
Abstract
Objective
Acute pulmonary embolism (APE) is a serious complication after off-pump coronary artery bypass grafting (OPCABG). We aimed to analyze the risk factors for APE in patients with OPCABG.
Methods
In this retrospective, observational study, patients with OPCABG who were treated in our hospital from 1 January 2018 to 31 March 2020 were included. The basic characteristics of patients and results of preoperative laboratory examinations were collected and analyzed.
Results
A total of 707 patients with OPCABG were included and the incidence of APE was 3.21%. Left ventricular ejection fraction (LVEF), a history of smoking, number of bypass grafting, duration of surgery, and age were significant risk factors for APE in patients with OPCABG. The areas under the curves of LVEF, number of bypass grafting, duration of surgery, and age were 0.773, 0.759, 0.738, and 0.723, respectively. The cutoff values of LVEF, number of bypass grafting, duration of surgery, and age were 59.84, 3.18, 237.42, and 73.28, respectively.
Conclusions
LVEF, a history of smoking, number of bypass grafting, duration of surgery, and age may be risk factors for APE in patients with OPCABG. Early measures should be taken to target these risks to prevent APE.
Keywords
Background
Coronary heart disease is a common type of cardiovascular disease in the clinical setting. The pathological basis of coronary heart disease is that coronary artery lesions lead to reduced blood flow, myocardial cell ischemia, hypoxia, and metabolic disorders in the corresponding blood supply area.1,2 In the early stage, these patients may experience chest tightness, suffocation, tingling, and discomfort after being overworked or with emotional fluctuation. 3 Early diagnosis and treatment of this condition are important for the prognosis of patients. 4 Coronary artery bypass grafting (CABG) is often used to treat coronary heart disease in the surgical department. CABG can effectively relieve the symptoms of angina pectoris, improve myocardial ischemia, avoid occurrence of myocardial infarction, and improve the quality of life. 5 CABG is one of the most effective methods for treating coronary heart disease-related myocardial ischemia. 6
Off-pump coronary artery bypass grafting (OPCABG) is effective and safe. 7 Compared with pump coronary artery bypass grafting, OPCABG can avoid mechanical damage of blood cells and reperfusion injury. OPCABG may also reduce kidney damage, and reduce resistance of the systemic circulation and pulmonary circulation, and intraoperative hemodynamics are relatively stable. 8 However, OPCABG also has perioperative complications, of which acute pulmonary embolism (APE) is a serious or even fatal complication of OPCABG. 9 With continuous improvement of surgical techniques, more patients with advanced age, poor cardiac function, and other serious underlying diseases are choosing OPCABG surgery for treatment. Therefore, the incidence of APE after surgery is gradually increasing. A total of 95% of APE occurs within 1 week after surgery in patients with OPCABG. 10 The incidence of APE varies from 1.4% to 3.8%, and the mortality of APE can reach up to 38%, which seriously affects the quality of life and prognosis of patients. 11 Therefore, this study aimed to investigate the risk factors for APE in patients with OPCABG to provide insight into the prophylaxis of APE after OPCABG.
Methods
Ethics
Our study was a retrospective analysis, and it was certified and approved by the ethics committee of The Affiliated Huai’an Hospital of Xuzhou Medical University (2018012855-c). Written informed consent was obtained from all of the included patients. Furthermore, we de-identified all of the patients’ personal details during data analyses.
Patients
Patients with coronary heart disease who underwent OPCABG in the Department of Cardiothoracic Surgery from 1 January 2018 to 31 March 2020 were identified as potential candidates. The inclusion criteria were as follows: (1) diagnosis of coronary heart disease was in accordance with the related guidelines; 12 (2) the patients underwent OPCABG treatment; and (3) patients were well-informed and agreed to participate in this study. The exclusion criteria were as follows: (1) patients with severe liver and kidney injury, cardiomyopathy, lung infection, and other serious conditions; (2) patients with heart valve-related diseases; and (3) patients who disagreed to participate in the present study.
OPCABG treatment
We obtained the patients’ consent for treatment. Coronary artery bypass grafting under simple off-pump circulation was performed clinically. The operations were performed by the same group of surgeons. Before the operation, all patients stopped taking aspirin and clopidogrel, and were administered low-molecular-weight heparin calcium 60 million IU subcutaneously for 2 days. The patients continued to take oral statins, β-blockers, and angiotensin-converting enzyme inhibitor drugs whenever necessary. All patients were prohibited from smoking, drinking, and avoiding strong mood swings and strenuous exercise before surgery. All patients were routinely prepared before surgery, such as having routine blood tests, including measurement of levels of albumin, hemoglobin, blood sugar, creatinine, urea nitrogen, triiodothyronine, thyroxine, thyroid-stimulating hormone, free triiodothyronine, and free thyroxine, arterial oxygen tension, and arterial carbon dioxide tension. Imaging examinations, including computed tomography and ultrasound, were performed for all patients.
