
Abstract
Well-differentiated papillary mesothelioma (WDPM) is an uncommon mesothelial tumor. The lesions may be single or multiple and usually behave in a benign or indolent fashion, sometimes persisting for many years. In the present case, a 37-year-old woman had experienced primary infertility for 12 years, and a diagnostic laparoscopy was performed. Approximately 200 mL of dark red, free fluid in the pelvis and more than 10 yellow-white nodules on the surface of the right round ligament, sacrum ligament, right fallopian tube, and both sides of the uterus were found. A lesionectomy was performed and immunohistochemical markers indicated WDPM with adenomatoid tumor. The patient was monitored by computed tomography and serum CA125 (cancer antigen 125) levels for 49 months with no recurrence. WDPM and adenomatoid tumor are both benign tumors of mesothelial origin. Because of the lack of effective radical treatment, regular follow-up is sufficient. However, the effects of estrogen and progesterone on WDPM and adenomatoid tumors during ovulation or pregnancy remains unclear. Although WDPM is not life threatening, a strategy to fulfill the fertility requirements of women with this condition is a new challenge for infertility doctors.
Keywords
Background
Well-differentiated papillary mesothelioma (WDPM) is an abnormal mesothelial proliferation most commonly encountered as an incidental finding in the peritoneal cavity, pericardium, or tunica vaginalis. WDPM occurs within a wide age range, is especially found during the reproductive years, and affects more women than men. 1 The lesions may be single or multiple but, by definition, do not invade the underlying stroma and usually behave in a benign or indolent fashion, sometimes persisting for many years.2,3 Patients with WDPM are mostly asymptomatic; thus, WDPM is rarely seen in patients with infertility.
Case Report
Four years prior to this reporting, a 37-year-old woman (gravida 0) consulted our Department of Gynecology for primary infertility that she had experienced for 12 years. Physical examination was normal, ovulation occurred in the natural cycle, hysterosalpingography revealed unilateral patency, and transvaginal ultrasound revealed chylous echo pelvic effusion, measuring 47 mm anterior and 46 mm posterior to the uterus. Her serum CA125 level was 43.53 U/mL (normal range: 0–35 U/mL). Before proceeding with assisted reproductive technology, we performed a diagnostic laparoscopy.
In the pelvis, approximately 200 mL of dark red, free fluid was observed, along with more than 10 yellow-white polypoid nodules or papillary formations, with a maximum diameter of 1.5 cm, on the surface of the round ligament, sacrum ligament, right fallopian tube, and both sides of the uterus. No obvious abnormality was found in the appearance of the left fallopian tube and bilateral ovaries, whereas the surface of the right fallopian tube was covered in miliary tumors of different sizes. The serous surface lesions of the fallopian tube were removed and sent to the lab for pathological analysis. The pathology report indicated WDPM with adenomatoid tumor (Figure 1). Immunohistochemical staining showed that the lesions were positive for AE1/AE3, vimentin, cytokeratin 5/6 (CK5/6), calretinin, podoplanin (D2-40), Wilms’ tumor protein (WT-1), p53 (>50%), and Ki-67 (<15%); partially positive for Pax-8; and negative for desmin, estrogen receptor (ER), progesterone receptor (PR), and carcinoembryonic antigen (CEA) (Figure 2). The patient was monitored by computed tomography and serum CA125 level for 49 months with no recurrence.
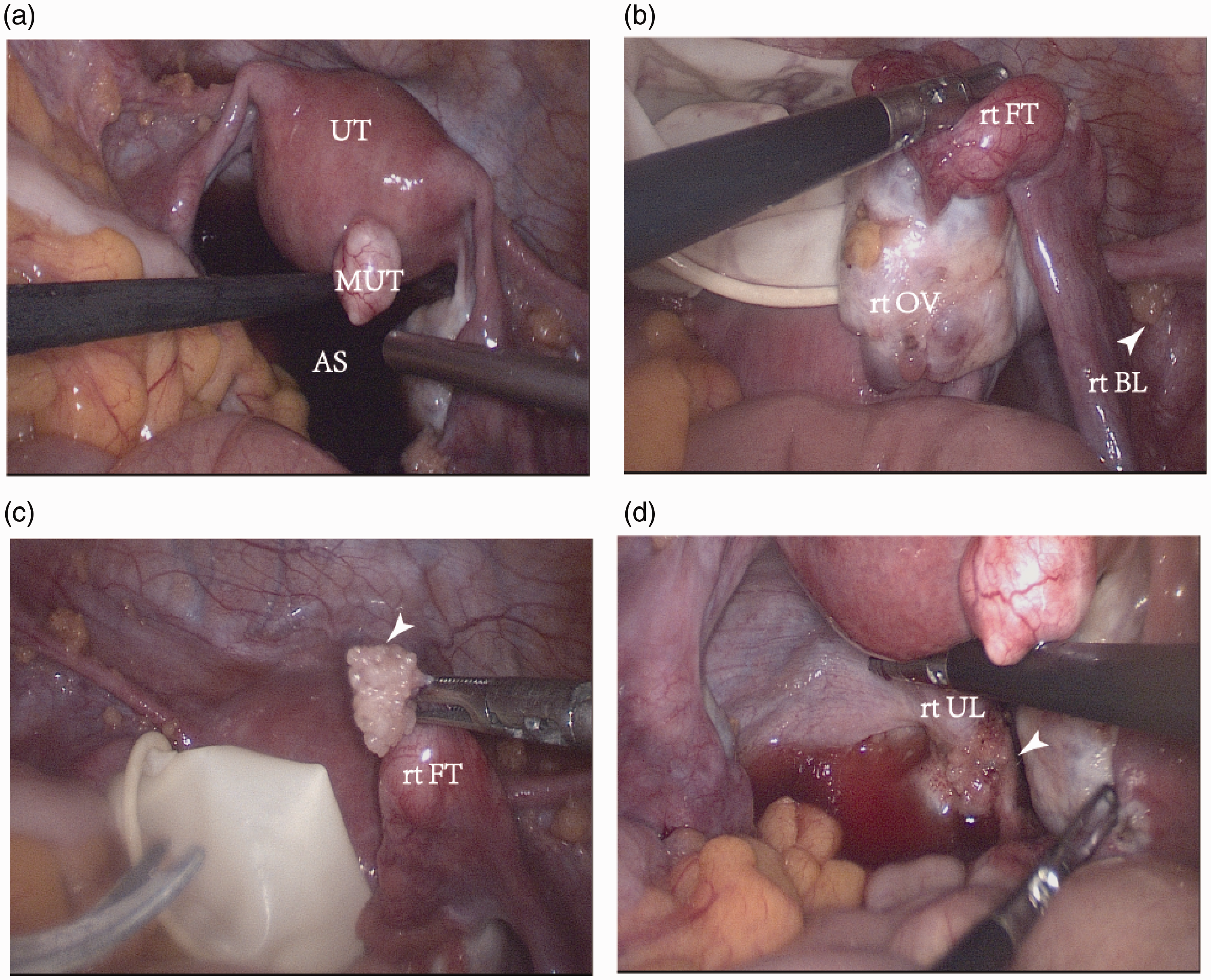
Laparoscopic images, with arrows indicating well-differentiated papillary mesothelioma (WDPM).

