
Abstract
Objective
This study was performed to identify the risk factors for carotid atherosclerotic plaque formation using B-Flow ultrasound.
Methods
In total, 120 patients who underwent bilateral carotid ultrasound examination were enrolled in this cross-sectional study. The intima–media thickness was measured, and the risk factors for carotid atheromatous plaque formation were investigated.
Results
Age, sex, medical history of hypertension, coronary heart disease, and diabetes were risk factors for carotid atheromatous plaque formation. Multivariate logistic regression analysis revealed that the main risk factors for carotid atheromatous plaque formation were male sex, advanced age, a high hemoglobin concentration, a high red cell distribution width, and a high low-density lipoprotein cholesterol concentration.
Conclusion
The risk factors for carotid atheromatous plaque formation were basically the same as those for stroke. Early ultrasound examination of the carotid artery enables the identification of risk factors associated with stroke.
Keywords
Introduction
Atherosclerotic plaque formation is a risk factor for cerebral infarction and coronary heart disease. The degree of carotid stenosis is positively correlated with the risk of stroke. 1 Rupture of unstable atherosclerotic plaques is the main cause of cerebral infarction and is a risk factor for early progression of cerebral infarction. 2 Stroke is currently the leading cause of death in China. Compared with Western countries, the incidence and mortality of stroke in China are higher than those of acute myocardial infarction. 3 Stroke is usually present in combination with cerebrovascular disease and thrombosis, which cause damage to target organs. 4 An age of >65 years has been identified as a major risk factor for stroke. 5 The prevention and treatment of carotid atherosclerosis should be especially focused on elderly patients. Therefore, evaluation of carotid atherosclerosis in elderly patients is important for the prevention and detection of ischemic cerebral stroke.
B-Flow ultrasonography is a highly sensitive detection method that can repeatedly measure the intima–media thickness (IMT) of the carotid artery. 6 An increased carotid IMT and plaque formation are reliable indicators of vascular outcomes. 7 In this study, we evaluated the properties of carotid plaques in elderly patients and identified risk factors for carotid atherosclerotic plaque formation by examining the bilateral carotid arteries using B-Flow ultrasonography.
Materials and methods
This cross-sectional study was approved by the Ethics Committee of Sir Run Run Shaw Hospital, College of Medicine and was performed in accordance with the declaration of Helsinki. Written informed consent was obtained from all participants.
General information
Patients who were admitted to our hospital and underwent carotid artery examination from July 2012 to May 2014 were enrolled in this study. All diagnoses were based on the standard guidance of ischemic stroke screening and prevention. A local IMT of >1.5 mm was set as the diagnostic basis for carotid plaque formation. The exclusion criteria were the presence of circulatory system diseases, lack of patient cooperation or inability to tolerate the examinations, long-term use of drugs that can affect blood coagulation functions, and a history of neck surgery.
Ultrasound examination method
We used a GE VIVID 7 color Doppler ultrasound machine equipped with a B-Flow function and 5- to 10-Hz broadband linear array probes (GE Healthcare, Chicago, IL, USA). Under quiet conditions, the patients were maintained in the supine position with a pillow placed beneath the neck, the head laid back, and the neck fully exposed. The following procedure was then carried out. (1) Using the gray-scale imaging method and B-Flow ultrasonic technology, the transverse section was scanned first, followed by the longitudinal section. On the right side, the scan was performed from the bifurcation of the innominate artery; on the left side, the scan was performed from the aortic arch to continuously observe the common carotid artery (proximal, middle, and distal segments), external carotid artery trunk and branches, internal carotid artery bifurcation, and internal carotid artery (proximal, middle, and distal segments). (2) The three-layer structure of the vessel wall in the proximal end of the common carotid artery, carotid body, and internal carotid artery (including the adventitia, media, and intima) was observed, and the IMT was measured. (3) Longitudinal sections were set within the internal and external carotid artery, respectively, with an up-and-down range of 1.0 to 1.5 cm. The diameters of the distal end (below the bifurcation) and body (at the bifurcation) of the common carotid artery, the diameter of the proximal end (above the bifurcation) of the internal carotid artery, and the arterial IMT were measured. The presence of atherosclerotic plaque was observed.
Clinical detection
A systematic physical examination of all patients was performed. Each patient’s medical history was recorded with respect to hypertension, coronary heart disease, diabetes, hyperlipidemia, and cerebrovascular disease. The fasting blood glucose concentration, red cell distribution width, hemoglobin concentration, triglyceride concentration, and low-density lipoprotein (LDL) cholesterol concentration were determined within 24 hours before the ultrasound examination using the ADVIA 2400 Clinical Chemistry System (Siemens, Munich, Germany) and the Hematology Analyzer XE-2100D (Sysmex, Shanghai, China).
Statistical analysis
Statistical analysis was conducted using SPSS for Windows, version 15.0 (SPSS Inc., Chicago, IL, USA). Count data were compared using a variance test. Measurement data are expressed as mean ± standard deviation and were compared using a t-test. Univariate logistic regression analysis was used to determine the correlation between two variables. The risk factors were analyzed using multivariate non-conditioned logistic regression analysis. A P value of <0.05 was considered statistically significant.
