
Abstract
Objective
To evaluate the effects of body mass index (BMI) in patients with polycystic ovary syndrome (PCOS) undergoing controlled ovarian stimulation (COS) with intrauterine insemination (IUI).
Methods
This retrospective study evaluated couples with PCOS undergoing COS and IUI. The relationship between cumulative IUI pregnancy outcomes and BMI, treatment cycles, treatment schemes, number of dominant follicles, endometrial thickness, infertility duration and type of infertility was analysed.
Results
The study evaluated 831 IUI cycles in 451 couples with PCOS. Compared with normoweight women, overweight and obese women required more human menopausal gonadotropin (hMG) doses and more days of COS. Gestational diabetes mellitus occurred more frequently in the obese group than in the other BMI groups. The clinical pregnancy and live birth rates in the hMG, clomiphene citrate (CC) + hMG and letrozole (LE) + hMG groups were significantly higher than those in the CC and LE groups. The clinical pregnancy rate was higher in the secondary infertility group compared with the primary infertility group.
Conclusion
Obese women might require more hMG doses and more days of COS to overcome the effects of weight. As BMI increases, the incidence of gestational diabetes might also increase. The number of cycles and type of infertility may have a predictive value for pregnancy outcomes.
Introduction
Polycystic ovary syndrome (PCOS) is the most prevalent endocrine disorder diagnosed in women of childbearing age, with a prevalence of 5.6% in Chinese women aged 19–45 years. 1 The clinical features of PCOS include oligo-ovulation or anovulation, hyperandrogenism and polycystic ovarian morphology. 2 , 3 According to the 2003 Rotterdam consensus, patients with at least two of the three criteria listed above may be diagnosed with PCOS. 3 PCOS is closely related to reproductive and metabolic diseases, which are characterized by anovulatory infertility, abnormal weight, increased risk of cardiovascular disease, severe health concerns and increased economic burden.4 –6
Lifestyle improvements and interventions have become a common consensus for the treatment of PCOS and have been listed as the first-line treatments for PCOS worldwide. 7 A loss of 5–10% of the body weight in overweight and obese PCOS patients is beneficial to the improvement of their reproductive and metabolic indices. 8 For patients that have not recovered ovulation after the 5–10% weight loss, further interventions can be provided. 9 Assisted reproductive technology (ART) has become a common and effective treatment for PCOS. 8 Considering the simple, non-invasive nature and low cost of intrauterine insemination (IUI) compared with those of in vitro fertilization (IVF), if patients do not become pregnant after 3–6 cycles of controlled ovarian stimulation (COS) combined with intercourse, they may try IUI when COS induces follicle maturation. 10
Clinical research has found that PCOS is closely associated with obesity. 11 Obesity, in turn, is strongly associated with the incidence of gestational diabetes, gestational hypertension, macrosomia and a low response to ovulation induction. 12 , 13 The interaction of PCOS and obesity can be detrimental to pregnancy. Therefore, given the association between obesity and PCOS, it is vital to pay more attention to the body mass index (BMI). Despite extensive research, the influence of obesity on the success of IUI remains controversial. Several studies have found that obesity does not negatively impact cycle fecundity during superovulation with IUI treatment. 14 , 15 Some studies have shown that overweight and obese patients have a higher fecundity than normoweight women when undergoing controlled ovarian hyperstimulation with IUI, 16 while other studies have reported negative effects of female obesity on the success of IUI treatment. 17 , 18 The selection of the sample population for the these previous studies were primarily based on BMI, rather than being limited to women with PCOS. Therefore, the present study addressed the impact of BMI as well as other factors in patients with PCOS undergoing COS with IUI on the improvement of pregnancy outcomes.
Patients and methods
Study population
This retrospective study enrolled consecutive couples with anovulatory infertility that underwent IUI between January 2008 and March 2019 at the Clinical Centre of Reproductive Medicine, Lianyungang Maternal and Child Health Hospital, Lianyungang, Jiangsu Province, China. The inclusion criteria were as follows: (i) patients with normal hysterosalpingogram or semen analysis results; (ii) the diagnostic test for PCOS was consistent with the 2003 Rotterdam consensus; (iii) patients with PCOS that did not become pregnant after 3–6 cycles of COS combined with intercourse. Exclusion criteria were as follows: (i) tubal patency and semen analysis were not normal; (ii) pelvic inflammation; (iii) endometriosis. BMI was calculated using the following formula: BMI = weight/height 2 (kg/m2).
