
Abstract
The Bonebridge and Vibrant Soundbridge systems are semi-implanted hearing devices, which have been widely applied in patients with congenital conductive hearing loss. However, comparison between these two hearing devices is rare, especially in the same patient. We report a 23-year-old man who underwent successive implantation of Vibrant Soundbridge and Bonebridge devices in the same ear because of dysfunction of the Vibrant Soundbridge. We provide insight on the patient’s experience and compare the audiological and subjective outcomes of satisfaction.
Keywords
Introduction
Bonebridge (BB) and Vibrant Soundbridge (VSB) are semi-implanted hearing devices, which have been widely applied in patients with congenital conductive hearing loss. Because these devices have a similar appearance and surgical cost, surgeons and patients can find making an appropriate decision difficult when the patients meet the surgical indications for both devices.1,2 Because of ethical considerations, previous studies retrospectively compared both of these hearing devices in different patient groups,3,4 which may have led to individual differences, especially in evaluation of subjective satisfaction. We report here a man who underwent successive implantation of the VSB and BB in the same ear because of dysfunction of the VSB. We provide insight on the patient’s experience and compare the audiological and subjective satisfaction outcomes between the VSB and BB in this patient. Our findings can be used as a preoperative reference for surgeons and patients to make a more appropriate selection of a hearing device.
Case report
Diagnostic process and treatment
A 23-year-old man presented with bilateral malformation of the auricles and bilateral conductive hearing loss. In 1994, he was diagnosed with bilateral congenital external and middle ear malformation, bilateral atresia of the vestibular window, and congenital bilateral conductive hearing loss at Beijing Tongren Hospital at 6 years old. He then successively underwent bilateral tympanotomy, but did not achieve a satisfactory improvement in hearing after the surgery.
In 2013, when the VSB device (MED-EL Corporation, Innsbruck, Austria) was introduced into the Chinese market, he opted for a left VSB implantation (round window vibroplasty). The hearing ability of his left ear was improved after the VSB was activated (2 months after the implantation surgery). However, 2 months later, his hearing fluctuated. Subsequently, he was hospitalized for a left VSB-floating mass transducer (VSB-FMT) position revision surgery. No abnormality was found at the VSB-FMT site under a microscope. However, the VSB-FMT was engulfed by fibrous connective tissues, which may have resulted in its poor activity (Figure 1). The fibrous connective tissues were separated by the surgeon, so that the VSB-FMT could establish good contact with the round window membrane. After this procedure, the patient reported recovery of hearing. One year later, in 2016, hearing in his left ear was reduced again. Therefore, he underwent surgery for removal of the left VSB implant, as well as implantation of the BB device (MED-EL Corporation) in the ipsilateral side. During surgery, the surgeon found that the VSB-FMT was wrapped in fibrous connective tissue within the round window niche, and therefore, could not be removed. The wire of the VSB-FMT was sheared to remove the rest of the implant. A bone slot was created beneath the linea temporalis, behind the left mastoid, for implantation of a bone conductive-floating mass transducer (BC-FMT) of the BB (Figure 2). After surgery, the patient self-reported improvement in hearing with no hearing-related complaints.

During surgery for adjusting the position of the Vibrant Soundbridge, the Vibrant Soundbridge-floating mass transducer was found to be wrapped by fibrous connective tissues. The black arrow indicates the wrapped Vibrant Soundbridge-floating mass transducer.

Bonebridge implantation. The black arrow indicates the bone conductive-floating mass transducer implanted behind the left mastoid.
Assessment of audiological and subjective satisfaction
Pure tone audiology (0.25, 0.5, 1, 2, and 4 kHz) was used to test the conduction ability of air and bone of both ears before implantation of the VSB and BB to exclude the possibility of sensorineural hearing loss. Free sound field thresholds and speech discrimination scores using the Chinese Mandarin Speech Test Materials system were determined. The Hearing Device Satisfaction Scale (HDSS) was used to evaluate the patient’s subjective satisfaction after each implantation. The HDSS consists of 21 questions pertaining to the voice quality of the hearing aid devices in different situations of daily life. In the HDSS, five options were provided, and these ranged from very satisfied (100%) to no use (0), and the average value of scores was considered the final score.
Both ears are were found to have conductive hearing loss and the bone conduction hearing ability remained normal during the whole follow-up time (Figure 3). The postoperative hearing thresholds of VSB and BB implantation were improved, but the VSB performed best at the frequencies of 0.25, 1, 2, and 4 kHz (Figure 4). The speech discrimination scores of the VSB and BB are shown in Table 1. Both devices showed obvious benefits compared with the unaided condition. In the subjective satisfaction test, the total HDSS scores with the VSB and BB were 87.6 and 76.2, respectively. The patient self-reported that the effect of the VSB was better than that of the BB, taking into consideration comfort, sound quality, noise communication, clarity of voice and tones, naturalness of the sound, and specific conditions, such as listening to music or watching television (Table 2).
