
Abstract
Objective
We aimed to determine the physiological and hemodynamic changes in patients who were undergoing hyperthermic intraperitoneal chemotherapy (HIPEC) cytoreductive surgeries.
Methods
This prospective, observational study enrolled 21 patients who were undergoing elective cytoreductive surgery with HIPEC at our hospital over 2 years. We collected vital signs, hemodynamic parameters including global end-diastolic volume index (GEVI) and extravascular lung water index (ELWI) using the VolumeView™ system, and arterial blood gas analysis from all patients. Data were recorded before skin incision (T1); 30 minutes before HIPEC initiation (T2); 30 (T3), 60 (T4), and 90 (T5) minutes after HIPEC initiation; 30 minutes after HIPEC completion (T6); and 10 minutes before surgery completion (T7).
Results
Patients showed an increase in body temperature and cardiac index and a decrease in the systemic vascular resistance index. GEDI was 715.4 (T1) to 809.7 (T6), and ELWI was 6.9 (T1) to 7.3 (T5).
Conclusions
HIPEC increased patients’ body temperature and cardiac output and decreased systemic vascular resistance. Although parameters that were extracted from the VolumeView™ system were within their normal ranges, transpulmonary thermodilution approach is helpful in intraoperative hemodynamic management during open abdominal cytoreductive surgery with HIPEC.
URL: https://clinicaltrials.gov/ct2/results?cond=NCT02325648&term
Keywords
Introduction
Peritoneal carcinomatosis involves the spread of a tumor over the peritoneal surface secondary to the seeding of gynecologic and non-gynecologic tumors in the peritoneum. It is difficult to treat, and treatment outcomes are poor.1,2 Recently, cytoreductive surgery with hyperthermic intraperitoneal chemotherapy (HIPEC) has been reported to be an effective treatment approach for peritoneal cancer, and several studies have demonstrated a significantly enhanced survival rate with this treatment approach.3–6 HIPEC involves the direct administration of highly concentrated anti-cancer agents into the tumor tissue via a glucose carrier solution at high temperature. This stresses the cardiovascular system, resulting in an increase in the heart rate (HR), cardiac index (CI), and oxygen consumption and a decrease in the systemic vascular resistance index (SVRI).7–9 Therefore, the continuous monitoring of arterial blood pressure and central venous pressure (CVP) is important, and in certain cases, vasopressors and inotropic agents are recommended to maintain the blood pressure. 10
In addition, appropriate fluid management and the maintenance of urinary output are critical because massive fluid shifts and circulating intravascular volume loss frequently occur during surgery.11–13 The wide extent of surgical resection and physicochemical trauma, as well as HIPEC, alters capillary permeability, resulting in tissue damage and facilitating abdominal and systemic complications, with postoperative morbidity and mortality rates ranging from 22% to 41% and 2% to 5%, respectively.14,15 However, there is insufficient information available from previously published studies on the anticipated metabolic and physiologic derangement for anesthesiologists. The VolumeView™ system (Edwards Lifesciences), which uses a novel algorithm for the mathematical analysis of the thermodilution curve, 16 has been recently introduced. Precise physiological parameters, such as the global end-diastolic volume index (GEDI), extravascular lung water index (ELWI), and pulmonary vascular permeability index (PVPI), can be derived from the dilution curve. Therefore, this system can provide more precise information for hemodynamic alteration during major abdominal surgery and assists in the management of fluid supply to high-risk patients with issues between fluid restriction and overloading.
The present study aimed to investigate the physiological changes, including the new transpulmonary thermodilution approach with the VolumeView™ system, in patients who are undergoing cytoreductive surgery with HIPEC.
Methods
Patients
This was a single-center, prospective, observational study. The study protocol was approved in accordance with the ethical standards of the Severance Hospital Research Ethics Committee and Institutional Review Board (IRB number: 4-2014-0854). Additionally, the study was registered at ClinicalTrials.gov (NCT02325648). This study was conducted in accordance with the World Medical Association Declaration of Helsinki. Furthermore, the submitted manuscript conforms to the ICMJE Recommendations for the Conduct, Reporting, Editing, and Publication of Scholarly Work in Medical Journals. All patients provided written informed consent before they were enrolled into the study, which occurred when the patients were informed of the study objectives and methods 1 day before the surgery. Adult patients who were undergoing elective cytoreductive surgery with HIPEC at our hospital between December 2014 and April 2016, were assessed for eligibility. The exclusion criteria were a sudden change in the surgical plan and the retraction of consent.