This study was approved by the Lianyungang Maternal and Child Health Hospital Research Ethics Board, Lianyungang, Jiangsu Province, China in 2020. The reporting of this study conforms to the ‘The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for Reporting Observational Studies’. 19 All patient details in this study have been de-identified to maintain anonymity. As this was a retrospective study, patients were not asked to actively participate.
Ovarian stimulation and IUI protocol
Ovarian stimulation was started between day 3 and day 5 of the menstrual cycle. The stimulation agents included clomiphene citrate (CC; Codal-Synto Ltd., Limassol, Cyprus), letrozole (LE; Jiangsu Hengrui Pharmaceutical Company, Lianyungang, China), human menopausal gonadotropin (hMG; Livzon Pharmaceutical, Zhuhai, China) or hMG with CC or LE. Dosages were based on BMI, antral follicle count and the patients’ previous response, if applicable. Transvaginal ultrasound was used to monitor the follicles and endometrium. The following ovulation trigger was implemented when the dominant follicle diameter was ≥18 mm: 10000 IU human chorionic gonadotropin (hCG; Livzon Pharmaceutical Co, Guangzhou province, China) intramuscular injection or 0.1 mg triptorelinacetate (GnRH-a; Ferring, St-Prex, Switzerland) subcutaneous injection. The IUI was executed 28–36 h after the ovulation trigger. The husband was directed to collect the semen specimen on the condition that abstinence was observed 2–7 days prior to collection. The total number of motile sperm was >10 × 106 after processing. The operator slowly injected the treated sperm suspension into the uterine cavity via a soft catheter. The patient was required to lie down for 20–30 min after the IUI. Conventional luteal phase support was performed, in the form of 200 mg soft progesterone capsules (Besins Healthcare, Brussels, Belgium) orally once daily for 14 days.
Outcome assessment and a follow-up visit
Transvaginal ultrasound was performed to evaluate for clinical pregnancy 1 month after the IUI. The patients received relevant professional follow-up from pregnancy to childbirth.
Statistical analyses
All statistical analyses were performed using IBM SPSS Statistics for Windows, Version 25.0 (IBM Corp., Armonk, NY, USA). All data were transferred to Microsoft Excel (Microsoft Corp., Redmond, Washington, United States) for analysis. All figures were drawn using GraphPad Prism 8 (Graphpad Software Inc., San Diego, CA, USA). Data were compared between groups using χ2-test. Fisher's exact probability method was applied to when the sample size was <40. A P-value <0.05 was considered statistically significant.
Results
This retrospective study enrolled 451 couples with PCOS that underwent IUI (n = 831 IUI cycles). The median age of the study participants was 28 years (range, 21–37 years); and 58 of 831 (7.0%) of the participants were ≥35 years of age. As so few of the study participants were ≥35 years, age was not used as a predictor of pregnancy outcomes in this study. The clinical pregnancy rate (CPR) was 188 of 831 (22.6%) per cycle and 188 of 451 (41.7%) per couple; 20 of 188 (10.6%) pregnancies resulted in miscarriage, while two of 188 (1.1%) were ectopic. Of the successful pregnancies, 184 of 186 (98.9%) were singletons and two of 186 (1.1%) were twins.
The female patients were divided into four groups based on body weight. Low body weight patients had a BMI of ≤18.4 kg/m2 (17 of 831, 2.0%); normoweight patients had a BMI of 18.5–23.9 kg/m2 (299 of 831; 36.0%), overweight patients had a BMI of 24.0–27.9 kg/m2 (321 of 831; 38.6%) and obese patients had a BMI ≥28 kg/m2 (194 of 831; 23.3%). Compared with the normoweight group, the obese and overweight groups required significantly higher dosages of hMG (P < 0.05 for both comparisons; Figure 1A) and more days of COS (P < 0.05 for both comparisons; Figure 1B).

The dosages of human menopausal gonadotropin (hMG) and the duration of controlled ovarian stimulation (COS) required in couples with polycystic ovary syndrome (PCOS) that underwent intrauterine insemination (IUI) stratified according to the body mass index (BMI) of the female patient. Analysis of the relationship between BMI and dosages of hMG (a) and days of COS (b). Data presented as mean ± SD. **P < 0.01 ; ***P < 0.001; χ2-test. The colour version of this figure is available at: http://imr.sagepub.com.
