
Abstract
Although customized three-dimensional tantalum implants have been used to treat a large variety of diseases, few reports have described the application of such implants to reconstruct large pelvic bone defects after the removal of massive tumors. We herein describe a 30-year-old woman with a 9-year history of a massive low-grade chondrosarcoma in the pelvic bone. After removal of a solid 12- × 8- × 6-cm tumor with clear margins, we used a customized three-dimensional printed tantalum implant to fill the large pelvic bone defect and performed hip arthroplasty in a one-step surgery. The patient’s postoperative recovery was uneventful. She started walking 1 month after surgery, and she developed no tumor recurrence, instrumentation failure, or implant loosening during the 12-month follow-up period. This report describes the successful application of a customized three-dimensional printed implant to reconstruct a massive pelvic bone defect. Satisfactory functional recovery was achieved with no apparent complications. The methodology of the current case may benefit orthopedic and oncologic surgeons in designing treatment strategies for similar cases.
Keywords
Introduction
Chondrosarcoma is one of the most common orthopedic tumors in adults. This tumor can grow to a large size because of its mild effect on movement and that most patients feel pain only when the tumor reaches considerable size. This is especially true of patients in some rural areas with less than ideal healthcare conditions.1–3 The most common sites of chondrosarcoma are the pelvis, femur, and tibia. After resection of a pelvic tumor, reconstruction of the skeletal defect is extremely challenging because of the complex structure of the pelvic bone and vital structures in this region.4,5 Although huge developments have been made in the design of prosthetic implants, they still fail to meet the demand for quick and stable reconstruction of the pelvic bone without the application of large allogeneic or autogenic bone transplants. The stress shielding effect due to inadequate matching of the implant and host bone tissue detrimentally affects the bone–implant interaction and can cause atrophy of the bone and loosening of the graft.6–8
Three-dimensional (3D) printing technology has been widely applied in various industries from construction to medicine and space industry. Several orthopedic implants have received FDA approval for clinical application. 3D printing can create implants of any shape with high precision. The micropores on the implants promote adherence of osteocytes, which further promotes implant stability.9,10
We herein report a case involving a patient with a giant pelvic chordoma who was treated by customized 3D printed tantalum implant-based reconstruction of the massive pelvic bone defect after removal of the tumor. The patient achieved satisfactory functional recovery with no apparent complications. Because the complexity and extent of this surgical procedure are not well described in the current literature, the treatment methodology applied in the current case may benefit surgeons in designing treatment strategy for similar cases.
Case report
A 30-year-old woman sought medical attention in our department for a recurrent iliac tumor. Ten years previously, she had felt a growing lump and pain in her right iliac bone that intensified with walking. She was admitted to a local hospital, where the surgeons removed an osseous tumor from her iliac bone, and the subsequent pathological studies showed that it was a low-grade chondrosarcoma. Three years before presentation, the patient felt pain while walking and noticed a similar lump in the previously operated area. Fifteen months before presentation, she visited her local hospital because of increasing pain and growth of the lump in her right iliac bone. Pathological studies following fine needle aspiration showed the same diagnosis of low-grade chondrosarcoma. Three months later, the patient visited our department for more specialized surgical treatment. Physical examination after admission showed a 4- × 4- × 3-cm lump with a clear boundary and no mobility. The patient reported mild tenderness when placing pressure on the lump. The patient had no active infection or skin impairment that could prevent us from scheduling a surgery, no sensory deficiency, and no muscle atrophy. No abnormalities were found in the muscle strength, sensory function, or circulation of the lower extremities. Computed tomography (CT) scans of the pelvic bone showed osteolytic damage in the right iliac body and iliac wing with a large soft tissue mass (Figure 1). A CT-guided biopsy suggested grade I chondrosarcoma.

Three-dimensional reconstruction of the patient’s computed tomography scan.