Anesthesia
Upon arrival in the operating room, routine monitoring was started, including electrocardiography, pulse oximetry, noninvasive blood pressure monitoring, and capnography. Anesthetic depth was monitored using a bispectral index (BIS) monitor (Aspect A-2000™, Aspect Medical System Inc., Newton, MA, USA). Anesthesia induction occurred through a bolus administration of 1.5 to 2 mg/kg of propofol and 1 to 2 µg/kg of remifentanil. Anesthesia was maintained using 4% to 7% desflurane with an adjuvant intravenous (IV) infusion of 0.05 to 0.2 µg/kg/minute of remifentanil. Rocuronium, which is a neuromuscular relaxing agent, was injected at 0.6 mg/kg to facilitate tracheal intubation in all patients. Tracheal intubation was performed in female and male patients using a 6.5-mm and 7.5-mm (internal diameter) tracheal tube, respectively. The cuff pressure of the tracheal tube was maintained at 20 to 25 cm H2O throughout the procedure. Mechanical ventilation was maintained with a tidal volume of 8 mL/kg of ideal body weight, and the ventilatory frequency was adjusted to maintain an end-tidal CO2 concentration of 35 to 45 mmHg with an air/oxygen mixture (fraction of inspired oxygen, 0.5). BIS scores were maintained in the range of 40 and 60, and the mean arterial pressure was maintained within 20% of the pre-induction value. In all patients, a central venous catheter was inserted for additional venous access and hemodynamic monitoring.
HIPEC procedure
All patients underwent cytoreductive surgery followed by HIPEC. For HIPEC, the open abdomen technique was used, allowing surgeons to manipulate abdominal contents. Inflow and outflow tubes were connected to a hyperthermia pump. Preheated 5% glucose peritoneal dialysis solution (1000 mL/minute) was circulated through the abdominal cavity. When the target temperature of 41°C to 42°C was reached, chemotherapeutic agents were added to this solution. HIPEC was scheduled for 90 minutes. The perfusate was then drained and the abdominal cavity was washed out with 4000 mL of normal saline.
Measurements
A VolumeView™ catheter (Edwards Lifesciences, Irvine, CA, USA) was inserted into the left or right femoral artery and connected to the EV 1000 monitoring system (Edwards Lifesciences). Thermodilution measurements were performed in sets of at least three consecutive injections of 15 to 20 mL cold saline, which were randomly distributed over the respiratory cycle. All hemodynamic data were electronically recorded at 100 Hz internally in the EV 1000 system and downloaded for analysis. Hemodynamic parameters, such as CI, stroke volume index (SVI), SVRI, and stroke volume variation (SVV), were continuously measured using the EV 1000 monitor, and new additional hemodynamic data, such as the GEDI, ELWI, and PVPI, were extracted. These volumetric parameters were calibrated and obtained when cold saline was infused to perform the thermodilution measurements. In addition, we defined the following seven time points: before skin incision (T1); 30 minutes before HIPEC (T2); 30 (T3), 60 (T4), and 90 (T5) minutes after HIPEC initiation; 30 minutes after HIPEC completion (T6); and 10 minutes before surgery completion (T7), to describe the course of the intervention. Laboratory test results and arterial blood gas analysis (ABGA) results were also recorded.
Fluid resuscitation
The amount of serious intravascular volume loss during surgery was estimated by the investigator and was equally substituted with additional crystalloid infusion. We recorded the detectable amount of blood loss in the suction unit during surgery but did not estimate the blood that was absorbed in the abdominal compresses. An isotonic HES preparation (Volulyte®, Fresenius Kabi AG, Bad Homburg, Germany) was administered to compensate for blood loss. The transfusion of red cell concentrates was considered when the hemoglobin level decreased below 8 g/dL. A continuous infusion of vasopressor was routinely used to maintain the mean arterial pressure at not more than 20% below the baseline value during surgery. All patients received a transurethral urine catheter, and urine output was measured hourly. Diuretics were not used during surgery.
