
Abstract
Objective
This prospective study was performed to explore the change in sacrococcygeal pressure during an operation under general anesthesia in the supine position and identify the correlation between pressure injury and body mass index.
Methods
This study involved 99 patients who underwent general anesthesia. Sacrococcygeal pressure was measured and recorded at seven time points: before general anesthesia, 5 minutes after general anesthesia, and 1, 2, 3, 4, and 5 hours after the beginning of the operation. The pressure change at each time point was compared, and the factors affecting the pressure were analyzed.
Results
The correlation analysis showed that the operation time was significantly and positively associated with the occurrence of pressure injury.
Conclusion
Perioperative management should be strengthened to speed up the surgical process and shorten the operation time, which will help to reduce the occurrence of intraoperative pressure injury.
Keywords
Introduction
Pressure injury (PI), also known as a pressure ulcer, pressure sore, or bedsore, is a localized injury that occurs in the skin and/or subcutaneous soft tissue, usually over a bone hump or area of contact between the skin and medical equipment. 1 The incidence of PI reportedly ranges from 7.1% to 27.0%,2,3 and 23% of PI that occurs during hospitalization is related to surgery. 4 Patients undergoing surgery are at high risk of PI during hospitalization, and the incidence of PI in this setting is as high as 4.7% to 66.0%. 5 Once PI has occurred, it not only affects patients’ postoperative recovery and prolongs their hospitalization time, but it also causes medical disputes and affects the quality of nursing services. 6 Therefore, the prevention and management of PI has become a research focus of nursing in the operating room. However, studies both in China and abroad have confirmed that the occurrence of intraoperative PI is related to sacrococcygeal pressure, age, body mass index (BMI), operation time, skin condition, operation position, and other factors.7,8
Scholars worldwide have also studied the development of PI through a large number of animal experiments7,9; however, no statistical data are yet available to clarify how the duration of surgery and other factors affect changes in pressure leading to PI. 10 Therefore, this study was performed to analyze the correlation between sacrococcygeal pressure changes and age, BMI, operation time, and other factors in patients undergoing operations in the supine position under general anesthesia. We anticipate that our findings will provide a basis for clinicians to take targeted measures that will reduce the incidence of intraoperative PI, improve the quality of care, and ensure the safety of patients.
Patients and methods
Patients
This prospective study was approved by the Ethics Committee of Sichuan Cancer Hospital and Institute, Sichuan Cancer Center, School of Medicine, University of Electronic Science and Technology of China (9 January 2018), and informed consent was obtained from all patients and their families. Ninety-nine patients who underwent general anesthesia in our hospital from March 2018 to March 2019 were included in this study. The inclusion criteria were surgery under general anesthesia in the prone position and voluntary participation. The exclusion criteria were a history of PI before surgery and refusal to participate.
Detection of sacrococcygeal pressure
The pressure in the sacrococcygeal region, which is the most common site of PI, was measured in patients undergoing general anesthesia in the supine position.5,6 The patient’s position and the position of the measuring device remained unchanged during the measurement. In addition, the temperature and humidity of the operating room were strictly maintained at 22°C and 55%, respectively, and the patient’s bed unit and clothes remained dry, flat, and free of wrinkles. Measurements were performed with a portable contact pressure tester containing an airbag (CR-490; Eunipas, Nagasaki, Japan). The measuring range was 0 to 200 mmHg, and the measurement accuracy was ±3 mmHg. Before anesthesia, the pressure sensor of the pressure-measuring device was placed under the skin in the sacrococcygeal region. The main engine of the pressure-measuring device was placed beside the operating table in the effective standby state. To perform the measurement, the power key and measurement key of the pressure-measuring device were activated.
Data collection
Before and after anesthesia, we recorded the patients’ general information, including their sex, age, BMI, operation time, anesthesia time, and intraoperative bleeding volume. The sacrococcygeal pressure was measured and recorded at seven time points: before general anesthesia, 5 minutes after general anesthesia, and 1, 2, 3, 4, and 5 hours after the beginning of the operation. Because the operation times differed among the patients, 99 sacrococcygeal pressure measurements were collected at three time points (before anesthesia, 5 minutes after induction of anesthesia, and 1 hour after the beginning of the operation). Furthermore, 42 measurements were collected 2 hours after the beginning of the operation, 14 measurements were collected 3 hours after the beginning of the operation, 6 measurements were collected 4 hours after the beginning of the operation, and 3 measurements were collected 5 hours after the beginning of the operation.