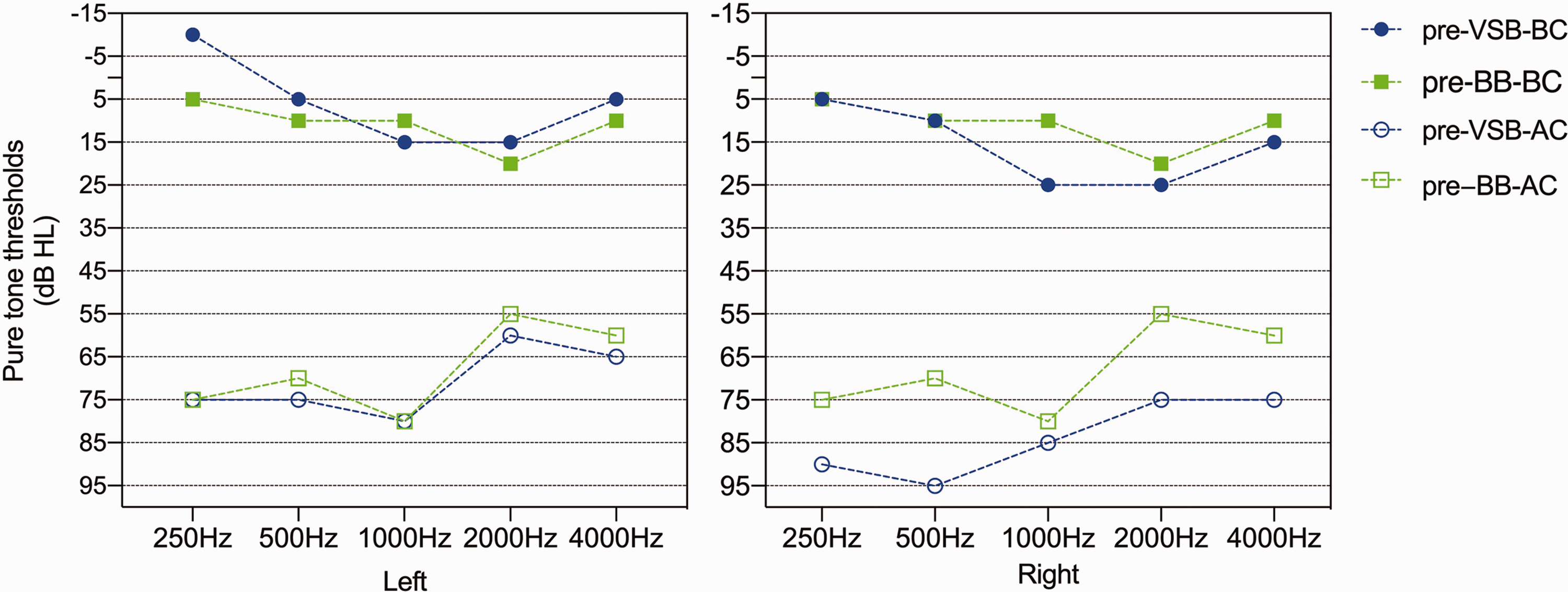
Pure tone air and bone conduction hearing threshold audiograms of both ears before each implantation surgery. The symbols show the bone conduction hearing threshold under different conditions
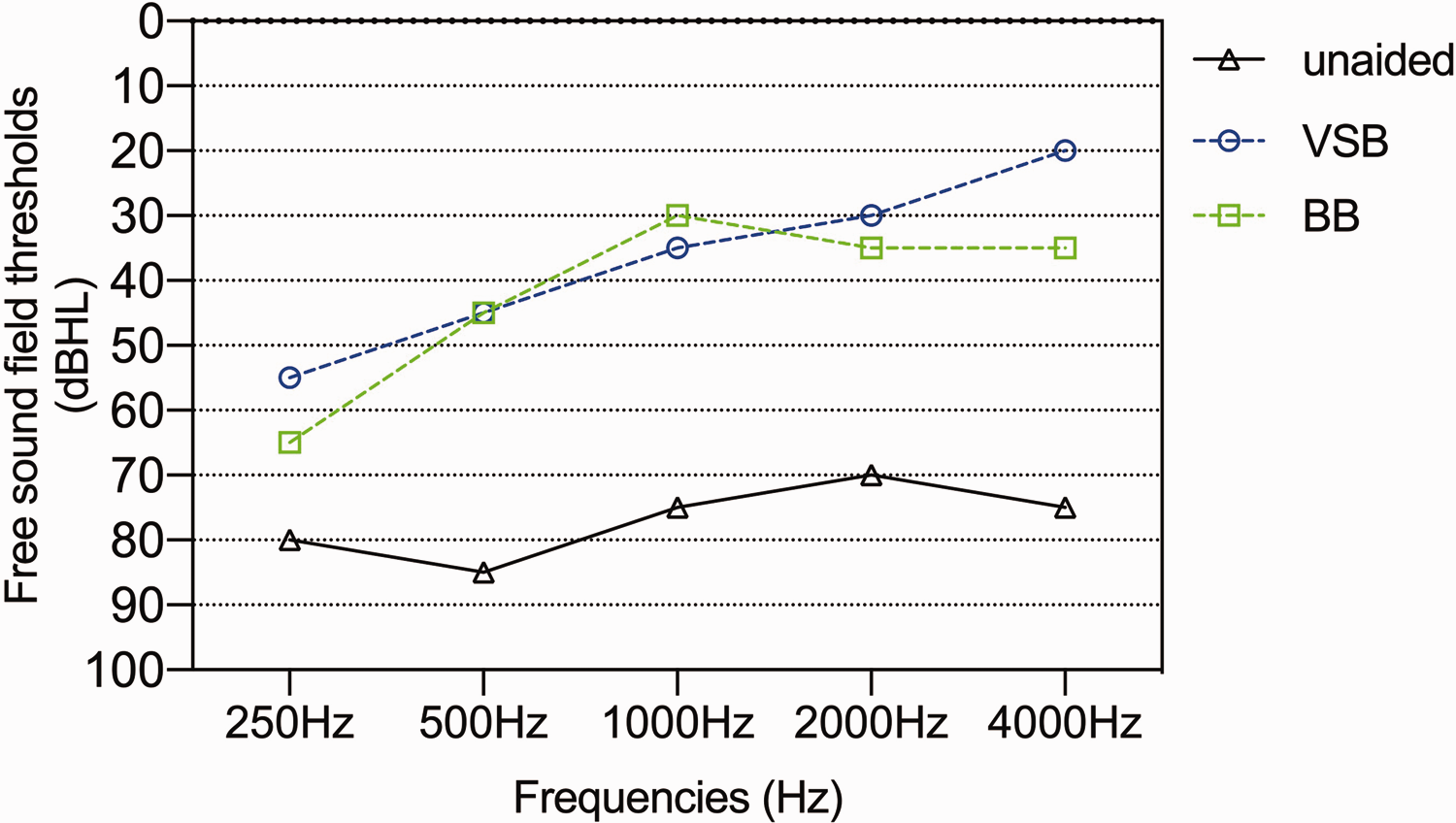
Free sound field threshold audiograms. The symbols indicate the hearing threshold under different conditions.
Speech discrimination scores of the MSTMs after implantation of the VSB and BB.