Body temperature control
Body temperature was continuously measured with a thermodilution prove in the VolumeView™ catheter. Patients were warmed with a BairHgger™ upper body airstream blanket (3M GmbH, Neuss, Germany), hot line, and heated circuit during cytoreductive surgery. Patients were cooled with a BairHgger™ upper body airstream blanket (3M GmbH) and cold IV fluids to maintain normal body temperature during HIPEC.
Postoperative data
We collected postoperative patient data, including coagulation profiles (platelet count, prothrombin time, and partial thromboplastin time), serum albumin levels, renal function profiles, respiratory function restoration, bowel movement recovery, complications, and the length of intensive care unit (ICU) and hospital stays. We elucidated the occurrence of acute kidney injury (AKI) in accordance with the RIFLE (Risk, Injury, Failure, Loss, and End-stage Kidney Disease [ESKD]) criteria. The criteria are based on an elevated serum creatinine level and decreased estimated glomerular filtration rate and urinary output compared with baseline, and they have been used to define AKI and classify patients on the basis of the AKI severity. 17 Bowel movement recovery was evaluated on the basis of the gas passing time, sips of water time, and soft diet time. Postoperative complications included surgical complications that required re-operation during the hospital stays, and non-surgical complications that required conservative care.
Statistical analysis
Descriptive analyses were performed to demonstrate patient characteristics. Continuous variables are reported as the mean (standard deviation or range), and categorical variables are reported as the number of subjects (percentage). All descriptive statistics were obtained using SPSS (SPSS version 23.0; IBM Corp., Armonk, NY, USA).
Results
Patient characteristics
Among 31 patients who were scheduled to undergo cytoreductive surgery with HIPEC, 22 patients who provided consent were enrolled between November 2014 and April 2016. Among these 22 patients, one patient was excluded because of a change in the surgical plan. The remaining 21 patients were included in the analysis. Table 1 presents the patient demographic data. The average age of the patients was 59.0 ± 11.7 years, and there were 13 men and eight women who were included in the analysis. Colon cancer was the most common cause of peritoneal cancer in our study population. The other causes included appendix cancers, sigmoid cancers, and rectal cancers. The departments of Hepatobiliary and Pancreas Surgery and Urologic Surgery cooperated for the colorectal surgery.
Patient characteristics.

Data are presented as the mean (standard deviation) or number (percentage).
ASA, American Society of Anesthesiologists.
Intraoperative management
The anesthetic duration was nearly 12 hours. For postoperative pain control, 17 patients received IV patient-controlled analgesia (PCA) and the remaining four patients received epidural PCA. Fluid was administered with total crystalloid at 6983.3 mL and total colloid at 1177.2 mL. The urine output was maintained at 122 mL/hour, and the estimated blood loss (EBL) was 780 mL. To decrease the glucose level, rapid insulin (6.8 IU) was administered IV. In most patients (20/21), vasopressors were used, and phenylephrine was infused in 70% of the patients (Table 2).
Intraoperative parameters.
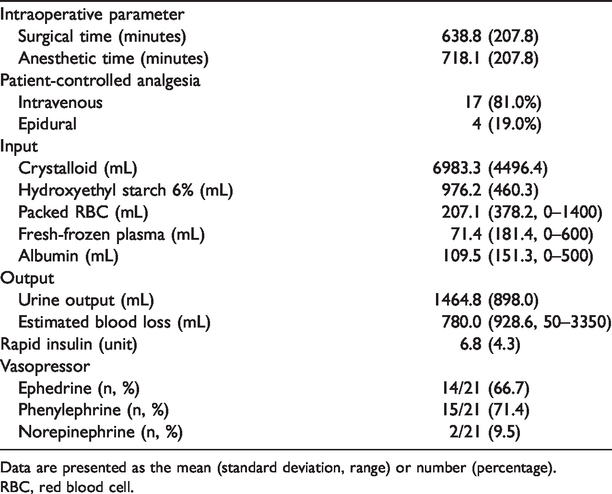
Data are presented as the mean (standard deviation, range) or number (percentage).