Photomicrographs of hematoxylin and eosin (h&e; panels a and b, 200× and 400× magnification, respectively) and immunohistochemical stains (panels c–k, 200× magnification). Positive staining for vimentin (c) and AE1/AE3 (d) illustrated tumor character and epithelial origin; positive results for other stains confirmed a mesothelial proliferation: cytokeratin 5/6 (CK5/6) (e), calretinin (f), podoplanin (D2-40) (g), and Wilms’ tumor protein (WT-1) (h). Staining for p53 was >50% positive (I) and staining for Ki-67 was <15% positive (j). Partly positive staining for Pax-8 (k) was helpful in the differential diagnosis.
Discussion
There are rare case reports of WDPM progressing to true malignant peritoneal mesothelioma. Clinically, WDPM is often discovered incidentally during pelvic examination or surgery. Imaging features of WDPM are not well documented, but complete resection, when possible, usually leads to normal survival.1,4–6 Genome-wide sequencing analysis shows that WDPM has a genetic profile distinct from that of malignant mesothelioma, with a lack of copy number alterations in genes characteristic of peritoneal and pleural mesothelioma: BAP1, SETD2, PBRM1, SMARCC1, CDKN2A/B, LATS1/2, and NF2.7,8 Adenomatoid tumors are also relatively uncommon benign tumors of mesothelial origin that usually occur in the male or female genital tract. 9 Although the American Society of Clinical Oncology published a clinical practice guideline on fertility preservation for adults and children with cancer in 2006, which has been updated periodically,10,11 therapeutic strategies for WDPM with adenomatoid tumor are not currently described. Therefore, treatment that allows patients with WDPM with adenomatoid tumor to become pregnant is a new challenge.
Ovulation, good oviduct function, a suitable endometrium for embryo implantation, and appropriate luteal support before and after pregnancy are prerequisites for pregnancy. In the present case, although the patient had natural ovulation, the surface of the right fallopian tube was covered with miliary tumors of different sizes, which may have affected fallopian tube function. Moreover, salpingography showed that one side of the fallopian tube was blocked, which reduced the probability of pregnancy by 50%. Immune and other factors cannot be excluded as possible causes of the patient’s 12-year history of infertility. In vitro fertilization is the first choice for treating infertility. However, it is not known whether the process of oocyte retrieval in a case such as that described here could lead to pelvic tumor spread and whether an invisible tumor implanted on the surface of the ovary could migrate inside the ovary. There are no reports on the effect of estrogen and progesterone on the prognosis of WDPM. Estrogen has been shown to aggravate disease progression in multiple cancer cell lines and mouse models, such as lung cancer, gastric cancer, skin cancer, and others. 12 Therefore, caution is required when considering adding or stimulating the production of supraphysiological estrogen for these patients.
Conclusions
Although our patient’s diagnosis does not affect her daily life, she has been infertile for 12 years and cannot become pregnant using assisted reproductive technology because of the lack of effective radical treatment for WDPM. Over time, ovarian failure may occur and the patient may never achieve fertility. This is an urgent problem that infertility doctors should address.
Supplemental Material
sj-pdf-1-imr-10.1177_0300060520986680 - Supplemental material for Peritoneal well-differentiated papillary mesothelioma associated with infertility in a 37-year-old woman
Supplemental material, sj-pdf-1-imr-10.1177_0300060520986680 for Peritoneal well-differentiated papillary mesothelioma associated with infertility in a 37-year-old woman by Bo Pang, Cong Hu, Qian Liu, Jinyu Yu, Zhentong Wei and Xiaowei Yu in Journal of International Medical Research
Footnotes
Author contributions
Xiaowei Yu conceived of and supervised the study; Jinyu Yu curated the data; Qian Liu and Zhentong Wei provided resources; Bo Pang wrote the original draft; and Cong Hu reviewed and edited the manuscript.
Ethics statement
Written informed consent was obtained from the patient for participation in the study and publication of this case report, and the Ethics Committee of the First Hospital of Jilin University approved the study.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.