
Abstract
Black hairy tongue (BHT) is characterized by a discolored, hairy tongue. We herein report two cases of BHT associated with antibacterial agents and review previous cases. In Case 1, a 17-year-old girl with a central neurocytoma was administered intravenous piperacillin–tazobactam for postoperative infection, and BHT developed 12 days later. Her symptoms resolved 8 days after she discontinued the piperacillin–tazobactam and brushed her tongue three times daily. In Case 2, a 65-year-old man was administered intravenous piperacillin–tazobactam and levofloxacin to treat multidrug-resistant Pseudomonas aeruginosa, and BHT developed 15 days later. The piperacillin–tazobactam was discontinued and the patient brushed his tongue, and the discoloration gradually subsided thereafter. However, the BHT reappeared after linezolid treatment. The patient had adverse drug reactions to both the piperacillin–tazobactam and linezolid treatments. The BHT might have been related to antibiotic use in both cases. We identified 19 cases of antibiotic-related BHT in a literature search, but none were related to piperacillin–tazobactam use. In all cases, symptoms resolved after discontinuation of the drug and brushing of the tongue. BHT may be a rare adverse effect of antibiotics. Treatment strategies include removal of the causative agents, mechanical debridement, and good oral hygiene.
Keywords
Introduction
Black hairy tongue (BHT) is an unusual condition characterized by discoloration, elongation, and hypertrophied filiform papillae on the dorsal surface of the tongue. 1 Hairy tongue commonly appears black or brown; however, yellow, green, and blue appearances have also been reported. 2 BHT is usually asymptomatic, but some patients experience halitosis, tickling, or burning of the tongue. 3 Antipsychotics, methyldopa, lansoprazole, interferon, antidepressants, antineoplastics, and antibiotics (e.g., cephalosporins, penicillins, tetracyclines, clarithromycin, and linezolid) have been reported to cause BHT. 3 , 4 We herein report two cases of BHT after treatment with anti-infective agents. Using the Naranjo adverse drug reaction causality scale, 5 we evaluated the association between BHT and antibiotics. To the best of our knowledge, these are the first two cases of BHT associated with piperacillin–tazobactam.
Case reports
Case 1
A 17-year-old girl presented with decreased vision in both eyes. She was diagnosed with a central neurocytoma. She had been healthy in the past and had no inherited diseases. The patient underwent excision of the intracranial space-occupying lesion and lumbar cistern catheterization. She was given ceftriaxone, omeprazole, dexmedetomidine, and potassium chloride for a couple of days perioperatively. Eleven days after the operation, the patient presented with remittent fever. A cerebrospinal fluid (CSF) analysis revealed a white blood cell (WBC) count of 12 × 106/L and a protein levels of 1330.85 mg/L. The CSF sample was cultured on Columbia agar with 5% sheep blood at 35°C. Intravenous (IV) vancomycin (1 g, every 8 hours) and meropenem (1 g, every 8 hours) were administered as empirical antibiotics on 23 November. Fifteen days after the operation, a CSF culture showed Staphylococcus capitis. Meropenem was stopped and sulfamethoxazole–trimethoprim was added according to the antimicrobial susceptibility results on 27 November. Two days later, the patient was febrile again (maximum body temperature of 39°C) with an elevated WBC count (12.82 × 109/L). Piperacillin–tazobactam (4.5 g, every 6 hours, IV) was introduced on 29 November. The patient’s temperature dropped and her WBC count returned to normal 1 day after initiation of the new therapy. Twelve days after initiation of the new antimicrobial therapy, the patient’s mother reported blackish pigmentation on the surface of the patient’s tongue (Figure 1(a)). Examination of her oral cavity revealed brown-to-black discoloration with a hairy coating on the posterior aspect of the dorsal surface of the tongue. The patient was diagnosed with BHT. Bifidobacterium was prescribed as a probiotic to regulate the flora based on suspicion of a secondary infection caused by piperacillin–tazobactam treatment. No culture of the BHT was performed. The piperacillin–tazobactam was discontinued, and the patient was asked to clean her tongue with a soft-bristle toothbrush three times a day. The patient also gargled after eating. Most of the hairy coating subsided after 2 days (Figure 1(b)). Total disappearance of the lesion was observed 8 days later. Using the Naranjo adverse drug reaction causality scale to evaluate the association between the drugs and BHT, the score for piperacillin–tazobactam was 5, which was higher than that for other drugs used by the patient.