All patients underwent general anesthesia, conventional tracheal intubation, and a sternal incision, and an artificial heart–lung machine was used, but not prefilled. We freed the internal mammary artery and used a small dose of heparin (1 mg/kg) to maintain the activated whole blood clotting time for 300 s. We prepared a vascular bridge according to the conventional method. We adjusted the heart rate to approximately 60 minutes by controlling the depth of anesthesia or providing β-blockers. We then used a special sternum retractor to open the sternum and cut the pericardium longitudinally. We made two or three pericardial traction lines parallel to the left phrenic nerve, and sewed another pericardial traction line near the apex to lift the heart. A CTS stabilizer (CTS, Cupertino, CA, USA) was used to locally fix the coronary artery to be anastomosed to reduce the amplitude of the heartbeat and facilitate the operation. Under normal circumstances, left internal mammary artery–anterior descending artery anastomosis was performed first, and then anastomosis of the other target vessel was performed. We continuously monitored the patient’s electrocardiogram, blood pressure, heart rate, and oxygen saturation during the operation.
The patients were routinely returned to the cardiac intensive care unit (ICU) after surgery, and were provided comprehensive care, such as cardiosurgical special care, assisted respiration, comprehensive electrocardiographic monitoring, anti-infection, and nutritional myocardium (recombinant human brain natriuretic peptide [Xinhuosu; Xinhua Bioscience Co., Shanghai, China], 1.5 μg/kg/day; sodium creatine phosphate [Qingxi; Hengrui Co., Lianyungang, Jiangsu, China], 1 g/day). The patients were not on regular anticoagulation post-surgery. If patients experienced pain in the surgical incision postoperatively, painkillers were provided in a timely manner. If patients experienced nausea or vomiting, antiemetic and antispasmodic drugs were administered.
Diagnosis of APE
The diagnosis of APE was made in accordance with the related guidelines from the European Society of Cardiology (2019 update).13,14 All diagnoses of APE were verified by at least two senior doctors. Computed tomography pulmonary angiography was used for the diagnosis of APE with the following direct signs: there was a low-density filling defect in the pulmonary artery, which was partially or completely surrounded by the opaque blood flow (orbital sign), or it was a complete filling defect, and the distal blood vessels were not visible; or the lung field showed a wedge-shaped increased density, a banded high-density zone or discoid atelectasis, a dilated central pulmonary artery, and the distal vascular branches were decreased or disappeared.
Data collection
Two authors independently collected data on the basic characteristics of patients, including age, sex, body mass index, related complications, and a history of smoking. The results of preoperative laboratory examinations, such as albumin and hemoglobin levels, were also collected. Furthermore, details of surgery, such as the left ventricular ejection fraction (LVEF), number of bypass grafting, and duration of surgery, were evaluated and calculated.
Statistical analysis
All of the data were statistically analyzed using IBM SPSS, version 23 software (IBM Corp., Armonk, NY, USA). All continuous data are expressed as mean ± standard deviation, Comparison of binary data was conducted using the chi-square test and comparison of continuous data was performed using the t test. Furthermore, variables with statistical significance in univariate analyses were further included for logistics analyses. Logistics regression analyses were conducted to identify the relevant risk factors for APE. The receiver operating curve (ROC) was created and the area under the curve (AUC) was calculated to analyze its predictive value. A p value <0.05 was considered statistically significant.
Results
General information of the included patients
A total of 707 patients with OPCABG were included in the present study of whom 22 had an attack of APE. The incidence of APE in patients with OPCABG was 3.21%. Age was significantly older, the rates of hypertension, a history of smoking, and occurrence of concomitant deep vein thrombosis were higher, the LVEF was lower, the number of bypass grafting was higher, and the duration of surgery was longer in patients with APE than in those without APE (all p<0.05) (Table 1). There were no significant differences in sex, BMI, the rates of diabetes mellitus and hyperlipidemia, D-dimer levels, N-terminal pro-brain natriuretic peptide levels, high-sensitivity C-reactive protein levels, duration of surgery, length of ICU stay, length of hospital stay, and onset of mobilization after surgery between the two groups of patients.
