
Abstract
Objective
The performance of coronary bypass grafting (CBG) induces a type of subclinical systemic inflammatory response syndrome. The present study was performed to examine the changes in pentraxin 3 (PTX3) and oxidative parameters during cross-clamping in patients undergoing CBG. We also examined factors affecting the development of postoperative atrial fibrillation (POAF).
Method
This study involved 40 patients who underwent elective on-pump CBG (33 men, 7 women; mean age, 60.8 ± 8.0 years). Blood specimens were drawn before anaesthesia and after aortic cross-clamping. POAF was detected by analysing the rhythm records of telemetry units for 96 hours postoperatively.
Results
The mean PTX3 concentration prior to surgery was 176.3 ± 148.4 pg/mL. After cross-clamping, it increased to 947.7 ± 377.2 pg/mL. The increase was statistically significant. Twelve patients had POAF. The leucocyte count and change in the oxidative stress index were significantly higher in patients without than with POAF. Although the increase in PTX3 was higher in patients without POAF, the difference was not statistically significant.
Conclusion
The PTX3 concentration significantly increases during CBG. A significant change in the oxidative stress index and a more intense increase in the PTX3 concentration were seen in patients without POAF.
Keywords
Introduction
In patients referred for surgical myocardial revascularisation, cardiopulmonary bypass (CPB) along with cardioplegic arrest allows the surgeon to operate on a bloodless, non-beating heart. 1 However, this indisputable superiority is offset by an increase in the accompanying inflammatory response. Subclinical systemic inflammatory response syndrome is present in virtually all patients undergoing coronary bypass grafting (CBG).2,3 This response includes the activation of leucocytes, which may cross the endothelial barrier and transmigrate into the interstitial space of damaged tissue. The response is also characterised by release of proinflammatory cytokines and chemokines, expression of adhesion molecules on target organs, and activation of the complement and coagulation systems. 4 The development of systemic inflammatory response syndrome is both initiated and perpetuated by excessive production of reactive oxygen species (ROS). 5 In appropriate environmental conditions, inflammatory cells deploy their proteolytic enzymes in collaboration with highly cytotoxic ROS. 6 After aortic cross-clamping, the heart is exposed to global ischaemia. During CBG performed with the use of CPB, highly cytotoxic oxygen species are generated in post-ischaemic tissues. 7
Along with the plethora of strictly proinflammatory mediators, an almost equal number of anti-inflammatory moieties are generated during CBG operations. The best-known anti-inflammatory molecule is long pentraxin (PTX). Short PTX is a major acute-phase reactant, the prototype of which is C-reactive protein (CRP) synthesised in the liver. 8 Two forms of PTX3 are preformed and stored in specific granules of neutrophils, and they are then newly synthesised in response to appropriate stimuli and released into the extracellular space by other cells (monocytes, macrophages, dendritic cells, endothelial cells, fibroblasts, and epithelial cells). 9 Circulating neutrophils have a short half-life terminated by apoptotic death, which is necessary for host protection against any undue damage to itself. Neutrophil-derived PTX3 has a dual feedback mechanism in vivo. Whenever inflammation is evoked, delayed release of PTX3 occurs concomitantly with apoptotic death of neutrophils. However, it also restricts excess transmigration of activated neutrophils into the host’s tissues. 10
Postoperative atrial fibrillation (POAF) is the most common arrhythmia after cardiac surgery and is an important medical problem associated with an increased cost of care, mortality, and morbidity. The complexity and multifactorial nature of POAF make it impossible to identify an optimal medical treatment. Well-known conventional risk factors for AF are not consistent with those for POAF. Although clinical and experimental trials have been performed to investigate the pathogenesis of POAF, no conclusive studies have satisfactorily elucidated it. 11
The main goal of this study was to determine the changes in PTX3 and oxidative parameters in patients undergoing “on-pump” CBG. We also investigated the factors affecting development of POAF, including PTX3 and oxidative stress.
Materials and methods
This study involved patients undergoing elective on-pump CBG at the Istanbul University-Cerrahpasa Institute of Cardiology. We excluded patients with chronic inflammatory disease (rheumatoid arthritis, systemic lupus erythematosus, and similar conditions), valvular heart disease, a history of CBG or heart valve surgery, and New York Heart Association class III or IV heart failure. We also excluded patients with preoperative AF, impaired thyroid function tests, electrolyte imbalance, and a left atrial diameter of >50 mm on transthoracic echocardiography.