Case 1. (a) Black hairy tongue in a 17-year-old girl receiving piperacillin–tazobactam. (b) Image of the patient’s tongue 2 days after stopping piperacillin–tazobactam and brushing the tongue.
Case 2
A 65-year-old man presented with a 24-year history of hypertension. His blood pressure was well controlled with enalapril. He had undergone surgical treatment of lung cancer 3 months prior. After 5 days of chemotherapy, he developed a fever. A peripheral blood test revealed a very low WBC count (0.62 × 109/L) and platelet count (63 × 109/L), indicating myelosuppression. To avoid gingival bleeding, the patient was asked not to brush his teeth. He was prescribed mouthwash containing silver ions, which he used three times a day to maintain oral hygiene. He had a 47-year smoking history and had not used cigarettes for about 2 years. He had 17 artificial teeth, which were removed and cleaned every night before sleep. He was administered tropisetron, granulocyte colony-stimulating factor, compound vitamins, and compound amino acids within the first week after admission. Fourteen days after admission, a sputum culture revealed multidrug-resistant Pseudomonas aeruginosa. Piperacillin–tazobactam (4.5 g, every 6 hours, IV) and levofloxacin (750 mg, once daily, IV) were started on 26 November. The patient became afebrile after 6 days, and repeated sputum cultures turned negative. The levofloxacin was discontinued on 7 December. After 5 days, the patient reported a brown-to-black discoloration of the tongue (Figure 2(a)). The patient was diagnosed with BHT. A scraping of the tongue was cultured, and no bacteria or yeast were found. The BHT was suspected to be secondary to treatment with piperacillin–tazobactam. The piperacillin–tazobactam and mouthwash were discontinued. The patient was advised to brush his tongue three times a day. The discoloration of his tongue gradually subsided. The Naranjo score for piperacillin–tazobactam was 3, which was higher than that for other drugs taken by the patient.