Values are shown as %.
Signal sound level: 65 dB sound pressure level.
Noise sound level: 55 dB sound pressure level.
MSTMs, Chinese Mandarin Speech Test Materials system; VSB, Vibrant Soundbridge; BB, Bonebridge.
Details of the HDSS.
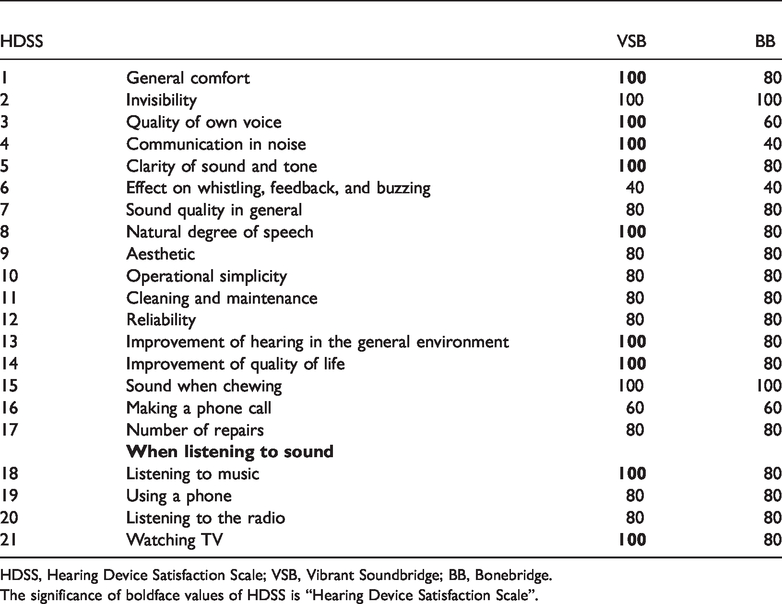
HDSS, Hearing Device Satisfaction Scale; VSB, Vibrant Soundbridge; BB, Bonebridge.The significance of boldface values of HDSS is “Hearing Device Satisfaction Scale”.