Results
General information of patients
In total, 120 patients (75 men, 45 women) were included in this study. The patients’ mean age was 72.72 ± 9.23 years. Sixteen patients had diabetes mellitus, 34 had hypertension, and 4 had both hypertension and diabetes mellitus. Among the 120 patients, 240 carotid arteries were examined. According to the conditions of bilateral carotid plaque formation and using a local IMT of >1.5 mm as the diagnostic basis of carotid plaque formation, 87 of the 120 patients were determined to have carotid atheromatous plaques in one or both sides of the carotid artery. These patients were assigned to the plaque group. The remaining 33 patients had no plaque on either side of the carotid artery and were assigned to the control group. The demographic information of the patients in both groups is summarized in Supplemental Table 1. The number of patients aged ≥70 years was significantly higher in the plaque group than in the control group (P < 0.05). The number of patients with diabetes was also significantly higher in the plaque group than in the control group (P < 0.05). There was no significant difference in sex, history of hypertension, or coronary heart disease between the two groups.
Multifactor analysis of risk factors for carotid atherosclerotic plaque formation
The correlations between routine blood indexes and carotid plaque formation were analyzed and compared between the two groups (Table 1). The properties of the carotid plaques were used as dependent variables, while routine blood indexes were used as independent variables. Using one-factor logistic regression analysis, the correlations between related routine blood indexes and the properties of the carotid plaques were evaluated. The correlations between related blood biochemical indexes and carotid plaque formation were also analyzed and compared between the two groups (Table 2). The presence of carotid plaques was used as the dependent variable, while age, hypertension, diabetes, and other basic diseases and routine blood indexes were used as independent variables. The following independent variables were screened using one-factor analysis: sex X1, age X2, hypertension X3, glucose concentration X4, total cholesterol concentration X5, high-density lipoprotein cholesterol concentration X6, LDL cholesterol concentration X7, free fatty acid concentration X8, and high-sensitivity C-reactive protein concentration X9. Multifactor logistic regression analysis was used to evaluate the correlation between the above-mentioned independent variables and unstable carotid plaque formation.
Comparison of correlations between related routine blood indexes and carotid plaque formation in both groups.
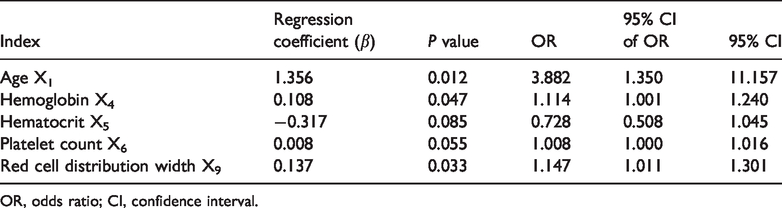
OR, odds ratio; CI, confidence interval.
Comparison of correlations between related blood biochemical indexes and carotid plaque formation between the two groups.

OR, odds ratio; CI, confidence interval; LDL, low-density lipoprotein; HDL, high-density lipoprotein.
Discussion
Atherosclerosis is a chronic, progressive systemic disease closely associated with advanced age, diabetes, coronary heart disease, hypertension, and smoking history. 8 Our study demonstrated that age was an independent risk factor for carotid plaque formation in elderly patients. Advanced age has been shown to cause disorders in cerebrovascular function, leading to the development of diseases such as hypertension and cerebral amyloidosis. 9 Hypertension can in turn damage vascular endothelial cells and induce coagulation of platelets and mononuclear macrophages, leading to atherosclerotic plaque formation. Diabetes may cause insulin resistance and hyperinsulinemia; thus, diabetes is also an important risk factor for atherosclerosis formation. 10
We further identified correlations between instability of carotid artery plaques and the red blood cell distribution width, total cholesterol concentration, hemoglobin concentration, and LDL cholesterol concentration in elderly patients. These findings are consistent with previous studies showing that increases in these parameters are correlated with the occurrence of carotid atherosclerosis in patients with diabetes and peripheral arterial disease.11,12 Early administration of lipid-lowering drugs (statins) may increase the stability of atherosclerotic plaques and reduce the occurrence of ischemic cerebral apoplexy. Previous evidence has revealed that the stability of atherosclerosis plaques plays a decisive role in plaque rupture. 13 In this study, the carotid atherosclerotic plaques mostly occurred in the carotid bifurcation, and most of them were soft plaques.
This study has two main limitations. First, other cardiovascular risk factors, such as the body mass index, smoking history, and dietary habits, were not analyzed in this study. Second, the sample size was relatively small and the patients were from the same hospital. Further investigations with a multicenter design, larger sample size, and more carotid atherosclerosis-related risk factors are needed to validate the findings of the current study.
In conclusion, carotid atherosclerotic plaque formation is a predictor of the occurrence of cerebral infarction or arterial sclerosis disease. B-Flow imaging can be used to evaluate the morphology, characteristics, and hemodynamic changes of atherosclerotic plaques. For patients with potential stroke, early ultrasound examination of the carotid artery enables the identification of vulnerable atherosclerotic plaques in the carotid artery as well as the risks associated with stroke.
Supplemental Material
sj-pdf-1-imr-10.1177_0300060520961224 - Supplemental material for Evaluation of carotid atherosclerosis and related risk factors using ultrasonic B-Flow technology in elderly patients
Supplemental material, sj-pdf-1-imr-10.1177_0300060520961224 for Evaluation of carotid atherosclerosis and related risk factors using ultrasonic B-Flow technology in elderly patients by Hai-Ying Gong, Xiao-Ke Shi, Heng-Quan Zhu, Xian-Zhong Chen, Jiang Zhu and Bo-Wen Zhao in Journal of International Medical Research
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.