
Abstract
Patients with several concurrent illnesses often present with complex manifestations and therefore receive a variety of treatments. The purpose of this report was to describe a patient diagnosed with hypothyroidism, Hashimoto’s encephalopathy, cerebral infarction, and ventricular arrhythmia. The patient also had multiple physiological and psychological disorders, including dizziness, frequent ventricular premature beats, hypotension, anxiety, and insomnia. Among other treatments, the patient received a stellate ganglion block and most symptoms were substantially alleviated. Therefore, stellate ganglion block appears to be a useful approach for treating perplexing clinical conditions in patients with autonomic dysfunction.
Keywords
Introduction
Patients diagnosed with more than one disease often exhibit complicated symptoms and tend to require various therapeutic approaches. However, potential conflicts between different treatment strategies may compromise outcomes and exacerbate the side effects of individual treatments. Therefore, an approach for treating multiple illnesses is needed.
The stellate ganglion is an aggregation of the inferior cervical ganglion and the first thoracic sympathetic ganglia located at the level of the sixth and seventh cervical vertebrae. This structure is part of the sympathetic nervous system governing the face and arm, but it does not control feeling or movement. Trauma or infection can sensitize these nerves, inducing a sense of pain.
Stellate ganglion block (SGB) is achieved by injecting a local anesthetic around the structure; this reduces the sympathetic activity of the stellate ganglion. SGB has shown clear benefits in several painful conditions such as refractory angina, ischemic pain in the upper limb from peripheral vascular disease, and regional pain syndrome.1,2 More recently, preoperative SGB was used as an analgesic to reduce postoperative pain. Furthermore, angioneurotic impairments, reflex sympathetic dystrophy, and ophthalmologic and otolaryngologic diseases are all reported to respond to SGB. Refractory ventricular arrhythmia and sweating in the face, head, arms, and hands can be relieved by SGB. 3
In psychological terms, a dysfunctional sympathetic tone constitutes one of the main features of posttraumatic stress disorder (PTSD), which manifests as hyperarousal with a defective relaxation response. SGB has been used to treat this disorder and relieve sympathetic hyperactivity in the long term.4,5 This fast-acting, somatic approach can reduce the barriers that prevent patients from receiving therapy, which are frequently encountered in the treatment of anxiety and insomnia, 6 particularly among the military population. Most patients who benefit from SGB present with only one or two symptoms. However, in this study, we used SGB to treat a patient who had several physiological and psychological disorders. Most of the patient’s symptoms were relieved, demonstrating the advantages of this approach for handling complex clinical situations.
Case report
A 36-year-old female patient visited the hospital for dizziness, palpitations, insomnia, and anxiety. She had been diagnosed with hypothyroidism, Hashimoto’s encephalopathy, cerebral infarction, and frequent ventricular premature beats 5 years earlier. Since her diagnosis, she had visited the hospital multiple times. After admission, the patient underwent magnetic resonance imaging and magnetic resonance angiogram examinations, which showed multifocal ischemic infarctions in the brain. Dynamic electrocardiography (ECG) revealed frequent ventricular premature beats (Figure 1a). The patient exhibited evident anxiety and therefore received drug interventions in the form of levothyroxine sodium (50 µg, once a day), zolpidem (10 mg, once a night), buspirone (5 mg, twice a day), and pregabalin (75 mg, twice a day), which induced only a brief remission. The dizziness, palpitations, sweating, sleeplessness, and emotional anxiety remained significant. After discussion, the patient agreed to undergo a 7-day SGB treatment using 4 mL of 1% lidocaine, which was administered around the stellate ganglion under ultrasound guidance on the left or right side, alternating each day. The stellate ganglions on both sides were not blocked simultaneously. Horner’s syndrome occurred within 5 minutes after each manipulation and was transient. The first SGB markedly improved the patient’s sleep quality, with her subsequent sleep time exceeding 9 hours a day. The patient’s dizziness subsided substantially after the second SGB. The 24-hour dynamic ECG showed that the ventricular premature beats decreased from 1633 to 267 per 24 hours, and the paroxysmal ventricular bigeminy decreased from 154 to 39 per 24 hours (Figure 1b, Table 1). The patient’s ambulatory maximum blood pressure (systolic/diastolic) varied from 172/109 mmHg (mean 130 mmHg) to 183/108 mmHg (mean 130 mmHg) (Table 2), and the minimum blood pressure improved from 80/38 mmHg (mean 52 mmHg) to 100/71 mmHg (mean 80 mmHg) (Table 2). All other symptoms were alleviated and stabilized. After 7 days of SGB adjuvant treatment, the patient was discharged.