Discussion
Performing traditional surgical correction in patients with bilateral congenital external and middle ear malformation because of various complications and variable improvement in hearing remains challenging. Semi-implant hearing devices, such as the VSB and BB, provide new choices for such patients. Both of these devices are composed of external audio processors and an internal implant. The FMT is the most important part of the internal implant for the VSB and BB. As a bone conductive hearing aid, the BB audio processor can collect sound signals and transfer them into the implant by magnetoelectric induction. The BB implant can transform the sound signals into mechanical vibrations and it can be transcutaneously placed under a skin flap. As a producer of vibrations, the bone BC-FMT is fixed by two cortex screws to the mastoid and transfers vibrations into the inner ear by the bone conduction hearing pathway. The VSB is a type of middle ear implant, and the VSB-FMT can generate vibrations to stimulate the cochlea by connecting with the incus, stapes, or round window. Our patient had the VSB implanted on the round window niche and the BB implantation fixed on the skull bone cortex. The working principle of the VSB appears to be similar to normal sound transmission pathways.1,5 Therefore, the VSB may provide better quality of sound signals. Our patient’s subjective satisfaction in the HDSS is in accordance with this suggestion, and is also concordant with a survey conducted by Monini et al. 3 on subjective satisfaction of air and bone conduction hearing devices. From an audiological perspective, such results may relate to the fact that the VSB may improve the patient’s air conduction hearing, with a wider scope for enhancing sound signals in the high frequency range.
Several studies have shown the efficacy of round window implantation of the VSB.6,7 However, the mechanism of single window sound conduction remains unclear. This conduction may be caused by a third window of the cochlea, such as the cochlear aqueduct or vestibular aqueduct. 8 Furthermore, owing to the presence of an air gap between the VSB-FMT and the round window membrane, the sound wave energy returns through the round window membrane. 6
The major reason for the ineffectiveness of the VSB in our case was wrapping of the VSB-FMT by peripheral fibrous connective tissue at the round window, which demonstrated its fixation. There are two possible reasons for this finding. The first reason is that the VSB-FMT’s slight displacement caused by the connective tissue led to its disconnection with the round window membrane. Barbara et al. 9 reported two patients who had sudden hearing loss after VSB round window vibroplasty because of displacement of the VSB-FMT. These authors emphasized that the surgeon’s skill and experience played a major role in VSB round window implantation. The second reason may be that the connective tissue, which wrapped the VSB-FMT, was too thick, thus obstructing the inner ear from receiving vibration signals. This implant may be regarded by the body as foreign matter, resulting in it being wrapped and fixed by fibrous connective tissue. This complication has not been previously reported in other VSB implantation cases. However, similar pathological progress was found in metallic conductors of certain cardiac pacemakers, which were also wrapped by and adhered with fibrous tissues. 10 The mechanism of fibrous connective tissue hyperplasia has not been clarified. Cremers et al. 2 confirmed the stability of the VSB in a 3-year follow-up study of patients who were implanted with the VSB. Moreover, they suggested that, in children younger than 14 years, the implanted VSB-FMT may displace and eventually lose its function owing to changes in tympanic cavity, or displacement of the peripheral structures, such as the tympanic ring and the squamous bone. The BC-FMT has a relatively large volume (diameter of 1.58 cm, depth of 0.87 cm), and is usually placed in a bone slot that is drilled in the mastoid and fixed by cortex screws, and is surrounded by bony structures. Therefore, theoretically, the BC-FMT has limited ability to be wrapped and fixed by peripheral soft tissue compared with the VSB-FMT. No studies have reported the ineffectiveness of the BC-FMT owing to wrapping by surrounding soft tissues.
Conclusion
To the best of our knowledge, this is the first report to describe successive implantation of the VSB and BB in the same patient, particularly on the ipsilateral side. The better subjective quality of sound signals provided by the VSB may be vital when selecting a suitable device for patients who meet the indications for both devices. However, VSB implantation requires surgeons to have sufficient clinical experience and be well prepared for managing potential complications during and after the operation. We will continue to follow-up patients with semi-implant hearing devices in our research group and obtain further compelling evidence on patients’ outcomes.
Footnotes
Ethics statement
Ethical approval was provided by the medical committee of Tongren Hospital, Capital Medical University (TRECKY2018-067). Verbal informed consent for publication was obtained from the patient.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This work was supported by the Project of Capital Clinical Characteristic Application Research of Beijing Municipal Science and Technology Commission (grant number: Z171100001017079).