CRP was analysed by turbidimetry on a ROCHE/Hitachi Modular P800 system analyser (Roche Diagnostics GmbH, Mannheim, Germany). The lower limit of detection of the CRP assay was 0.2 mg/L.
We documented the changes in the PTX3 concentration during cardiac surgery. Neutrophils represent a ready-to-use reservoir of PTX3, guaranteeing that the inflammation is in the acute stage.
Blood samples were obtained from the jugular vein 30 minutes after placement of the aortic cross clamp and 10 minutes after removal of the aortic cross clamp for documentation of early release and early activity of PTX3. The blood samples were centrifuged at 3000 rpm for 10 minutes. All samples were stored at −70°C until analysis. Care was taken to ensure that the blood samples did not become lipaemic or haemolysed.
PTX3 was measured with a commercial sandwich enzyme-linked immunosorbent assay (DY1826; R&D Systems, Minneapolis, MN, USA).
The plasma total antioxidant capacity (TAC) and total oxidant status (TOS) were determined using a novel automated measurement method developed by Erel (Opera analyser, Technicon RA System; Bayer, Leverkusen, Germany). The percentage ratio of the TOS to the TAC was defined as the oxidative stress index (OSI), which is an indicator of the degree of oxidative stress. The OSI was calculated using the following formula:

POAF was detected by analysing the rhythm records of telemetry units for 96 hours after the operation. POAF was defined as an irregular rhythm without p waves and with a narrow QRS formation in the absence of a bundle branch block lasting >5 minutes on an electrocardiogram.
Echocardiographic examinations were performed according to the methods established by the American Society of Echocardiography.
SPSS for Windows, Version 15.0 (SPSS Inc., Chicago, IL, USA) was used for the statistical analysis. The results are presented as mean and standard deviation. The normality of the data distribution was checked using the Shapiro–Wilk test. Student’s t-test or the Mann–Whitney paired t-test, the Wilcoxon test, and Spearman’s correlation test were utilised when appropriate. A P-value of <0.005 was considered statistically significant.
This study was approved by the local ethics board, and all patients provided written informed consent prior to inclusion in the study.
Results
Forty patients (33 men, 7 women) were enrolled in this study. Their mean age was 60.8 ± 8.0 years, and their mean body mass index was 27.5 ± 4.4 kg/m2. Twenty-four patients were smokers, 26 had hypertension, and 17 had diabetes mellitus. The patients’ left ventricular systolic function was relatively preserved (mean ejection fraction, 52.0 ± 10.3). The average cross-clamp time was 75.2 ± 34.0 minutes, and the average number of grafts was 3.7 ± 1.1 (Table 1).
Characteristics of study population.
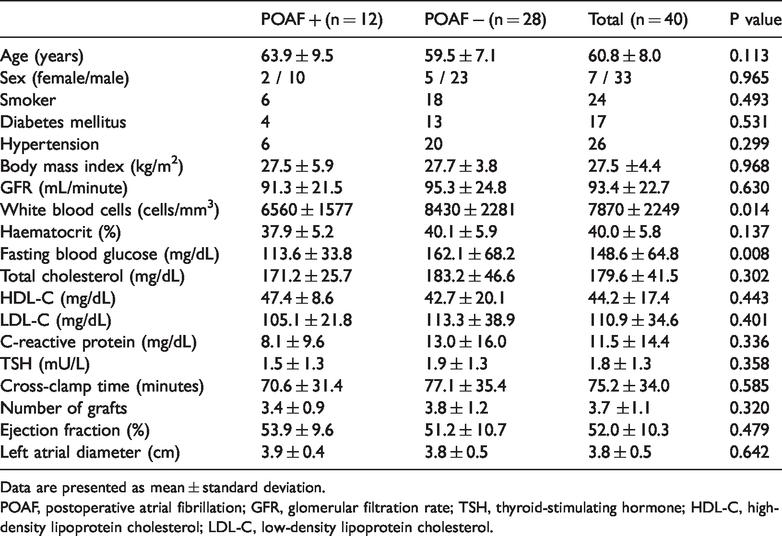
Data are presented as mean ± standard deviation.