Characteristics of included patients with off-pump coronary artery bypass grafting.

Data are expressed as mean ± standard deviation or n (%).
APE, acute pulmonary embolism; BMI, body mass index; LVEF, left ventricular ejection fraction; NT-proBNP, N-terminal pro-brain natriuretic peptide; hs-CRP, high-sensitivity C-reactive protein; ICU, intensive care unit.
Comparison of preoperative laboratory examination results
There were no significant differences in levels of albumin, hemoglobin, blood sugar, creatinine, urea nitrogen, triiodothyronine, thyroxine, thyroid-stimulating hormone, free triiodothyronine, and free thyroxine, arterial oxygen tension, and arterial carbon dioxide tension between the two groups (Table 2).
Patients’ preoperative laboratory examination results.
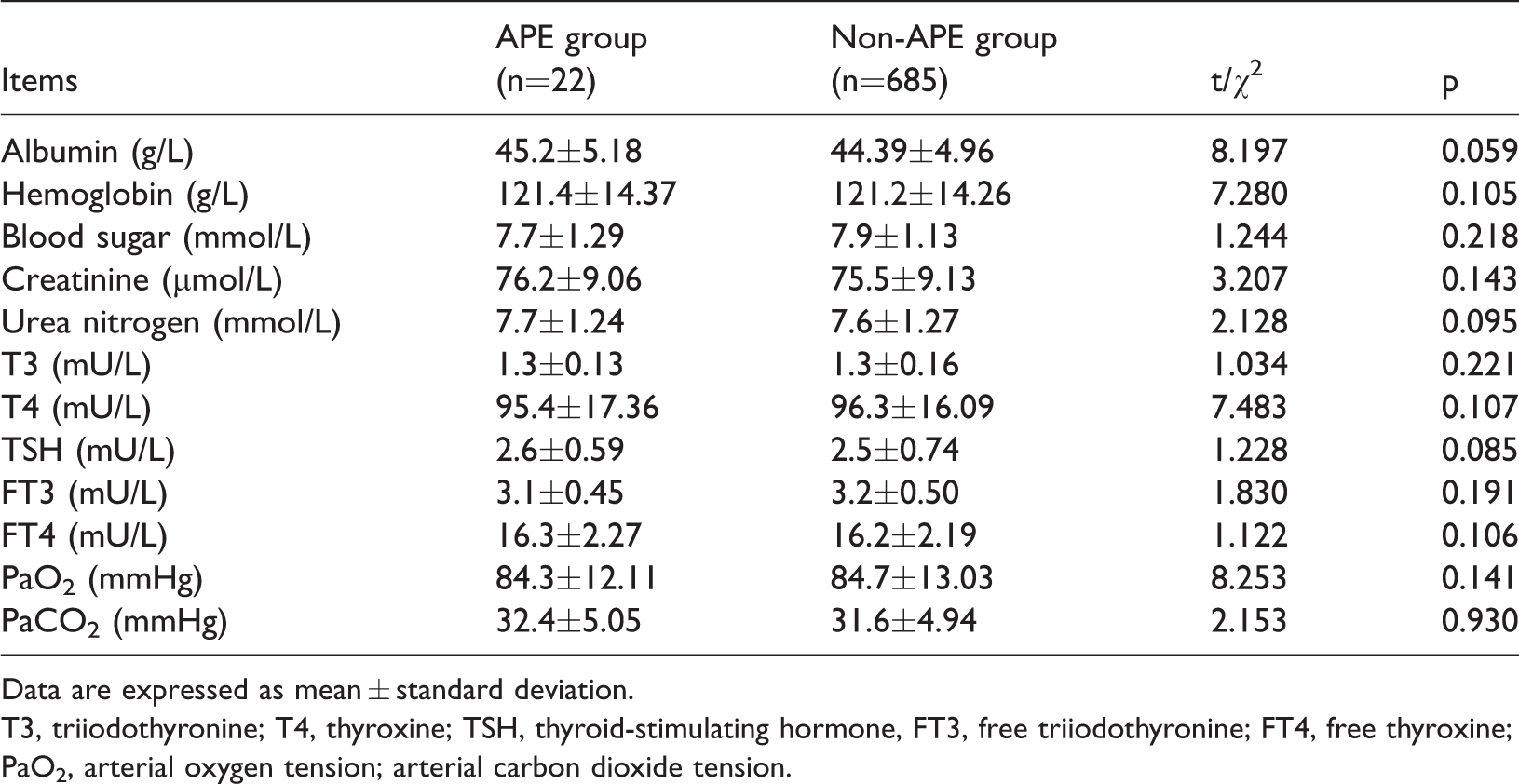
Data are expressed as mean ± standard deviation.