Statistical analysis
The statistical analysis was performed using IBM SPSS Statistics for Windows, Version 22.0 (IBM Corp., Armonk, NY, USA). Count data are expressed as a percentage. Measurement data conforming to a normal distribution are expressed as mean ± standard deviation. Pearson correlation analysis was used to analyze the correlation between variables.
Results
General clinical data
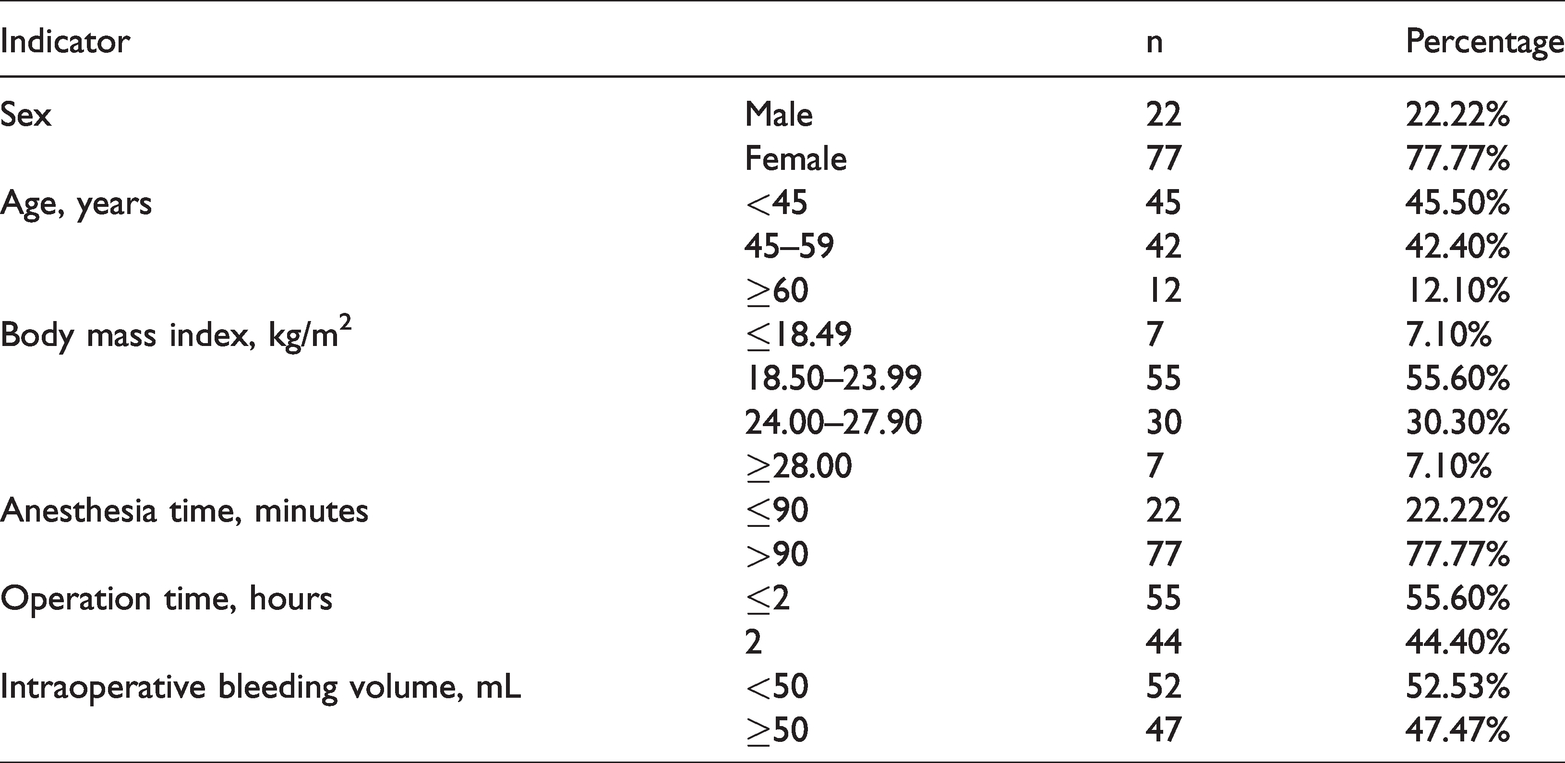
This study involved 99 patients (22 men and 77 women). Their mean age was 56.7 ± 12.3 years, and their mean BMI was 23.05 ± 3.33 kg/m2. The anesthesia time ranged from 1 to 2 hours, the operation time ranged from 0.33 to 10.33 hours, and the intraoperative bleeding volume ranged from 5 to 900 mL. These results are summarized in Table 1.