Because chondrosarcoma is not sensitive to chemotherapy, and considering the availability of a safe and mature technique with which to remove the lesion in a one-step surgical procedure, we considered one-step surgery to be the optimal treatment regimen. Any contraindications for surgical intervention were ruled out with a comprehensive blood test and examinations of the patient’s circulatory, respiratory, urinary, and gastrointestinal systems. Magnetic resonance imaging was performed to exclude early tumor penetration of the pelvic bone outside the large bone mass. After completion of all preoperative evaluations, surgery was scheduled with the consent of the patient and her family. The 3D printed tantalum implant was prepared by reconstruction of the patient’s CT scan with a spatial resolution of 20 lp/cm and density resolution of 0.67 mm (Figure 2).

Designing and molding of the three-dimensional implant used in the current case. (a–c) Design of the implant from different angles. (d) Three-dimensional printed model of the implant with the pelvic bone. (e, f) Three-dimensional printed tantalum implant.
Images of the patient’s pelvic bone and chondrosarcoma were obtained by a CT scanner (Siemens Healthineers, Erlangen, Germany), and the scan data from the Picture Archiving and Communication System (PACS) were reconstructed by Mimics 17.0 software (Materialise NV, Leuven, Belgium). The extent of the lesion was outlined, and the preoperative surgical plan was established using the 3D model. The 3D data including the surgical plan was stored in STL format and sent to an engineer for implant printing. The implant was designed by an engineer according to the surgical plan, bone quality, and patient’s overall condition (e.g., weight and height) under the parameters of “Personalized Additive Manufactured Medical Device Technical Censoring Guidelines (February, 2018)” by the Center for Medical Device Evaluation of China (www.cmde.org.cn). Finite element analysis was carried out to evaluate the probable biomechanical stress distribution of the implant. A porous structure was used in the 3D painted implant to avoid bone resorption and implant loosening from stress shielding. The implants were 3D printed using tantalum powder by Xi’an Sailong Metal Materials Co., Ltd. (Xi’an, China). The density of the implant was 2.7 g/m3, the diameter of each aperture was 200 µm, and the extent of porosity was 40%. The muscle and ligament suturing points were designed according to the pelvic CT and magnetic resonance imaging scans. Tumor recession guidance plates were designed to cut the tumor 2 cm beyond tumor border, and a 3-mm-diameter hole was made in the middle of the plate to fix it to the bone with a 2.5-mm-diameter Kirschner wire (Figure 3).

Preoperative surgical planning and three-dimensional printed surgical guidance templates. (a, b) Preoperative planning of the resection margin. (c, d) Three-dimensional printed surgical guidance templates.
Surgical procedure
The patient was treated by en bloc resection of the chondrosarcoma in the right iliac bone, reconstruction of the iliac bone with the 3D tantalum implant, right total hip arthroplasty, and adjacent skin flap reconstruction (Figure 4). The patient was fixed in the left lateral position after induction of general anesthesia. A 29-cm-long Watson–Jones incision was made from the right iliac crest to the right anterolateral thigh. The subcutaneous tissue and deep fascia were excised and the periosteum of the right iliac bone around the tumor was exposed while maintaining the integrity of the tumor capsule. The 3D printed guidance plate was then fixed on the iliac bone with Kirschner wires, and the tumor was extracted without exposing any tumor tissue to the normal tissue. The right superior acetabulum, femoral head, and part of the iliac body were resected and sent for pathological diagnosis. The 3D printed tantalum implant was placed in the bone defect and fixed to the existing pelvic structure with screws. The femoral neck was exposed by abduction, internal rotation, and flexion of the hip joint, and it was then sawed 1 cm superior to the lesser trochanter by a swing saw. The right acetabulum was exposed, and acetabular reamers were used to prepare the acetabulum. After the articular cavity was washed repeatedly by iodophors and physiological saline, 4 g of gentamicin-loaded bone cement (DePuy Synthes, Raynham, MA, USA) was used in the articular cavity to attach a 50-mm-diameter PINNACLE Acetabular Cup System (DePuy Synthes) with titanium as the bearing material and a ceramic-on-ceramic interface. The acetabular cup prosthesis was fixed to the pelvic prosthesis by bone cement. After the femoral medullary cavity was satisfactorily reamed and the femoral stem (#8; Johnson & Johnson, New Brunswick, NJ, USA) and femoral head prosthesis (M-SPEC porcelain, Φ32 mm; Johnson & Johnson) were inserted, the hip joint was restored. After assuring the mobility of the joint, the surgical field was washed with sterile physiological saline. The iliotibial tract, quadriceps femoris muscle, and iliacus muscle were repaired, and the incision was sutured by layers over a drainage tube. The total operative time was 4 hours, and the total intraoperative hemorrhage volume was 700 mL. A solid 12- × 8- ×6-cm tumor with clear margins was extracted and cut open in vitro. White bone-like tissue with little tissue necrosis was observed. Pathological examination of the specimen confirmed the preoperative diagnosis of low-grade chondrosarcoma (Figure 5).