There were no significant differences in the rates of clinical pregnancies, miscarriage, ectopic pregnancies, live births, multiple pregnancies or the delivery method in the different BMI groups (Table 1). The miscarriage rate in the normoweight patients with PCOS was lower than those in the overweight and obese patients with PCOS, but the differences were not significant. The rate of gestational diabetes mellitus was significantly higher in the obese group than in the other three groups (P < 0.05). There was no significant difference in gestational hypertension and macrosomia between the four BMI groups.
The effect of body mass index (BMI) on pregnancy outcome and complications in couples with polycystic ovary syndrome (PCOS) that underwent intrauterine insemination (IUI).

Data presented as n of patients (%).
aχ2-test; *P < 0.05 versus obese group; NS, no significant between-group difference (P ≥ 0.05).
The patients were classified into four groups based on their IUI cycle. There were 451 patients in their first cycle, 237 in their second cycles, 108 in their third cycles and 35 had ≥four cycles. The CPR did not differ significantly based on the number of cycles completed. The association between the cumulative number of cycles and the cumulative pregnancy outcomes were examined further. The results showed that the cumulative CPR and live birth rate (LBR) increased as the number of cycles increased (Figure 2A), with the increase in CPR plateauing after the third cycle. In pregnant women, the CPR was 111 of 188 (59.0%) after the first cycle, while it was 45 of 188 (23.9%), 19 of 188 (10.1%) and 11 of 188 (5.9%) after the second, third and fourth cycles, respectively (Figure 2B).
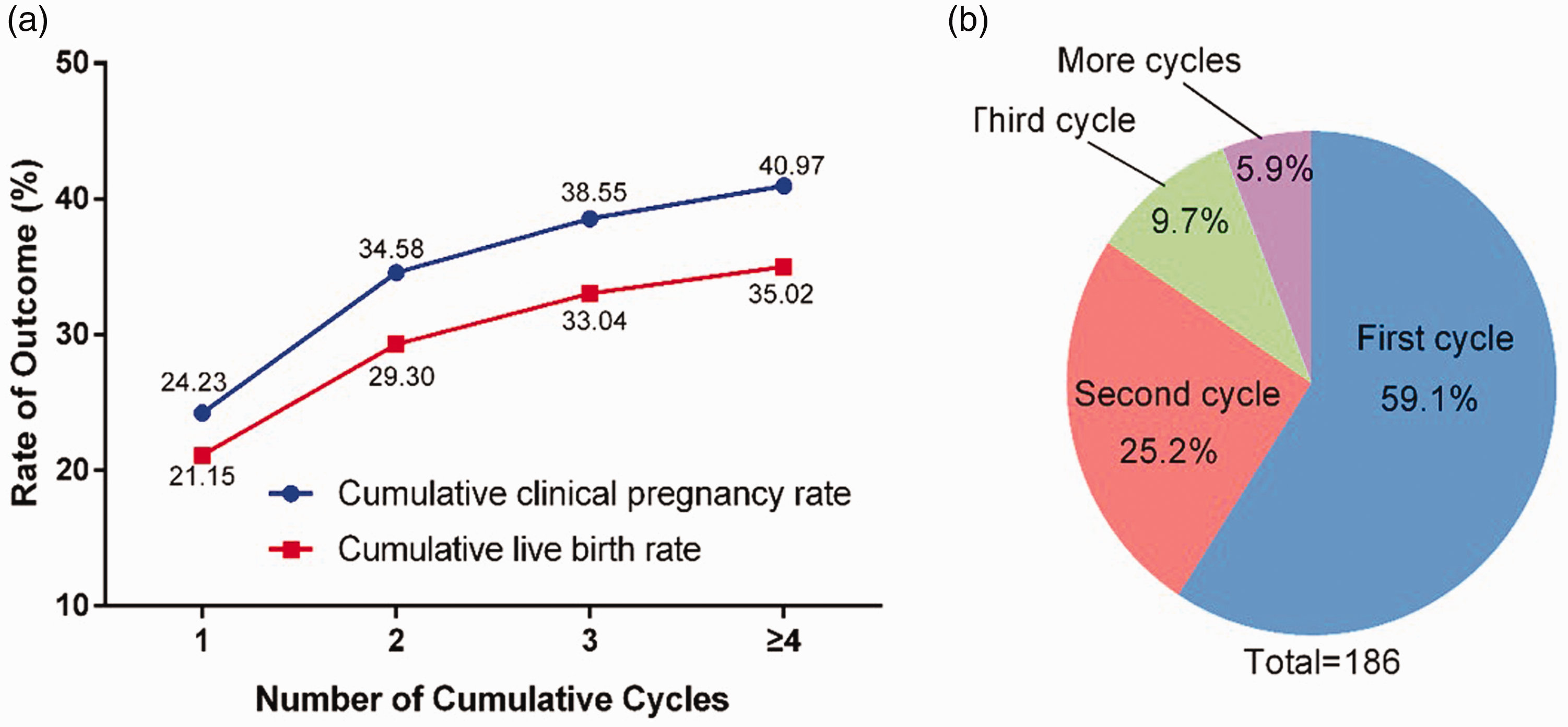
The relationship between the number of intrauterine insemination (IUI) cycles and pregnancy outcomes. The relationship between the number of IUI cycles and cumulative clinical pregnancy rate and cumulative live birth rate (a) and the pregnancy rate in various cycles in the pregnant group (n = 186) (b). Data presented as percentage of patients. The colour version of this figure is available at: http://imr.sagepub.com.