POAF, postoperative atrial fibrillation; GFR, glomerular filtration rate; TSH, thyroid-stimulating hormone; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol.
The mean PTX3 concentration prior to surgery was 176.3 ± 148.4 pg/mL. After cross-clamping, it increased to 947.7 ± 377.2 pg/mL. This increase was statistically significant (P < 0.001) (Table 2). As expected, the TAC level did not significantly change, but the TOS level increased significantly during the operation (P = 0.002). As a result, the OSI also increased significantly (P = 0.001) (Table 2).
Comparison of pentraxin 3 and oxidative parameters in all patients.
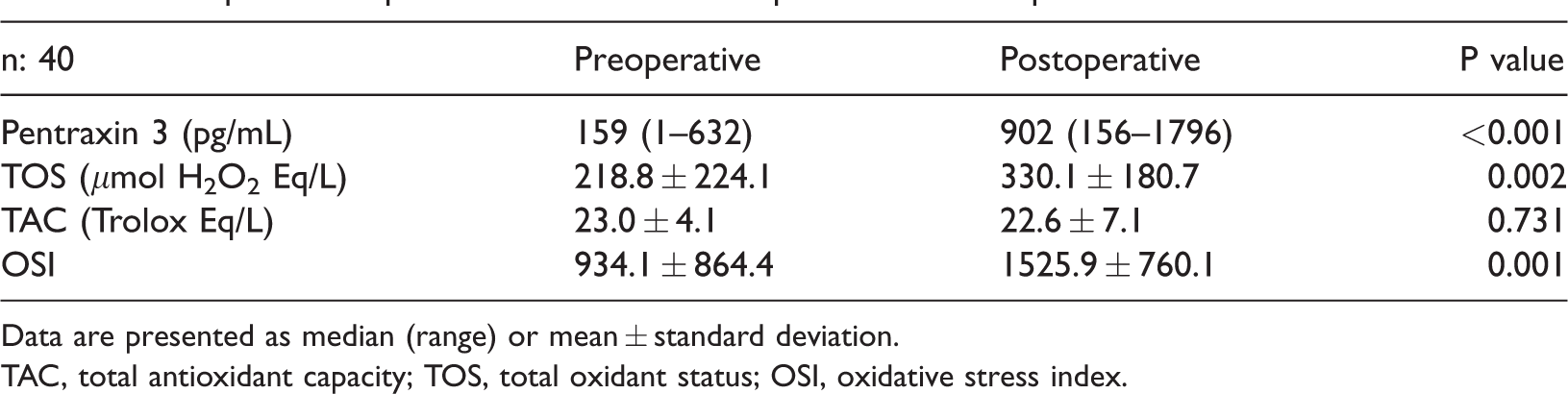
Data are presented as median (range) or mean ± standard deviation.
TAC, total antioxidant capacity; TOS, total oxidant status; OSI, oxidative stress index.
Twelve patients (30%) had POAF; 2 were female and 10 were male. Their mean age was 63.9 ± 9.5 years. Six were smokers, six had hypertension, and four had diabetes mellitus. The main clinical and echocardiographic data are shown in Table 1.
The leucocyte count, fasting blood glucose concentration, and high-density lipoprotein cholesterol (HDL-C) concentration were significantly different between patients with and without POAF (P = 0.015, P = 0.049, and P = 0.045, respectively). The PTX3 and CRP concentrations were not significantly different between the two groups (Table 1).
The correlation analysis showed a negative correlation between the HDL-C concentration and leucocyte count (P = 0.006, r = −0.430) and between the HDL-C and CRP concentrations (P = 0.02, r = −0.370). A positive correlation was found between the leucocyte count and CRP concentration (P = 0.003, r = 0.455). There were no significant correlations between other clinical, biochemical, or echocardiographic parameters.
The PTX3 concentration was 212.0 ± 165.0 pg/mL preoperatively and 881.7 ± 220.9 pg/mL postoperatively in patients with AF, and 160.7 ± 135.2 pg/mL preoperatively and 971.3 ± 420.2 pg/mL postoperatively in patients without AF. These concentrations were not significantly different between the groups (Table 3). Furthermore, the intraoperative change in the PTX3 concentration was significant in both groups (P < 0.05) (Table 4).