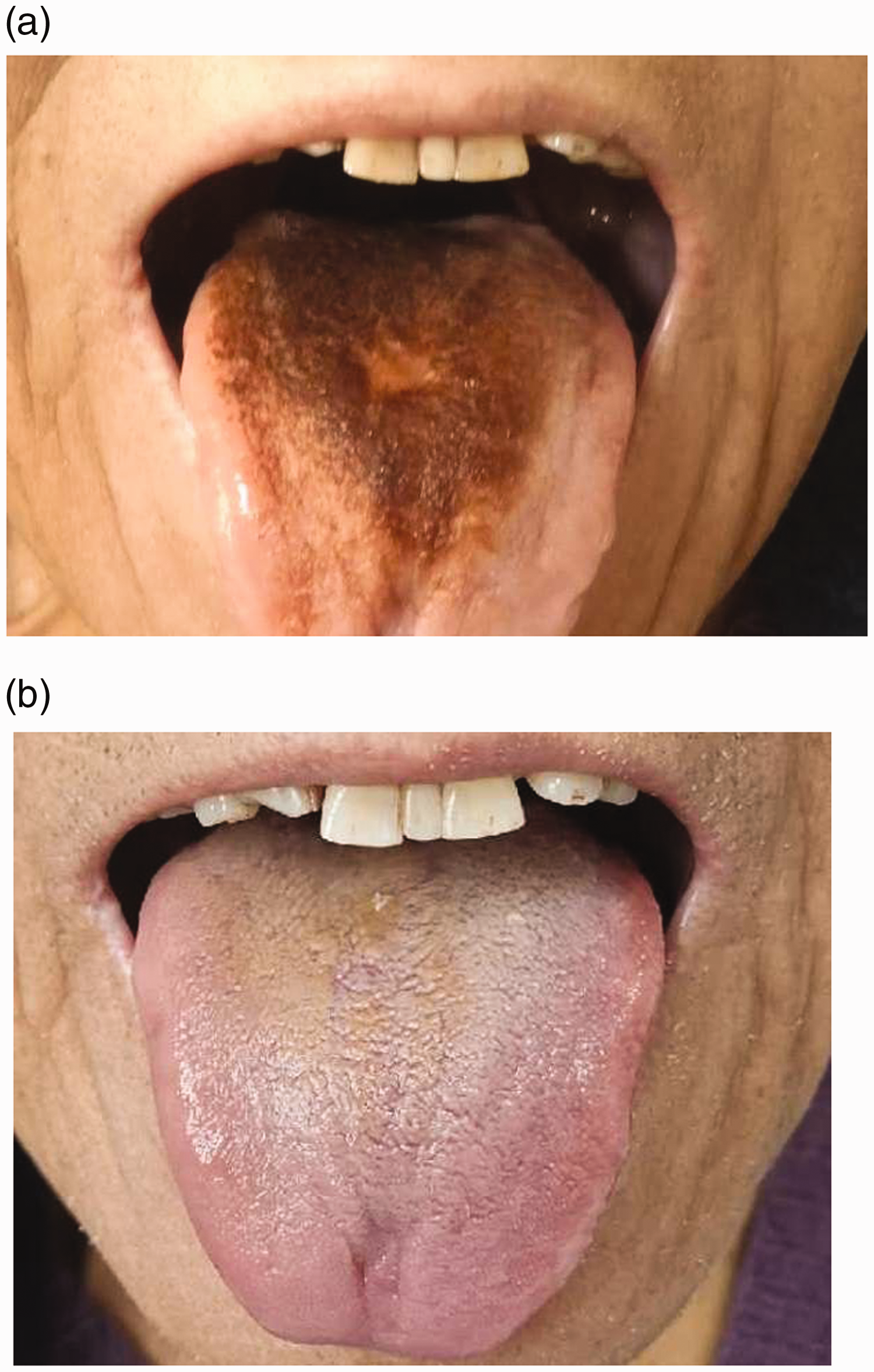
Case 2. (a) Black hairy tongue in a 65-year-old man receiving piperacillin–tazobactam. (b) Image of the patient’s tongue 13 days after discontinuing treatment on 25 December.
Outcome and follow-up
On 19 December, the patient in Case 2 developed a fever again. Piperacillin–tazobactam (4.5 g, every 6 hours, IV) and linezolid (600 mg, every 12 hours, IV) were started again. Six days later, the piperacillin–tazobactam was discontinued. The tongue still exhibited brown discoloration (Figure 2(b)). Intravenous linezolid was administered for another 10 days. The BHT had not completely resolved when the patient was discharged from the hospital on 7 January.
The patient was prescribed linezolid tablets (600 mg, every 12 hours) for 1 month after leaving the hospital. The BHT recurred after he had been taking linezolid for about 7 days; however, he completed the 1-month course of linezolid. During this month, the tongue discoloration persisted despite brushing his tongue and teeth three times a day. BHT associated with linezolid was suspected, and the Naranjo score was 7 (Table 1). The BHT eventually resolved nearly 10 days after discontinuation of linezolid.
Naranjo adverse drug reaction causality scale scores.

P, piperacillin–tazobactam; L, linezolid; ADR, adverse drug reaction.
Source: Reference 5.
The patient had an adverse drug reaction to both the piperacillin–tazobactam and linezolid treatments; the Naranjo scores were 3 and 7, respectively.
Patients’ perspectives
In Case 1, the patient’s mother felt that the treatment was very effective with low cost. In Case 2, the patient and his companion were confused about why the abnormal appearance of the tongue persisted, and they sought other solutions. They felt anxious until they were informed that BHT is a benign condition with a good prognosis. Both patients considered the treatment to be simple, practicable, and painless.