T3, triiodothyronine; T4, thyroxine; TSH, thyroid-stimulating hormone, FT3, free triiodothyronine; FT4, free thyroxine; PaO2, arterial oxygen tension; arterial carbon dioxide tension.
Logistic regression analysis
Logistic regression analysis showed that LVEF, a history of smoking, number of bypass grafting, duration of surgery, and age were significant risk factors for APE in patients with OPCABG (all p<0.05) (Table 3).
Logistic regression analysis on the risk factors for acute pulmonary embolism in patients with off-pump coronary artery bypass grafting.
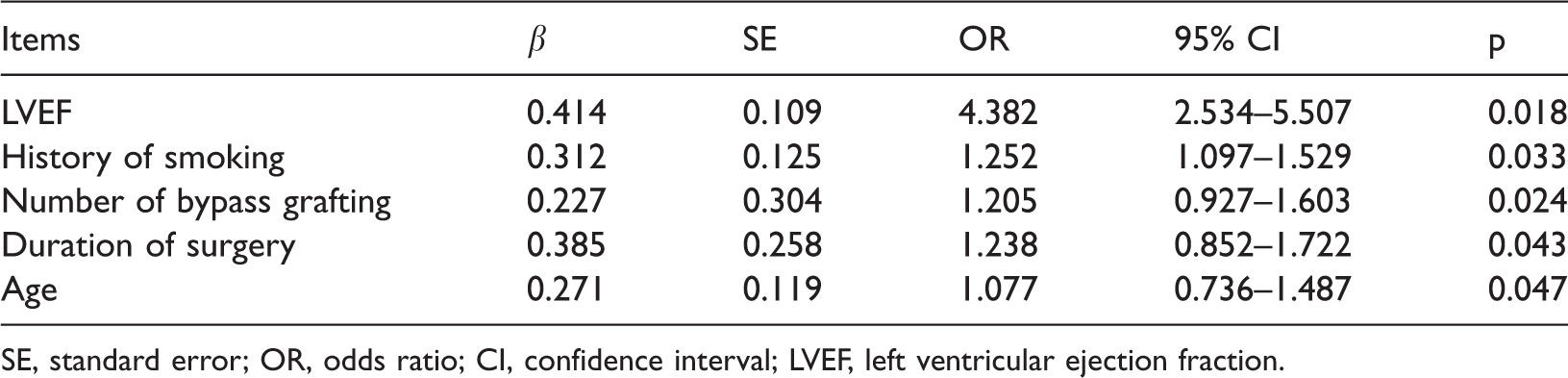
SE, standard error; OR, odds ratio; CI, confidence interval; LVEF, left ventricular ejection fraction.
ROC analysis of related factors
The AUCs of LVEF, number of bypass grafting, duration of surgery, and age were 0.773, 0.759, 0.738, and 0.723, respectively (Figure 1 and Table 4). The cutoff values indicated that patients with an LVEF ≤59.84%, number of bypass grafting ≥3.18, duration of surgery ≥237.42 minutes, and age ≥73.28 years had a higher risk for APE after OPCABG.

Receiver operating curve of relevant risk factors for acute pulmonary embolism in patients with off-pump coronary artery bypass grafting. LVEF, left ventricular ejection fraction.
Predictive value of factors related to acute pulmonary embolism.

AUC, area under the curve; CI, confidence interval; SEM, standard error of the mean; LVEF, left ventricular ejection fraction.