RBC, red blood cell.
Intraoperative hemodynamic, respiratory, and metabolic parameters
Table 3 presents the various intraoperative parameters, including physiological changes. During the HIPEC 90-minute period, hyperthermia occurred with a mean overall peak body temperature of 38.0°C. The mean blood pressure decreased to 76 mmHg and HR increased to 95 bpm until HIPEC completion. Additionally, the CI increased to 3.8, SVI increased to 5.2, and SVV increased to 11.4 during HIPEC. Their peak levels did not occur at the same time point. In advanced hemodynamic monitoring, the ELWI, PVPI, and GEDI increased overall during HIPEC and changed significantly over time. The SVRI decreased to 1326.8, and it remained low until the end of surgery. In accordance with ABGA, the serum lactate level increased by four-times compared with the initial baseline level, and the serum glucose level increased by 2.5-times compared with the initial level.
Intraoperative hemodynamic, respiratory, and metabolic variables.

Data are presented as the mean (standard deviation).
T1, before skin incision; T2, 30 minutes before HIPEC; T3, 30 minutes after HIPEC initiation; T4, 60 minutes after HIPEC initiation; T5, 90 minutes after HIPEC initiation; T6, 30 minutes after HIPEC completion; and T7, 10 minutes before surgery completion.
BT, body temperature; HR, heart rate; MBP, mean arterial pressure; CVP, central venous pressure; CI, cardiac index; SVI, stroke volume index; SVV, stroke volume variation; SVRI, systemic vascular resistance index; GEDI, global end-diastolic volume index; ELWI, extravascular lung water index; PVPI, pulmonary vascular permeability index; ABGA, arterial blood gas analysis; PO2, partial pressure of oxygen; PCO2, partial pressure of carbon dioxide; HCO3, bicarbonate.
Postoperative recovery profile
For postoperative coagulation profiles (Table 4), the platelet count, prothrombin time, and partial thromboplastin time decreased compared with the preoperative levels. Additionally, the albumin level decreased after surgery. One patient experienced an acute deterioration of renal function in accordance with the RIFLE criteria during the hospital stay. Nine ICU patients received ventilation, and six patients were maintained with vasopressors upon ICU arrival. Three cases of postoperative complications, including adhesion, bleeding, and wound dehiscence, needed surgical treatments, while four patients with complications, including pancytopenia, pneumonia, and pancreas fistula, needed conservative treatments. The mean length of hospital stay was 18.5 days, and the mean length of ICU stay was 1.4 days. Two patients died within the study period (18 months).
Postoperative recovery profiles.

Data are presented as the mean (standard deviation, range) or number (percentage).
*Death during the study period.
PT, prothrombin time; INR, international normalized ratio; pTT, partial thromboplastin time; ICU, intensive care unit; SOW, sips of water; GPT, gas passing time; SDT, soft diet time; LOS, length of stay; POD, postoperative day.
Discussion
In our study, we prospectively described the physiological changes during open abdominal cytoreductive surgery with HIPEC. To the best of our knowledge, the present study is the first trial to examine the cardiopulmonary and intravascular volume status with a new thermodilution measurement approach using the VolumeView™ system in cytoreductive surgery with HIPEC.