Literature review
A search of the online databases PubMed, Embase, and Web of Science as well as the reference lists of all retrieved articles was performed for articles published from 2000 to 2019. The search terms were “black hairy tongue,” “lingua villosa nigra,” “hairy tongue,” “antibiotic,” “side effect,” and “adverse drug reaction.” Reports in which BHT was associated with antimicrobials were collected. The full-text articles, if available, were retrieved. Non-English articles for which we could not acquire a translation were excluded from the literature review. In total, 16 articles describing 19 cases of antibiotic-induced BHT were found during the literature search. The clinical characteristics of all patients are listed in Table 2. The related antimicrobial agents were linezolid (n = 10), amoxicillin–clavulanate (n = 4), erythromycin (n = 1), doxycycline (n = 1), minocycline (n = 2), and metronidazole (n = 1). Of the 19 patients, 13 (68.4%) were male and 6 (31.6%) were female. The patients’ ages ranged from 7 to 80 years. Six patients had other possible risk factors for BHT, such as smoking, edentulism, and poor oral hygiene. The Naranjo probability scale was applied in 13 reports. Microbiologic culture of the tongue or a throat swab revealed fungi in three patients, two of whom were prescribed antifungal agents. In one case, the Naranjo score was 10, indicating a definite drug association. The mean time to the occurrence of linezolid-associated BHT was about 2 weeks. Most patients discontinued the suspected drug, and the BHT resolved in all of them with cleaning of the tongue and application of good oral hygiene.
Summary of cases of antibiotic-associated black hairy tongue from the literature and two cases at our institution

M, male; F, female; NR, not reported; ND, not detected; SMZ-TMP, sulfamethoxazole–trimethoprim
Discussion
The first case of BHT was documented in 1557 by Dr. Amatus Lusitanus, who described the condition as self-renewing of the tongue. 1 Since then, several cases have been described in the literature.
We have herein presented two cases of BHT in Chinese patients. In Case 1, recovery was observed 8 days after treatment. In Case 2, the brown discoloration persisted throughout the hospitalization period. Persistent discoloration may be related to the reuse of piperacillin–tazobactam before the problem is completely resolved. Notably, the linezolid-associated BHT recurred after the patient had been discharged from the hospital for about 1 week. The presence of linezolid-induced BHT was supported by the Naranjo score of 7. The duration of linezolid-related BHT was about 3 weeks, which was slightly longer than the durations in previous reports.
Limitations
Our study had two main limitations. First, because patients may not closely monitor their appearance while hospitalized, the reported onset of symptoms may be inaccurate. Second, the inpatient in Case 2 was in a fragile state, and a large amount of information was reported by his companion. Some details may have been omitted, affecting our assessment.
Etiology
Many substances and conditions aggravate, precipitate, and even cause BHT. First, several medications are associated with the development of BHT. The association of BHT with antibiotics such as erythromycin, doxycycline, linezolid, penicillin, minocycline, and metronidazole is well documented in the literature. 3 Antipsychotic medications capable of causing xerostomia and some chemotherapeutic agents are linked to BHT. 1 Second, various behavioral factors, such as smoking or chewing tobacco, excessive coffee consumption, alcohol consumption, heavy black tea consumption, and poor oral hygiene, increase the risk of BHT. 3 Third, immunocompromised states, human immunodeficiency virus infection, advanced cancer, and recent radiation therapy to the head and neck region are also associated with an increased rate of BHT. 1 Fourth, certain conditions are thought to limit the normal desquamation of the keratinized filiform papillae, leading to hyperkeratosis. For example, patients with trigeminal neuralgia may experience pain during mastication. 22 Pureed or soft diets with less roughage, such as those ingested by edentulous patients, are less likely to desquamate the dorsal tongue and may therefore lead to keratin retention. 23 Fifth, xerostomia alone is probably capable of causing BHT when combined with other predisposing factors. 24 Finally, there is evidence for a relationship between excessive use of oxidizing mouthwashes and BHT. 25
Clinical diagnosis
No objective diagnostic criteria have yet been established for BHT. The diagnosis of BHT depends on visual inspection of discolored, elongated, and hypertrophied filiform papillae. BHT should be differentiated from black tongue without elongated filiform papillae. A detailed history may be necessary to determine the contribution of a drug or other substance. Dermoscopy can be used as a diagnostic tool in BHT by enabling the precise detection of changes in the shape and color of filiform papillae. 26 Biopsy is not necessary unless the lesion is atypical, symptomatic, or suspected to be a malignancy or systemic disease. The patients described in this article were diagnosed with BHT without a dermoscopic examination or biopsy.
