
Abstract
Epilepsy is a chronic neurological disorder that is characterized by episodes of seizure. Sexual dysfunction has been reported in patients with seizure, which mostly manifests as erectile dysfunction and premature ejaculation in men. In this study, we report the case of a 65-year-old Chinese man with frequent spermatorrhea. Electroencephalography suggested local epilepsy in the left temporal lobe. After treatment with anti-epilepsy drugs, the symptoms disappeared and did not recur. To the best of our knowledge, this is the first reported case of epilepsy-induced spermatorrhea. The symptoms of spermatorrhea are probably a rare manifestation of seizure. When repetitive stereotyped symptoms occur, seizure should be considered, and tentative anti-epileptic treatment may be a good option.
Introduction
Epilepsy is a chronic neurological disorder that is characterized by episodes of seizure (of various types), and often requires lifelong management with medication. 1 Both children and adults are affected by this disease. Approximately 1 in 26 people will develop epilepsy at some point in their lives. 2 An association between epilepsy and sexual dysfunction has been noted over the last 70 years.3,4 This sexual dysfunction often manifests as altered sexual desire and dyspareunia in women, and erectile dysfunction and premature ejaculation in men.5–8 Spermatorrhea refers to the excessive emission of semen without orgasm or erection, and abnormal frequent spermatorrhea can compromise quality of life for men. 9 To the best of our knowledge, there are no previous reports of patients with epilepsy-induced spermatorrhea. Here, we present the case of an older man who presented with frequent spermatorrhea that was probably a manifestation of epilepsy.
Case presentation
A 65-year-old man was admitted to the outpatient neurology clinic with complaints of frequent spermatorrhea for 9 months, which occurred up to six times a day and led to social anxiety and a lack of energy. His past medical history presented no neurological or psychiatric disorders except for hypertension, which had existed for many years and was well-controlled by amlodipine add-on therapy. Apart from the calcium channel blocker, the patient denied the use of any other medications or alcohol and drug abuse. He was referred to a urologist 5 months after the first onset of spermatorrhea symptoms, but no specific treatment was provided. Because no improvement had been noted in his symptoms, he was referred to our clinic.
A general examination and neurological examination did not reveal any significant abnormal signs. The results of routine blood counts, liver and renal function, blood glucose, serum electrolytes, ceruloplasmin, and vitamin B12 levels were all within the normal limits. Cranial magnetic resonance imaging did not show any abnormalities (Figure 1a). Interictal electroencephalography (EEG) revealed local sharp waves and slow waves in the left temporal region, which suggested local epilepsy in the temporal lobe (Figure 1b).
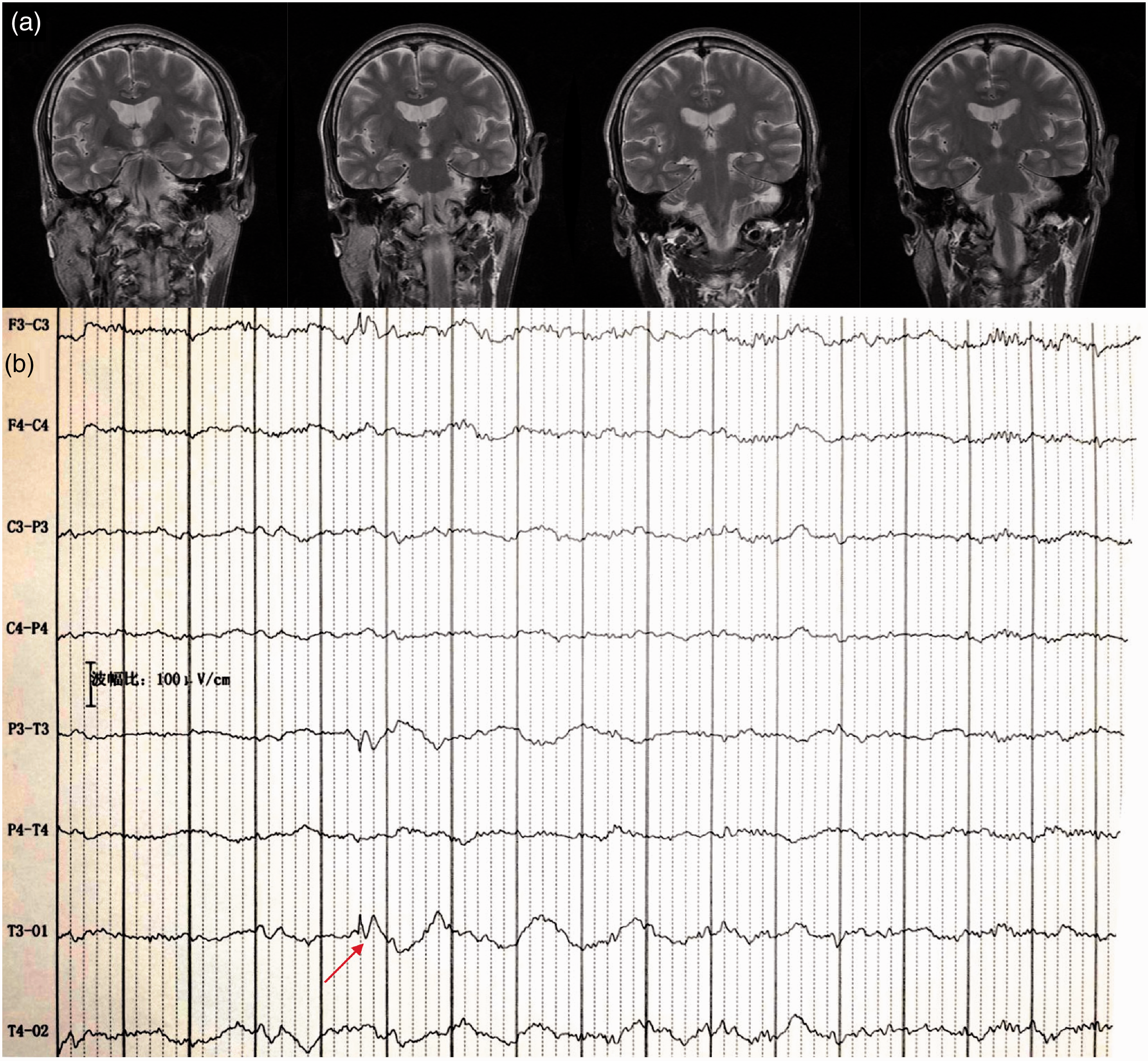
(a) Cranial magnetic resonance images of the patient with epilepsy. (b) Interictal electroencephalography showing local sharp waves and slow waves (arrows) in the leads of the left temporal zone.