Comparison of oxidative parameters and pentraxin 3 concentration between groups.
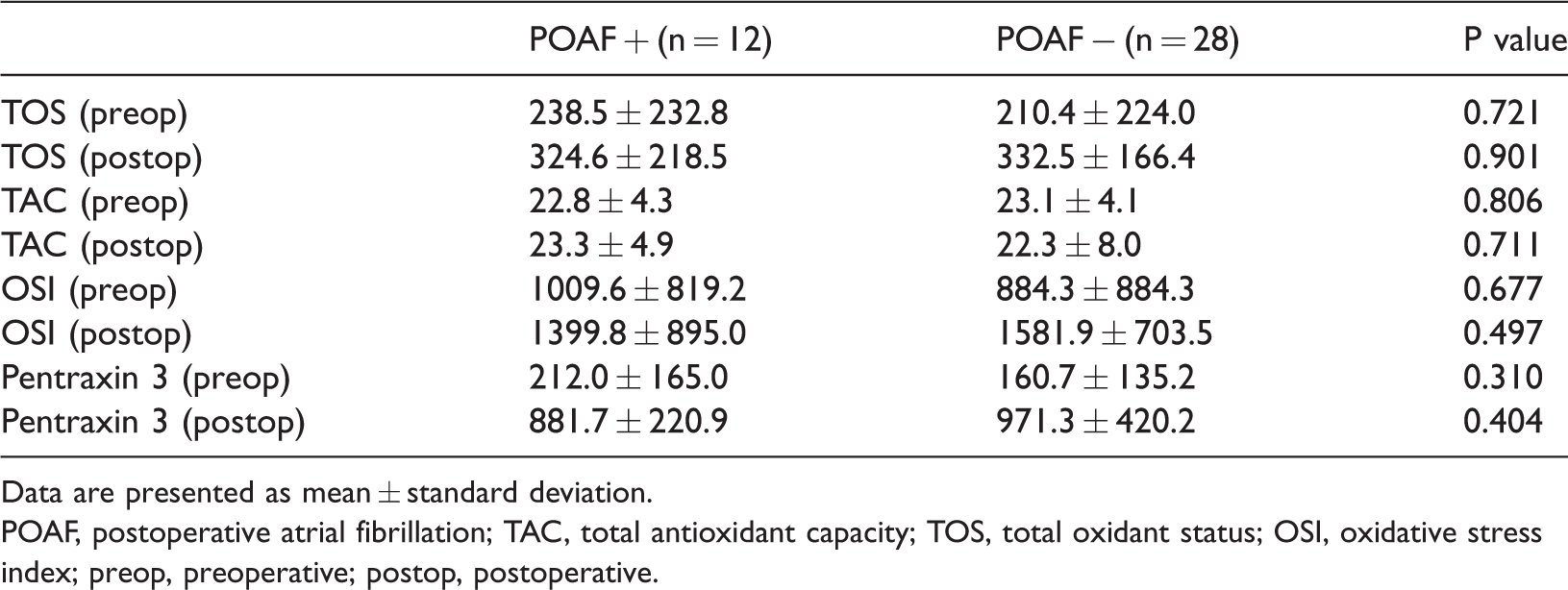
Data are presented as mean ± standard deviation.
POAF, postoperative atrial fibrillation; TAC, total antioxidant capacity; TOS, total oxidant status; OSI, oxidative stress index; preop, preoperative; postop, postoperative.
Significance of intraoperative change in oxidative parameters and pentraxin 3 concentration between groups.

POAF, postoperative atrial fibrillation; TAC, total antioxidant capacity; TOS, total oxidant status; OSI, oxidative stress index; preop, preoperative; postop, postoperative.
We found no significant difference in the TOS, TAC, or OSI preoperatively and postoperatively between patients with and without POAF (Table 3). However, patients without POAF exhibited a significant change in the TOS and OSI intraoperatively (P < 0.05). The change in the oxidative parameters was not statistically significant in patients with POAF (Table 4).
Discussion
The current study is one of few to evaluate the serum concentrations of PTX3 and oxidative stress biomarkers during cardiac bypass surgery.