Discussion
Coronary heart disease, which is a common clinical disease, seriously endangers human health, and its morbidity and mortality have been increasing yearly. 15 The main treatment methods for coronary heart disease include conservative medical treatment, percutaneous coronary intervention, and surgical treatment. In patients with surgical treatment, the mid- and long-term effects of this treatment are more obvious, the probability of disease recurrence is lower, and the risk of early and long-term death is relatively reduced compared with patients with conservative medical treatment and percutaneous coronary intervention. 16 In recent years, OPCABG has been widely adopted worldwide and continues to develop and improve. OPCABG provides a wide range of ideas and options for treating coronary heart disease. 17 OPCABG effectively reduces the adverse effects of cardiopulmonary bypass on various organs and systems of the human body and related complications during and after surgery. Therefore, patients with OPCABG can avoid injury to themselves under nonphysiological conditions while undergoing surgical treatment. 18 The effect of OPCABG on the coagulation system causing hypercoagulability must be considered. APE is a serious complication in patients with OPCABG. The incidence of APE in patients with OPCABG in our study was 3.21%, which is similar to previous reports. 19 Once APE occurs after OPCABG, patient may have a faster heart rate, shortness of breath, increased cardiac work, decreased oxygen uptake, and the possibility of pulmonary infection increases. 20 Finally, APE can increase the risk of hypoxemia and pulmonary infection. If the above-mentioned symptoms and lesions cannot be improved in a timely and effective manner, they can lead to irreversible serious damage to cardiopulmonary function. Additionally, this situation can prolong the patient’s stay in the ICU and increase the financial burden, and a small number of patients with severe hypoxemia may even die. 21 Therefore, prevention and avoidance of APE after OPCABG have important practical and clinical significance for patients. The present study showed that patients with an LVEF ≤59.84%, number of bypass grafting ≥3.18, duration of surgery ≥237.42 minutes, and age ≥73.28 years had a higher risk for APE after OPCABG. Therefore, early interventions targeted for these risk factors need to be adopted to improve the prognosis of patients with OPCABG.
Our study showed that an LVEF ≤59.84% was the main risk factor for APE in patients with OPCABG. Previous studies22,23 have shown that there is a certain relationship between the degree of preoperative cardiac dysfunction and formation of venous thrombosis. In patients with insufficiency of cardiac function, the heart is often accompanied by hypertrophy. 24 For patients with preoperative cardiac insufficiency, cardiac function should be improved before surgical treatment, which may greatly reduce the incidence and mortality of postoperative APE.
People with a high incidence of coronary heart disease are relatively old, and age is closely related to disorder of the body’s coagulation function. 25 Our study showed that older patients had a higher probability of APE after surgery, which is consistent with the results of previous studies.26,27 In elderly people aged older than 70 years, the physiological reserves of various organs are reduced, such as decreased heart, liver, and lung function. 28 Elderly people are prone to disturbance of the cardiovascular system. With development of society and improvement of people’s living standards, an increasing amount of elderly patients are undergoing coronary artery bypass surgery.29,30 Special attention should be paid to patients with an older age and adequate preoperative preparations should be made to prevent the occurrence of postoperative APE.
Several previous studies31,32 have shown that smoking is closely related to atherosclerosis and thrombosis. Long-term heavy smoking can damage alveolar epithelial cells, resulting in a reduction in the amount of oxygen diffused. At the same time, this damages tracheal and bronchial epithelial cells, making them prone to bronchospasm, which ultimately leads to thrombosis. 33 Previous studies34,35 have shown that patients who smoke have more postoperative sputum, which is thick and difficult to cough up, and easily blocks the airway, compared with those who do not smoke. At the same time, the risk of lung infection is significantly increased in smokers. 36 The current study showed that smoking was an important risk factor for APE after OPCABG. Therefore, these patients should be instructed to quit smoking as early as possible to reduce postoperative APE.
Previous studies37–39 have shown that occurrence of APE is positively correlated with the operation time. Our study showed that the possibility of APE occurring increased as the operation time increased, which is consistent with related study results.37–39 A prolonged operation time increases stimulation to the body, and activates and aggregates neutrophils on the surface of the lungs through a series of inflammatory reactions. This then causes damage to endothelial factors of the lungs, leading to formation of thrombi. 40 Therefore, to effectively reduce the occurrence of APE, surgeons need to reduce the operation time as much as possible.
There are several limitations in this study. First, we did not include myocardial infarction for consideration owing to the limited collected data. Therefore, further investigation on associations of severity of myocardial infarction and APE in patients with OPCABG are required. Second, several previous studies27,41,42 showed that BMI and diabetes were risk factors for pulmonary embolism. The sample size of our study was small, and it might not have had sufficient power to detect potential related risk factors. Therefore, more studies on risk factors for APE in patients with OPCABG are required in the future. Finally, we only followed up patients for 30 days and no patients died. However, long-term follow-up on the mortality rate of these patients is required.
Conclusions
The LVEF, a history of smoking, number of bypass grafting, duration of surgery, and age may be risk factors for APE in patients with OPCABG. For patients with OPCABG, improvement of cardiac function, quitting smoking as soon as possible, and shortening the operation time during the perioperative period might have an important role in the prophylaxis of postoperative APE.