The patients were divided into five groups based on the stimulation agent used during COS: CC, LE, hMG and hMG combined with CC or LE. The CPR and LBR in the hMG, CC + hMG and LE + hMG groups were significantly higher than those in the CC and LE groups (P < 0.05 for all comparisons) (Table 2). No significant difference was observed between the CC and LE groups. There was no significant difference in the rates of miscarriage, multiple pregnancies or caesarean sections.
The relationship between controlled ovarian stimulation (COS) treatment protocols and intrauterine insemination (IUI) pregnancy outcomes in couples with polycystic ovary syndrome (PCOS).

Data presented as n of patients (%).
aχ2-test; *P < 0.05 versus CC and LE groups; **P < 0.01 versus CC and LE groups.
CC, clomiphene citrate; LE, letrozole; hMG, human menopausal gonadotropin; NS, no significant between-group difference (P ≥ 0.05).
The patients were divided into two groups: pregnant and non-pregnant (Table 3). A total of 556 patients had primary infertility and 275 had secondary infertility. The CPR of the primary infertility group was 20.5% (114 of 556) and it was 26.9% (74 of 275) for the secondary infertility group (P < 0.05). There were no significant differences between the pregnant and non-pregnant groups in terms of duration of infertility, endometrial thickness on the hCG day, the number of dominant follicles and the type of endometrial tissue.
Comparison of the infertility characteristics between the pregnant and non-pregnant groups of women with polycystic ovary syndrome that were treated with controlled ovarian stimulation and intrauterine insemination.

Data presented as mean ± SD or n of patients.
aχ2-test; NS, no significant between-group difference (P ≥ 0.05).
Discussion
Polycystic ovary syndrome is closely associated with obesity and the two diseases have overlapping characteristics. 20 Previous research demonstrated that the dosage of COS agents used differed significantly among BMI categories; PCOS patients with a BMI ≤25 kg/m2 required fewer gonadotrophins to achieve the same number of oocytes retrieved when undergoing controlled ovarian hyperstimulation. 21 , 22 In the present study, the hMG dosages and the days of COS were higher in the overweight and obese groups than in the normal group, indicating that obesity may impair ovarian responsiveness to gonadotrophin induction. Therefore, it is economical and expedient for overweight PCOS patients to lose weight.
Body mass index is a significant factor that affects pregnancy outcomes. 21 However, some studies showed that there was no difference in the rates of successful pregnancies and miscarriages between the normoweight and obese groups undergoing IVF. 22 , 23 The present study showed no difference in CPR, LBR or miscarriage rate between the different BMI groups, suggesting that BMI had little effect on IUI outcomes. In the literature, ovarian responsiveness to gonadotrophin induction is impaired by obesity, increasing the number of cycles cancelled, premature births and miscarriages, while these hazards were overcome with an increase in dosage. 20 The rate of caesarean sections increased with BMI in the current study, although the difference was not significant, which was in accordance with the conclusion that overweight and obesity were associated with an increased risk of caesarean delivery. 24 A reduction in pregravid BMI for overweight and obese women was associated with a significant reduction in caesarean deliveries. 25
Obesity adversely affects the maternal milieu by increasing the risk of gestational diabetes and hypertensive disease in pregnancy. 5 A previous study reported that abnormal weight did not affect pregnancy outcomes in women with PCOS that underwent frozen embryo transfer. 26 The results of the present study showed that the incidence of gestational diabetes was higher in the obese group. There were no statistically significant differences in macrosomia and hypertension disease between the BMI groups in the present study. There are many possible reasons for these differences: limitations of sample size, gaps in research methods and study participant characteristics. In the long term, the offspring of women that were overweight and obese before pregnancy have a significantly increased risk of developing obesity and/or metabolic syndromes later in life. 27 In addition, the risk of cardiovascular disease, coronary heart disease and type 2 diabetes increases in their adult offspring. 28 Being overweight before pregnancy may also cause behavioural, cognitive and emotional disorders in the women’s offspring. 29 Therefore, controlling maternal weight is beneficial for the health of their offspring.
