/MRI scans as follows: 1 = nondiagnostic, 2 = poor, 3 = good, and 4 = excellent.
The maximal standardized uptake value (SUVmax) and mean SUV (SUVmean) for primary tumors, metastases, and metastatic lymph nodes were used as a means for quantitative analysis of the diagnostic efficacy of the PET/MRI scans. For these analyses, a volume of interest surrounding these lesions was drawn with the isocontour function of the volume of interest in the analytical software with a SUVmax threshold of 40%.
We analyzed the identified primary cervical cancers via the cognitive fusion of diffusion-weighted images and T2-weighted images. The scanning software generated apparent diffusion coefficient (ADC) maps in an automated manner. Tumor diffusion parameters were calculated by manually marking tumor tissue borders using a polygonal region of interest in each ADC map slice.
Statistical analysis
The relative sensitivity and specificity for each imaging modality were calculated. Data analyses and figure construction were conducted using OriginPro 2016 (OriginLab Corporation, Northampton, MA, USA) and SPSS for Windows, Version 16.0 (SPSS Inc., Chicago, IL, USA). Quantitative data are given as mean ± standard deviation and were compared via one-way analysis of variance and Student’s t-test. Confidence thresholds for these analyses were set at 95% and 99%.
Results
Patient characteristics
This study involved 124 patients with untreated histologically confirmed primary cervical cancer from January 2013 to December 2017. Of these patients, whole-body 18F-FDG PET/MRI scanning was performed for 59 patients, while 65 underwent 18F-FDG PET/CT scanning. As shown in Table 1, no significant differences in the patients’ age, body mass index, surgical strategy, FIGO cancer stage, or history of abdominal surgery were found between the PET/CT and PET/MRI groups, enabling comparative analyses between these two patient groups.
Comparison of diagnostic indicators between imaging detection technology and surgical pathological findings using histopathology as gold diagnostic standard
Excellent-quality images (score of 4) were obtained for all scans (PET/CT and PET/MRI) recorded in this study, with representative images shown in Figures 1 and 2, respectively. No detectable errors were observed in any MR attenuation correction map reads, and perfect spatial coregistration (<2-mm mismatch) was observed between PET and MRI or CT in all patients. Relative to PET/CT, higher sensitivity and specificity were observed for 18F-FDG PET/MRI when defining the primary tumor extent (Figures 1d and 2d, red arrow). After undergoing PET/CT or PET/MRI, all patients underwent modified radical or radical hysterectomy as appropriate, and all tumor tissues were then subjected to immediate pathological analysis (data not shown). Comparisons of the diagnostic indicators associated with these two imaging approaches and surgical pathology are shown in Table 2. When assessing primary tumors, 18F-FDG PET/MRI showed significantly higher sensitivity than PET/CT (94.4% vs. 61.9% for <2-cm primary lesions, p = 0.016; 89.7% vs. 68.6% for 2- to 4-cm primary lesions, p = 0.042; and 100% vs. 66.7% for >4-cm primary lesions, p = 0.031).