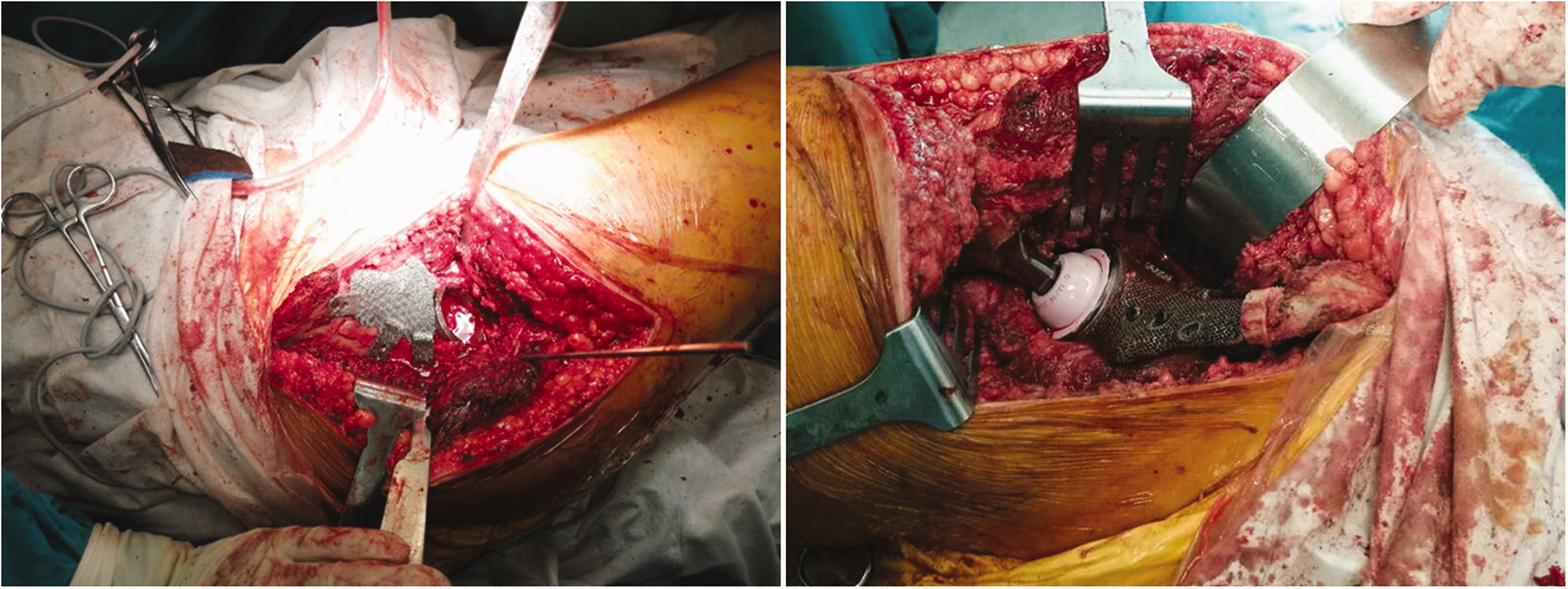
Surgical procedure of tumor resection and three-dimensional implant fixation.

Pathological studies of the intraoperative specimen confirmed the preoperative diagnosis of mucinous chondrosarcoma.