General clinical characteristics of patients undergoing general anesthesia.
Comparison of sacrococcygeal pressure at different time points
The sacrococcygeal pressure was measured at seven time points, and the mean pressures are shown in Table 2. The results showed that the sacrococcygeal pressure was highest 5 hours after the operation. In addition, the trend of the change in the sacrococcygeal pressure at different time points is shown in Figure 1. The pressure was higher after the beginning of the operation than before anesthesia. As the operation progressed, the average pressure at the five time points after anesthesia was higher than that before anesthesia.
Comparison of sacrococcygeal pressure at different time points.

SD, standard deviation.

Trend of changes in sacrococcygeal pressure at different time points.
Correlation of sacrococcygeal pressure with sex, age, and operation time
As shown in Table 3, there was no statistical correlation of the intraoperative sacrococcygeal pressure with sex, age, BMI, anesthesia time, or intraoperative blood volume in patients undergoing general anesthesia in the supine position. However, a statistical correlation was found between the operation time and intraoperative sacrococcygeal pressure in the supine position (r = 0.258, P = 0.010). A regression analysis was performed to analyze the sacrococcygeal pressure and operation time in the supine position; the regression equation was y = 3.843x + 28.777, where y was the sacrococcygeal pressure and x was the operation time variable.
Factors influencing sacrococcygeal pressure.

Discussion
The normal capillary interface pressure is 22 to 32 mmHg. When the external pressure repeatedly exceeds this range within a short period of time, capillary occlusion and tissue ischemia are likely to develop. 11 In the clinical setting, the pressure of the contact surface is used as an index to predict and prevent PI. 12 Landis 13 found that when the contact surface pressure was >32 mmHg, PI readily occurred. In the present study, the sacrococcygeal pressure of patients undergoing general anesthesia was >32 mmHg at different time points. Our results are consistent with those of other studies.14,15 Therefore, for patients undergoing general anesthesia in the supine position, the sacrococcygeal area should be protected because it is at high risk of PI, and the skin of the sacrococcygeal area should be protected to prevent PI.
In this study, the average sacrococcygeal pressure after anesthesia was higher than that before anesthesia, and the average sacrococcygeal pressure from 1 to 5 hours after the beginning of the operation gradually increased. Pearson correlation analysis showed that sex, age, BMI, anesthesia time, and intraoperative bleeding were not correlated with intraoperative sacrococcygeal pressure. However, a positive correlation was found between the operation time and sacrococcygeal pressure in patients undergoing general anesthesia. Studies have shown that maintenance of a position for a long period of time in patients undergoing surgery will cause certain parts of the body to be under prolonged pressure, leading to blood and oxygen supply disturbances and even skin necrosis. 16 Gebhardt 17 found a parabolic relationship between pressure and duration; specifically, skin ulcers more rapidly formed under high than low pressure. In the present study, the highest sacrococcygeal pressure recorded after the beginning of the operation was 61.16 mmHg. Considering that pressure is positively correlated with the operation time, the pressure at the compression site is also positively correlated with the incidence of injury. 16 One study showed that under pressure of 70 mmHg (1 mmHg = 0.133 kPa), tissue can undergo irreversible damage if it is continuously compressed for more than 2 hours. 18 Necrosis of muscle will occur after 4 hours under 500 mmHg of pressure, and skin necrosis will occur after 16 hours under 200 mmHg of pressure or after 8 hours under 800 mmHg of pressure. 19 These findings suggest that as the operation time increases, skin pressure increases and the risk of PI therefore also increases. Through preoperative preparation and active intraoperative team cooperation, patients can undergo the operation in the shortest possible time, which will reduce the risk of PI. This is important to ensure early rehabilitation of patients and to improve the satisfaction of patients and nursing quality. The incidence of intraoperative PI is also an important index of modern nursing quality evaluation.
One limitation of this study is that we did not perform a sample size calculation. Another limitation is that the limited number of patients and insufficient stratification may have affected the statistical significance of the results.
In conclusion, the pressure in the sacrococcygeal region in the supine position increased with the operation time, and a positive correlation was noted. However, further studies with larger sample sizes are needed.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the Scientific Research Project of Sichuan Health Committee (No. 16PJ519).