A previous systemic review of patients with pseudomyxoma peritonei that was treated with cytoreductive surgery and HIPEC demonstrated that the median survival duration ranged from 51 to 156 months and that the 5-year survival rate ranged from 52% to 96% depending on the disease severity at the time of treatment.18,19 In addition, Verwaal et al. 20 reported that patients with peritoneal carcinomatosis secondary to colorectal cancer treated with cytoreductive surgery and HIPEC showed a significant increase in the median survival (22 months) compared with survival in patients who were treated with systemic chemotherapy alone (12 months). Consequently, cytoreductive surgery with HIPEC is currently recognized as the standard of care for managing peritoneal carcinomatosis secondary to colorectal or gynecological cancers in selected patients.8,21,22
Despite continuous improvements in surgical and anesthetic techniques, cytoreductive surgery with HIPEC is often associated with disturbances in hemodynamics, coagulation, respiratory exchange, and nutrition.7,23 Therefore, understanding the pathophysiological changes accompanying this procedure is crucial and helpful for patients who are undergoing anesthesia. There were three studies that systemically evaluated additional hemodynamic parameters, such as cardiac output and vascular resistance, which were assessed using either esophageal Doppler or transpulmonary thermodilution (TPTD) and pulse contour analysis.24,25 Although the results of the variation in systemic vascular resistance and cardiac output were not consistent and significant, 26 a decrease in the SVRI and an increase in the CI were only measured in patients during the HIPEC open coliseum technique, 27 which is consistent with our results.
Considering the duration of surgery, large fluid shifts, frequent requirement for vasopressor support, and intraoperative hemodynamic changes need constant and adequate attention, although they are transient in nature. The intraoperative monitoring of hemodynamics is multipronged, and across studies on cytoreductive surgery with HIPEC, the monitoring approaches that were used included at least a CVP line, invasive arterial pressure monitoring line, and hourly urine output assessment.28,29 However, the CVP and amount of urine are not accurate indices of fluid responsiveness, and they only help to detect a patient’s intravascular volume status.30–32 In addition, both the pulse pressure variation and SVV, which may exhibit faster responses to sudden changes in volume responsiveness, are calculated using an arterial pressure waveform analysis method. However, some studies have reported clinically unacceptable accuracy for these systems in patients with vasodilation or impaired systolic function during a hypovolemic state.33,34
To overcome these challenges, a new TPTD system was recently developed and introduced into clinical practice. It involves a specific thermistor-tipped arterial catheter, the VolumeView™ catheter, and the EV 1000 monitoring platform, and it uses a novel algorithm to mathematically analyze the thermodilution curve. 16 After injecting a cold indicator into the superior vena cava, TPTD allows the computation of cardiac output from a TPTD curve that was recorded using a thermistor-tipped femoral arterial catheter. 35 Volumetric preload indicators, such as the GEDI,36–38 have been shown to be the reliable indicators of cardiac preload and have been successfully implemented in therapeutic strategies that may improve outcomes. The GEDI ranged from 715.4 to 809.7 in the present study, and this level steadily increased during the HIPEC period because of fluid resuscitation for compensating a decreased SVRI and increased SVV and HR. The ELWI, which is measured with single indicator dilution, is a reliable measure of pulmonary edema that has been validated against postmortem gravimetric measurement in animals.39–41 Moreover, ELWI and PVPI may be used as criteria to indicate the risk of fluid administration. 42 In particular, ELWI ≥10 mL/kg was defined as pulmonary edema, although no definitive quantitative criteria for ELWI that are associated with pulmonary edema have been established. A previous human autopsy study reported that the normal ELWI value is approximately 7.4 (SD 3.3) mL/kg, and this value can distinguish between healthy and pathological lungs. 43 Because ELWI ranged from 6.9 to 7.3 (peak value during HIPEC) in our study, the risk of intraoperative pulmonary edema occurring that is related to the cytoreductive surgery with HIPEC was lower than anticipated. However, HIPEC would be a factor that interfered with the measurement of volumetric parameters.
During HIPEC, the circulation support with inotropes/vasopressors does not have definite recommendations. 30 The common practice in the setting of vasodilation was the use of noradrenaline and methoxamine, and it usually depends on institutional protocols. We almost selected and administered phenylephrine to our patients as a vasopressor because of increased HR and decreased SVRI. As a compensatory mechanism for the lower SVRI, increased cardiac output and HR were measured using Vigileo™ during HIPEC, which is consistent with previous reports.44,45 The SVRI remained low during HIPEC and postoperatively. In six patients, the vasopressor was maintained when they left the operating room.