Imaging findings in a 26-year-old patient with FIGO IB1 cervical cancer. (a) Whole-body 18F-FDG uptake. (b) Tumor and uterine cervix 18F-FDG uptake map. (c) Tumor CT map. (d) Fused 18F-FDG PET/CT image of tumor lesion map.
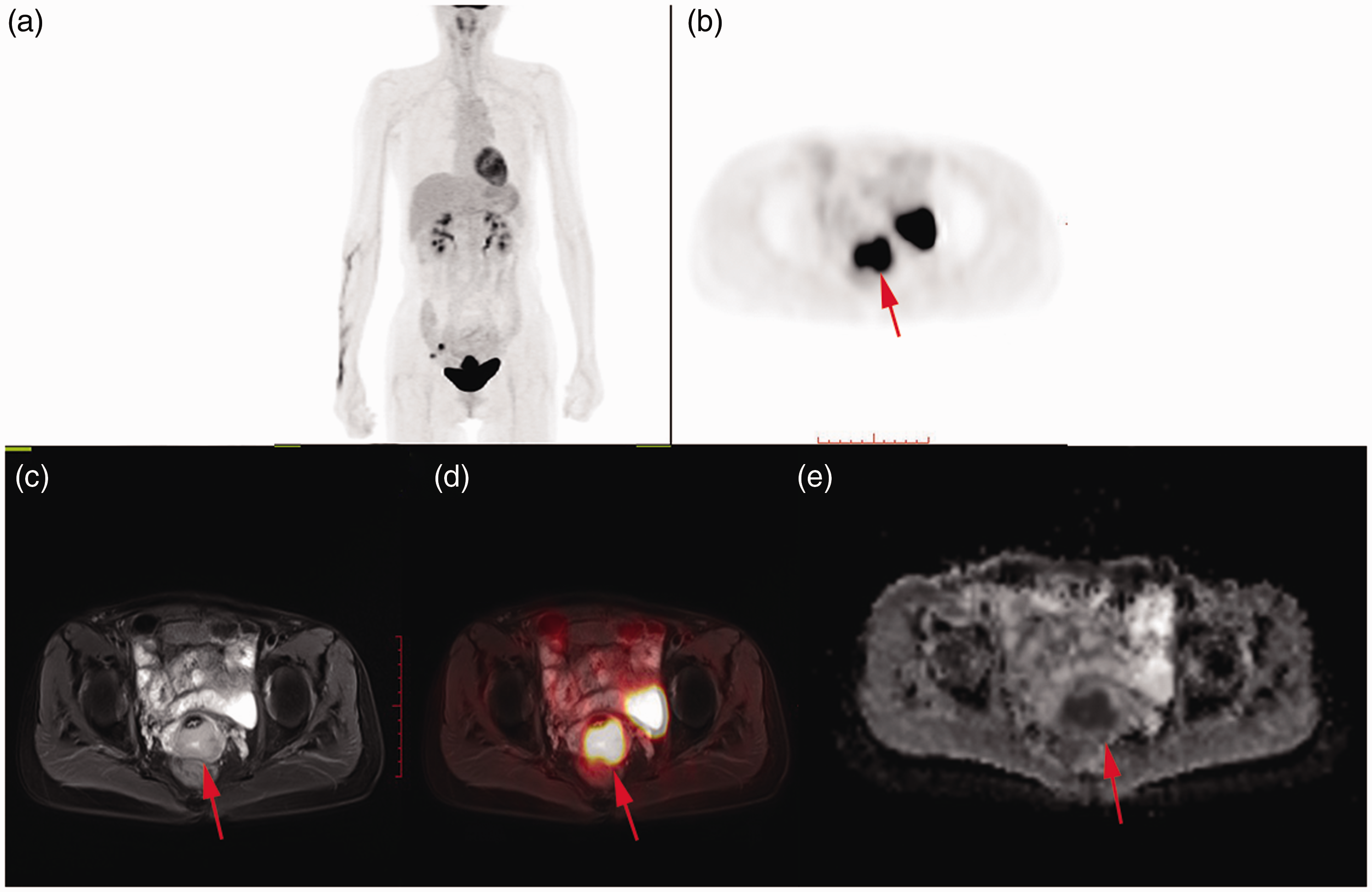
Imaging findings in a 56-year-old patient with FIGO IB1 cervical cancer. (a) Whole-body 18F-FDG uptake. (b) Uterine cervix 18F-FDG uptake. (c) T2-weighted MRI. (d) Fused 18F-FDG PET/T2-weighted MRI of the lesion. (e) Tumor ADC map.
As a means of assessing vaginal involvement, however, the differences in diagnostic sensitivity and specificity were not statistically significant between PET/MRI and PET/CT. In contrast, these two approaches exhibited significant differences in diagnostic sensitivity when used to assess bladder involvement (p = 0.023). Similarly, for detecting pelvic lymph node metastasis via 18F-FDG PET/MRI and 18F-FDG PET/CT on a per-level basis, the specificity and sensitivity were 96.2% vs. 93.1% and 87.9% vs. 91.7%, respectively, with no significant differences. However, PET/MRI showed significantly higher sensitivity than PET/CT when used to detect para-aortic lymph node metastases (100% vs. 33.3%, p = 0.035).
Quantitative lesion analysis
During the analysis of only primary tumors, both the SUVmean and SUVmax were significantly higher in the PET/MRI group than in the PET/CT group (p < 0.001) (Table 3). The SUVmax and SUVmean differed by 57% and 54%, respectively, between PET/MRI and PET/CT. When specifically assessing vaginal involvement, however, no significant difference was observed in the SUVmax or SUVmean of these two groups (Table 3). In contrast, when evaluating bladder involvement, the SUVmax and SUVmean were significantly higher in the PET/MRI group than in the PET/CT group (p < 0.001) (Table 3). Finally, when analyzing para-aortic lymph node metastases, the SUVmax and SUVmean were also significantly higher in the PET/MRI group than in the PET/CT group (p < 0.001). No significant differences were found for pelvic lymph node metastases (Table 3).
Quantitative evaluation of lesions.

Data are presented as mean ± standard deviation (n).
* p < 0.05 was considered statistically significant.
PET: positron emission tomography, MRI: magnetic resonance imaging, CT: computed tomography, SUVmax: maximal standardized uptake value, SUVmean: mean standardized uptake value.