Previous research has demonstrated that the CPR increased with the number of IUI trials. 30 The current results demonstrated that the probability of getting pregnant per cycle increased with an increase in the number cycles, whereas the CPR increase plateaued after the third cycle. Therefore, if a couple fails to get pregnant after 3–6 cycles of ovulation induction combined with artificial insemination, it is likely that other factors are causing their infertility. For these couples, IVF treatment is recommended. This current study demonstrated that the group treated with hMG obtained higher CPRs and LBRs than those using CC or LE alone. A meta-analysis proved that gonadotrophins seem to improve LBR compared with CC. 31 hMG had been found to be beneficial for oocyte maturation, which may improve embryo implantation in the endometrium. 32 , 33
This current study demonstrated that CPR in the secondary infertility group was higher than that in the primary infertility group. Some women previously had regular menstruation and ovulation. Women that had a history of pregnancy will experience irregular menstruation, ovulation disorders and polycystic ovarian after gaining weight, which leads to secondary infertility. These patients had no mature oocytes, hence the failed fertilization. Compared with patients with primary infertility, those with secondary infertility have a higher chance of having a successful pregnancy after correcting the ovulation problems.
The CPR decreased as the duration of infertility increased. 34 However, the current results showed no significant difference in the duration of infertility between the pregnancy and non-pregnancy groups, which was inconsistent with previous research. 34 In our experience, some patients diagnosed with PCOS have a longer period of infertility due to oligo-ovulation or anovulation, leading to missed chances of pregnancy. The duration of infertility had little significance on overall pregnancy outcomes in the current study. The current study also analysed the relationship between the number of follicles and pregnancy outcome, but found no significant differences in the dominant follicles in the pregnant and non-pregnant groups. A previous study reported that multi-follicle growth was associated with higher CPR than mono-follicle growth. 35 However, another study found no correlation between increased number of follicles and pregnancy outcomes. 36
Endometrial receptivity refers to the capacity of the endometrium to accept embryos. Ultrasound characteristics can be indicators to evaluate endometrial receptivity, including endometrial thickness, classification, peristaltic wave and blood flow. 37 Endometrial thickness did not differ between the pregnancy and non-pregnancy groups in the current study. Considering that endometrial thickness had no obvious predictive value for the pregnancy outcome of ART, it is not suggested to cancel IUI or embryo transfer only according to endometrial thickness. 31 Previous research demonstrated that women with an ultrasound scan displaying a triple-line pattern had more positive outcomes. 39 These studies did not achieve consistent conclusions.38,39It is unreasonable to evaluate intimal receptivity through thickness or classification separately because ultrasound indicators must be comprehensively assessed.
This current study had several limitations. First, the small sample size. Secondly, the retrospective study design. Therefore, the results obtained from this current study should be interpreted with caution considering these limitations.
In conclusion, obese women might need to be treated with higher doses of stimulating agents for more days during their COS treatment in order to overcome the effects of increased weight. Once the effect is overcome by adding hMG, CPR may be similar to that in normoweight women. As BMI increases, the incidence of gestational diabetes might also increase. The number of treatment cycles and the infertility types have predictive values for pregnancy outcomes. The other variables were not significantly different. Further studies are required to obtain meaningful results.
Footnotes
Author contributions
Li-Sha Tang and Huai-Yun Tang designed the research; Hui-Juan Guan, Lin-Qing Pan and Hang Song collected the data and wrote the paper; Hui-Juan Guan, Lin-Qing Pan and Hang Song analysed the data; Hui-Juan Guan and Lin-Qing Pan edited the manuscript. All authors have read and approved the final manuscript.
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants from the Jiangsu Basic Research Program (Natural Science Foundation, no. BK20161298), the Jiangsu Commission of Health (no. H2018014) and 521 Projects of Lianyungang (no. LYG52105-2018080).