The choice of intraoperative fluid infusion involves balanced infusion therapy to maintain the preload, colloid oncotic pressure, end-organ perfusion (urinary output), and electrolyte homeostasis. 10 To prevent hemodynamic imbalance and reductions in end-organ perfusion, the anesthesiologist’s main aim should be adequate fluid replacement, blood loss adjustment, and maintenance of euvolemia. Moreover, in surgery with HIPEC, AKI usually occurs because of a decrease in blood pressure and insufficiency of intravascular volume. With maintenance of normovolemia only and adequate urine output, no change in creatinine values occurred during cytoreductive surgery and HIPEC,12,46 and in our study, only one patient experienced AKI. It would be helpful to perform a comprehensive evaluation of a patient’s intravascular volume status with closed monitoring involving various approaches, including the use of the VolumeView™ system. 7
The severity of metabolic changes that were observed during HIPEC depends on the type of carrier solution and degree of hyperthermia. The carrier solution that was used in this study was a fluid containing 5% dextrose. Metabolic changes occur when both glucose and free water are absorbed into the plasma causing hyperglycemia and dilutional hyponatremia. 1 In our study, body temperature increased to 38°C for 2 hours during the HIPEC period. Hyperthermia has been shown to increase metabolic activity, HR, carbon dioxide production, and ultimately oxygen consumption. 7 Additionally, a previous study reported increases in the lactate level of 2 to 4 mmol/L. 47 Although the results of this study also showed elevated levels of glucose and lactic acid, the levels of electrolytes, such as sodium, were almost in the normal range. This result may be associated with closed monitoring and adequate fluid management, which is made possible by the new TPTD system.
After HIPEC, patients are often admitted to the ICU or are kept in the post-anesthesia care unit to monitor their organ function, manage intraoperative complications, and correct coagulopathy. Physiological perturbations during the perioperative period affect the duration of their ICU stay and may precipitate multisystem organ failure. 1 Although the length of ICU stay (1.4 days) in our study was similar to the length that was reported in other studies, postoperative complications after surgery were unavoidable in our study. For postoperative outcomes, there are many debates about the ideal postoperative nutrition strategies. A retrospective study by Arakelian et al. 48 showed that postoperative ileus is a common problem after surgery. Although there are no prospective studies, most patients were able to tolerate oral feeding between 7 and 11 days after surgery. To promote healing and improve intestinal transit, early enteral feeding is both safe and beneficial for patients.49–51 In our study, the recovery time for bowel movement was about 6 days, and the water and soft diet feeding times were shorter than the gas passing time.
Some limitations must be acknowledged. This was a prospective observational study, and the number of enrolled patients was relatively low. Consequently, the results of our study may not be generalizable. In addition, it may be more critical to investigate the course of pathophysiologic changes, including fluid redistribution, after HIPEC surgery compared with intraoperative conditions. However, our findings will be a valuable source of information for further studies that address anesthetic management of patients who are scheduled to undergo major surgery that is accompanied by severe hemodynamic changes, such as those associated with HIPEC.
In conclusion, our study demonstrated various physiological changes via the developed hemodynamic monitoring system in patients who underwent open cytoreductive abdominal surgery with HIPEC. Fluid therapy remains one of the most challenging issues for the anesthesia team. Therefore, anesthesiologists should constantly explore the most optimal intraoperative anesthetic management, including the maintenance of intravascular volume status, in major surgery that is expected to result in acute hemodynamic changes.
Supplemental Material
sj-pdf-1-imr-10.1177_0300060520983263 - Supplemental material for Physiologic and hemodynamic changes in patients undergoing open abdominal cytoreductive surgery with hyperthermic intraperitoneal chemotherapy
Supplemental material, sj-pdf-1-imr-10.1177_0300060520983263 for Physiologic and hemodynamic changes in patients undergoing open abdominal cytoreductive surgery with hyperthermic intraperitoneal chemotherapy by Myoung Hwa Kim, Young Chul Yoo, Sun Joon Bai, Kang-Young Lee, Nayeon Kim and Ki Young Lee in Journal of International Medical Research
Footnotes
Acknowledgement
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by Edwards Lifesciences, Korea.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.