Limited information is available on the acute phase response of PTX3. Peri et al. 12 showed that the PTX3 plasma concentration peaked as early as 6 hours after the onset of chest pain in patients who had presented with myocardial infarction. Kunes et al. 13 found that operations performed using a CPB pump were associated with a marked release of PTX3 immediately after the operation. In the present study, the PTX3 concentration significantly increased during the operation, which is consistent with the literature. Research has also suggested that a PTX3 concentration of >400 pg/mL has a protective role. 14 In our study, the patients’ PTX3 concentrations were >400 pg/mL postoperatively. White blood cells are a source of anti-inflammatory markers, particularly during ischaemia and reperfusion. As previously mentioned, neutrophils represent a ready-to-use reservoir of PTX3, guaranteeing its early release and early activity in acute inflammation. We thus considered that this PTX3 increase was due to the release of readymade PTX3 from neutrophils.
In the literature, the role of PTX3 is not obvious. Salio et al. 15 and Shimizu et al. 16 described the inherent cardio-protective effects of PTX3 in an animal model. PTX3 protected the ischaemic myocardium after reperfusion by attenuation of C3 deposition in mice. Clinically, PTX3 plays an active role in acute coronary syndromes 17 and stent restenosis. 18 Additional studies have shown that PTX3 is a prognostic biomarker in both acute and chronic heart failure. 19 A cardiovascular health study showed an association between PTX3 and the incidence of coronary artery disease and all-cause mortality, independent of CRP and other classical risk factors. 20 In a cohort study, the PTX3 concentration was the only independent predictor of mortality in patients with myocardial infarction. 21
HDL-C has potent anti-inflammatory activity. 22 This explains the negative correlation between the HDL-C concentration, leucocyte count, and CRP concentration in the present study.
The repeated passage of blood through the extracorporeal circuit and ischaemia–reperfusion injury during surgery can cause substantial myocardial stress, leading to the generation of inflammatory mediators and ROS. Oxidative stress occurs when uncontrolled generation of ROS overwhelms the endogenous antioxidant capabilities; this in turn impacts postoperative outcomes. Additionally, the inflammatory response that occurs during CPB is in part responsible for the increased oxidative stress during cardiac surgery. 23 In our study, the TOS was significantly increased but there was no change in the TAC. As a result, we observed a significant increase in oxidative stress during the operation. This finding is also compatible with the literature.
The incidence of POAF ranges from 10% to 40% in the literature and was 30% in the present study. The literature suggests that older age is a significant predictor of POAF. 24 Although the patients with POAF were older than those without POAF in our study, the difference was not statistically significant.
Melduni et al. 25 showed that independent predictors of POAF were older age, a higher body mass index, and an abnormal left ventricular diastolic dysfunction grade. We found no relationship among the patients’ comorbidities, preoperative and perioperative clinical results, and incidence of POAF. We also found no relationship among the ejection fraction, left atrial diameter, and cross-clamp time, which has been controversial in previous studies.26–28
The pathogenesis of POAF after cardiac surgery is believed to be multifactorial. Although the precise cellular mechanisms and pathways remain poorly resolved, enhanced inflammation, ischaemia–reperfusion, and oxidative stress are believed to play a role in the occurrence of POAF.29,30 The inflammatory response needed to augment the incidence of POAF is not presently known. We found significantly lower leucocyte counts in patients with than without POAF group. The rise in the PTX3 concentration was also lower in this group, but we found no relationship between the PTX3 concentration and POAF.
Some studies have shown that increased ROS production is independently associated with a higher risk of POAF.23,31,32 In contrast, we found more a pronounced increase in the TOS and OSI in patients without POAF.
Our study also suggests that a high leucocyte count, high OSI, and high PTX3 concentration are interdependent. Thus, a high PTX3 concentration may prevent postoperative cardiac complications.
Conclusion
CBG induces a type of subclinical systemic inflammatory response syndrome. The PTX3 concentration and the OSI rose significantly during the operation in the present study. A higher leucocyte count and a more pronounced increase in both the PTX3 concentration and OSI were observed in patients without POAF. The inflammatory response and/or oxidative stress within the atrial tissue might be critical in determining the onset of POAF. Further studies are needed to examine the role of PTX3 in CBG surgery.