Duloxetine was administered first to treat the patient’s anxiety, but this had no effect on the frequency of spermatorrhea. After EEG examination, the patient was started on levetiracetam (500 mg per day), and the symptoms of spermatorrhea declined in frequency, but still existed. After consulting with a specialist in epilepsy, we added oxcarbazepine (150 mg per day), and the symptoms disappeared completely. The symptoms of his fatigue and anxiety were also improved. The duloxetine was stopped 6 months later, and the spermatorrhea had not recurred at the follow-up, 1 year later.
Discussion and conclusions
In this report we presented a case of frequent spermatorrhea with unknown cause. Interictal EEG revealed epileptiform discharges in the left temporal region. In addition, the symptoms of spermatorrhea were reversible and could be terminated by the use of anti-epileptic drugs (AEDs). It is therefore reasonable to conclude that the frequent spermatorrhea in this patient was probably a rare manifestation of local epilepsy. To the best of our knowledge, this is the first reported case of epilepsy manifesting as spermatorrhea.
Epilepsy appears to have the potential to affect sexual function. 6 The pathogenesis of sexual dysfunction in epilepsy is likely to be multifactorial, involving neurological, endocrine, drug-related, iatrogenic, psychiatric, and psychosocial factors. 5 Some studies have demonstrated that hypothalamic and pituitary feedback mechanisms contribute to sexual dysfunction in epileptic patients. The propagation of epileptiform discharges can affect the pulsatile secretion of reproductive endocrine and dopamine via amygdalo-hypothalamic pathways.10,11 This suggests that epilepsy itself can cause hypogonadism, hyperprolactinemia, and sexual dysfunction. Furthermore, there is circumstantial evidence that sexual dysfunction can occur with the use of AEDs. Traditional AEDs (such as carbamazepine, valproate, and oxcarbazepine) can decrease free testosterone, accelerate sex hormone-binding globulin production, and stimulate the metabolism of sex hormones, which can all lead to sexual dysfunction.12–14
Epilepsy-related spermatorrhea has not been previously reported. Moreover, the literature on spermatorrhea is sparse, and the exact mechanisms of this phenomenon remain unknown. 15 Serotonin (5-HT) receptors are related to sexual function, and the binding of 5-HT to its receptors causes two distinct, stimulating and inhibitory effects on sexual function. 16 In addition, the use of selective 5-HT reuptake inhibitors (SSRIs) reportedly induced spermatorrhea in two patients with depressive disorder. 17 SSRIs increase 5-HT levels in the brain, which causes an imbalance between the two distinct functions of 5-HT receptors. 18 We therefore speculate that the epilepsy-induced spermatorrhea in our patient was related to 5-HT. It has been reported that activity within the brain during seizures causes a considerable increase in 5-HT levels. 18 This might induce a dual negative effect of aromatase inhibitors in the 5-HT system: the 5-HT levels may decrease when testosterone levels increase, and the reduced estradiol produces fewer 5-HT receptors and binding sites. 19 Unfortunately, a search of the literature failed to yield any information on the underlying mechanisms of epilepsy-induced spermatorrhea. Thus, the possible role of 5-HT in seizure-related spermatorrhea warrants further investigation.
In summary, both patients and clinicians should be aware that frequent spermatorrhea may be a rare manifestation of epilepsy. When similar symptoms occur frequently in a patient, the possibility of epilepsy should be considered, and tentative anti-epileptic treatment may be a good option. The underlying mechanisms by which epilepsy induces spermatorrhea may be associated with increasing levels of 5-HT. However, further research is needed to elucidate the exact mechanisms.
Footnotes
Acknowledgements
We gratefully acknowledge all participants for their help and willingness to participate in this study.
Author contributions
LZ designed the project. HY, DL, and HQ initiated the project. LZ, HY, DL, HQ, and YC collected and analyzed the data. LZ wrote the manuscript. YC commented and revised on the manuscript. YC supervised all aspects of the project. All authors read and approved the final manuscript.
Availability of data and materials
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available because they contain information that could compromise research participant privacy.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Ethics statement
The study was approved by the Ethics Committee for Human Research of the Second Affiliated Hospital of Zhejiang University School of Medicine (reference number: 045). Informed consent was obtained from the participant prior to his enrolment in the study.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.