Discussion
PET/CT and PET/MRI are multimodal imaging strategies that have seen increasing clinical use in recent years. 25 PET scanning allows researchers and radiographers to gain tissue metabolism-based insights by analyzing tissues labeled with the 18F-FDG positron emission nuclide. 26 In contrast, MRI and CT scans offer detailed anatomical information pertaining to human bone and soft tissue structures.27,28 By integrating PET scans with CT or MRI data, clinicians can obtain whole-body images of the 18F-FDG metabolism profiles of patients with cancer. Rapid tumor cell proliferation and associated increases in glucose uptake and utilization allow for early-stage malignancies to be detected in an extremely sensitive manner via this approach. Because of the high sensitivity to intratumoral metabolic changes using this approach, it is possible to identify the tumor size, scope, degree of malignancy, and TNM staging. 29
Several studies to date have analyzed the PET/CT applications for evaluating gynecological tumors. Bollineni et al. 30 performed a meta-analysis on this topic and found that PET/CT was able to achieve specificity and sensitivity of 90.4% and 82.8%, respectively, for lymph node metastasis in patients with cervical cancer and other gynecological malignancies. While PET/MRI-related evidence-based medicines are still in their infancy, this combined imaging modality offers various advantages over more traditional imaging conducted by PET/CT. First, MRI offers better soft tissue imaging quality than does CT, making it better suited to the evaluation of specific tissues and organs through functional imaging approaches that are incompatible with CT. 31 In the present analysis, the diagnostic sensitivity was significantly higher in the PET/MRI group than in the PET/CT group for primary lesions of <2 cm (94.4% vs. 61.9%), 2 to 4 cm (89.7% vs. 68.6%), and >4 cm (100.0% vs. 66.7%) (p < 0.05). This suggests that PET/MRI scans are better suited to evaluating the lesion scope, providing radiographers and clinicians with additional insight into the tumor stage and status that can guide surgical and treatment planning.
Second, PET/MRI combination imaging can overcome the limitations of sequential PET/CT imaging by enabling complete synchronization of PET and MRI image acquisition, thus permitting simultaneous anatomical and functional metabolic analyses. In this study, a significantly higher diagnostic sensitivity was observed for PET/MRI than for PET/CT when evaluating para-aortic lymph node metastasis (100.0% vs. 33.3%, p < 0.05). This finding is clinically significant in the context of lymphadenectomy and pelvic external beam radiotherapy implementation in patients with cervical cancer patients. Kim et al. 32 observed that 18F-FDG PET/MRI scans offered 100% sensitivity and 96% specificity when used to detect early cervical cancer lymph node metastases of >5 mm in diameter, which was superior to PET/CT and in line with our findings. Third, PET/MRI scans can markedly reduce patient radiation exposure to roughly 20% of that associated with PET/CT scans. 33
Efforts to quantify PET/MRI- and PET/CT-based tumor diagnostic modalities to date have been largely focused on indicators including the SUV, ADC, and metabolic tumor volume. 34 The previously reported tumor SUVmax varies substantially, ranging from an SUVmax cut-off of 9.0 for non-small cell lung cancer to a cut-off of 13.7 for neuroendocrine tumors. The SUVmax cut-off value of cervical cancer, however, remains uncertain, with studies showing this value to be closely related to tumor size, differentiation, and morphology. 35
In the present study, the SUVmax and SUVmean of primary cervical cancer lesions detected via PET/MRI were 23.7 ± 8.1 and 14.2 ± 4.6, respectively, and were significantly higher than those obtained through PET/CT imaging (p < 0.001). Interestingly, the difference in the SUVmax and SUVmean for adjacent organ involvement and/or metastatic lymph nodes was not significantly different between PET/MRI and PET/CT in these patients. From our clinical practice experience, the SUV is considered a half-quantitative index, so its accurate calculation is helpful to determine the range of lesions and metastases.
This retrospective study has three main limitations. The first limitation is the difference in the FDG uptake periods between PET/CT and PET/MRI, which may have affected the PET diagnostic performance and SUVs. The second limitation is that the diagnostic performance for lymph node size was not analyzed. Third, from a technical viewpoint, PET/MRI is still unable to achieve fast scanning of multiple MRI sequences and PET fusion. Therefore, we should constantly optimize MRI sequences for patients with cervical cancer and improve the level of diagnosis.
In summary, PET/MRI is a more efficacious approach to the diagnosis of cervical cancer relative to other available imaging modalities. Primary lesions that are 4 cm in diameter are the diagnostic basis for locally advanced cervical cancer, 36 in addition to serving as the reference basis for cavity radiation therapy. Primary lesions ranging from 2 to 4 cm in size are optimal candidates for preoperative neoadjuvant chemotherapy. Although oncologists can generally evaluate these tumors through specialized examinations, PET/MRI scans represent a more reliable approach to evaluating these tumors. A meta-analysis conducted by Nie et al. 37 showed that PET/MRI is an extremely sensitive and specific approach to the diagnosis of gynecological pelvic tumors.
It is important to use some degree of caution when interpreting these imaging results, however, because neither PET/MRI nor PET/CT perform as reliably in diagnostic contexts as the gold standard approach of direct pathological examination. The SUVs used in these imaging approaches are not objective and are dependent upon the subjective interpretations of those reviewing the resultant scan data. 38 Despite the overall promise of this technology, there are still many limitations to the PET/MRI modality, necessitating future research and development to improve overall diagnostic reliability. Most importantly, further work is required to optimally integrate PET and MRI technologies, reduce overall operative costs, and improve interrater reliability.