Electrocardiograms of the patient before (a) and after (b) stellate ganglion block.
Twenty-four-hour dynamic electrocardiogram before and after SGB treatment.
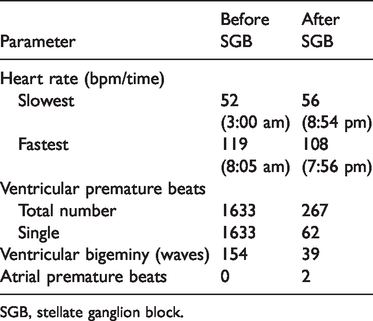
SGB, stellate ganglion block.
Twenty-four-hour ambulatory blood pressure before and after SGB treatment.

SGB, stellate ganglion block; S, systolic blood pressure; D, diastolic blood pressure; CV, coefficient of variation.
Discussion
SGB has been reported to be effective for patients with specific but not mixed symptoms. The patient in this case exhibited complex physiological and psychological disorders but still gained clear benefits from SGB.
SGB improves the functions of both the central and peripheral nerves, which maintain the body’s autonomic nervous activity, endocrine potency, and immune actions. The SGB procedure regulates the status of the hypothalamus and stabilizes secretion of pituitary hormones by increasing local blood flow, which increases the content of norepinephrine and elevates blood pressure. 7 Our findings suggest that SGB can reverse hypotension and minimize fluctuations in blood pressure. Moreover, the remission of dizziness in our patient may have resulted from the elevation of blood pressure caused by SGB.
Previous studies have shown that SGB reduces the frequency of ventricular tachycardia, thereby improving a patient’s systolic cardiac function, reducing the need for electrical defibrillation, and suppressing the formation of an ECG storm. 8 Additionally, premature ventricular contractions and bigeminy are controlled by SGB. In the present case, ventricular arrhythmia was substantially mitigated by SGB, in line with other reports and confirming the advantages of this treatment in restoring the cardiac autonomic nerve actions.
Patients with sleep disorders often exhibit an imbalance between sympathetic and parasympathetic potency, with the former boosted and the latter suppressed. Recently, the effect of SGB on PTSD was thoroughly evaluated, and SGB was found to significantly relieve sympathetic hyperactivity. Clinical symptoms and psychological scale scores of patients with PTSD treated with SGB improved considerably, with patients sleeping better and remaining in a more stable emotional state than before treatment.4,5 Our patient exhibited a marked improvement in sleep after receiving SGB, indicating that even for patients with a complicated and severe clinical presentation, SGB can provide visible benefits.
The height and weight of the patient in this study were 156 cm and 35 kg, respectively. Because of her small body size, 4 mL of 1% lidocaine was used, and the target area was infiltrated thoroughly. Previous studies have shown that SGB on the left side has a better therapeutic effect on heart disease, 9 whereas SGB on the right side improves mental and psychological disorders. 10 This patient received SGB four times on the left side and three times on the right side, and satisfactory therapeutic effects on the patient’s circulatory system and psychological disorders were achieved. Adverse effects such as hoarseness and loss of speech were avoided. However, for larger patients, a higher dose of lidocaine or more potent local anesthetics such as 0.5% ropivacaine or bupivacaine may be used.
In this case, following SGB and pharmacological therapy, the ventricular premature beats exhibited by the patient decreased significantly, her blood pressure stabilized, and her sleep improved. This result demonstrates that patients with complex physiological and psychological disorders can obtain clear benefits from SGB.
Supplemental Material
sj-jpg-1-imr-10.1177_0300060520985645 - Supplemental material for Treatment of multiple physiological and psychological disorders in one patient with stellate ganglion block: a case report
Supplemental material, sj-jpg-1-imr-10.1177_0300060520985645 for Treatment of multiple physiological and psychological disorders in one patient with stellate ganglion block: a case report by Yunyao Xu and Yuenong Zhang in Journal of International Medical Research
Footnotes
Ethics statement and informed consent
This study was approved by the Ethics Committee and Institutional Review Board of The Third Affiliated Hospital of Sun Yat-sen University-Yuedong Hospital, Guangdong, China (Number: 2020-11). The patient provided informed consent for publication of this case report. Our study followed the CARE guidelines listed at ![]() .
.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.