Pathophysiology
BHT may result from both environmental and intrinsic factors. BHT consists of two components: discoloration of the tongue and elongated filiform papillae. The elongated papillae can reach 12 to 18 mm in length and 2 mm in width. 8 The most common coloration of the tongue is black or brown, but the tongue can also be green, yellow or blue. Based on the current study and case reports of antibiotic-induced BHT, four hypotheses for the pathogenesis of BHT can be considered. First, hair-like projections are thought to develop from delayed, inadequate desquamation of keratin over the filiform papillae. This may be caused by a lack of tongue movement and friction. Antimicrobial use may alter the usual flora of the mouth, and chromogenic bacterial growth may discolor the tongue. Porphyromonas gingivalis, a gram-negative anaerobic rod bacteria, produces porphyrin, which can discolor the tongue. 27 Second, antimicrobials can discolor the tongue, and inadequate desquamation can lead to a hairy appearance. Linezolid reportedly has an adverse effect of tooth discoloration. 26 Minocycline can also discolor the tongue or the thyroid. 29 , 30 Third, long-term antimicrobial use may lead to a secondary fungal infection of the tongue. In our review, a fungal culture was performed for seven patients. Candida species or Saccharomyces cerevisiae was found in throat or tongue swab cultures of three patients. No culture was performed for the patient in Case 1 of our study. In Case 2, a culture was performed but no bacteria or yeast were found. Fourth, the urinary nicotinamide output decreases substantially during oral penicillin therapy, 31 suggesting that penicillin inhibits the growth of intestinal organisms involved in the synthesis of nicotinamide.
Management
BHT is a benign, asymptomatic, and self-limiting disease with a good prognosis. Identifying the at-risk population and performing appropriate interventions can reduce the development of BHT. Patients receiving medications associated with BHT should be educated on preventive techniques. The risk of BHT may be reduced by practicing good oral hygiene. After diagnosis, a thorough medical and medication history is needed to establish the causative relationship. In our review, most patients discontinued use of the suspected drug, and the BHT was resolved in all patients by cleaning the tongue and applying good oral hygiene. Accordingly, first-line treatments include discontinuation of the offending drug and modification of predisposing habits, such as the cessation of oxidizing mouthwashes and smoking, good oral hygiene, and gentle debridement with a soft toothbrush.
Because antibiotic-related BHT is rare, clinicians who encounter it for the first time may attribute the abnormality of the tongue to a secondary infection after a period of antibiotic use. Antifungal agents and/or probiotics may be prescribed as empirical therapies. However, in our review of 19 cases, only Ramsakal and Mangat 7 and Sheikh et al. 10 confirmed the presence of Candida species. Whether the microbiological finding of fungi represents an infection or colonization remains unclear. Therefore, antifungal treatment as first-line therapy is not recommended. There are also many anecdotal reports demonstrating the use of other products to treat BHT, such as topical 50% trichloroacetic acid, topical 40% urea solution, vitamin B complex, gentian violet, and thymol. 24 Our review and two newly reported cases clearly indicate that BHT is reversible and unlikely to be harmful; accordingly, the causative drug can be reintroduced if necessary.
Conclusion
BHT is a benign, self-limiting disease with a good prognosis. Current treatment is focused on mechanical debridement, good oral hygiene, and the removal of potential causative agents. Antifungal treatment is usually unnecessary.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Ethics approval and consent to participate
This study was approved by the Ethics Committee of The Second Affiliated Hospital of Air Force Medical University, Shaanxi, China. Written informed consent was obtained from the next-of-kin of both patients for the publication of the case reports and accompanying images.
Funding
This work was supported by the Shaanxi Province Youth Science and Technology New Star Plan (2018KJXX-089).