After the surgery, cefuroxime was used to prevent surgical site infection. The patient developed a low blood hemoglobin concentration and thus received an infusion of 300 and 400 mL of suspended red blood cells on postoperative day 4 and 6, respectively. Because of the extensive surgical removal of the tumor and surrounding tissues and the introduction of the large 3D printed tantalum implant, it was important to avoid postoperative infection due to inadequate drainage. Therefore, the drainage tubes were removed only after the daily drainage volume reached <50 mL, which in this case took a few more days than in conventional surgeries. The sutures were removed 14 days after surgery. No supportive brace was required postoperatively because of the strong support provided by the implant. The patient began performing exercises to enhance hip movement and quadriceps strength. At 24 hours after surgery, a continuous passive motion device was used to further increase the range of motion and improve postoperative recovery. The patient started walking with crutches 1 month after surgery and walking without a supportive brace 2 months after surgery. The patient was scheduled for outpatient visits at 1, 2, 3, 6, and 12 months postoperatively and once a year thereafter. She reported no pain with walking by 6 months postoperatively. No tumor recurrence, instrumentation failure, or implant loosening was observed during follow-up. The patient could walk without assistance 1 year after surgery (Figure 6, Video 1).

No failure or loosening of the implant had occurred at 1 year postoperatively.
Discussion
Giant chondrosarcomas in the pelvic region are difficult to remove because of the complex anatomical structure of the pelvic bone and surrounding vital organs. In patients with a long disease history, the tumor is always massive, and wide margin resection to avoid recurrence along with reconstruction with a sufficient biomechanical stress load can be even more challenging because of the large bone defect.11–13
With the developments in tissue engineering material technology, medical imaging, and 3D imaging techniques, computer-aided design of 3D orthopedic surgical implants is being more frequently used by surgeons.14,15 In the present case, we obtained the CT data from the PACS, used Mimics 17.0 software for reconstruction, and used a 3D printing system to print out the implant.
Several reports have described the application of 3D printed implants in orthopedic surgeries, including pelvic, femoral, and tibial arthroplasty.16–20 A group of spine surgeons in China used a customized artificial vertebral body fabricated according to a computer model using tantalum powder to reconstruct the cervical spine of a 12-year-old boy with Ewing sarcoma of the C2 vertebra after staged spondylectomy. 21 One year after the surgery, implant osseointegration was confirmed in sagittal reconstruction images as indicated by bone ingrowth into the built-in vertical slit in the center. The patient developed no tumor recurrence and had no residual neurologic deficits, and his neurological function score improved to 16 points on the 17-point Japanese Orthopedic Association scale. 21 Wong et al. 22 used a computer-aided design implant that matched both the bone defect and biomechanically evaluated 3D printed implant to recover hip function after complex pelvic tumor resection. The patient achieved pain-free motion 11 months after surgery without tumor recurrence or implant loosening. In the current study, we treated one of the largest bone defects that has been reconstructed with a 3D printed customized tantalum implant to date. Although several reports have described the application of similar 3D printed customized implant techniques in various reconstruction procedures, reports of the complexity and extent of the surgical procedure are still rare in the current literature. The methodology of this case may benefit orthopedic and oncologic surgeons in designing treatment strategies for similar cases.
Successful application of a 3D printing technique to treat a giant chondrosarcoma of the pelvis requires close collaboration between the radiologist, surgeon, and engineer. The surgeon should be able to anticipate the precise margin of bone removal and carry out the planned surgical procedure to fit the custom implant into the bone defect without the need for extensive adjustment or bone transplantation.23–25
Despite the numerous advantages of 3D printed implants over traditional implants, this is still a novel technique that requires improvement before further clinical applications. The biocompatibility and mechanical strength of printed implants should be increased, and more precise implant designs are needed to avoid stress shielding and promote bone–implant integration. Such developments will require more collaboration among surgeons, radiologists, and engineers.
Footnotes
Ethics and consent
The study was approved by the ethics committee of the Southwest Hospital of Third Military Medical University of China. The patient provided written consent to publish her clinical materials.
Availability of data and material
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the National Key Research and Development Plan (2016YFB1101404), Guangdong Provincial Key R&D Program: Industrialization Technology Research and Application Demonstration of Additive Manufacturing Customized Metal Tantalum Implant (Grant No. 2018B090906003), Chongqing Science and Technology Commission R&D Base Construction Program (International Cooperation): Research and Development of Customized Orthopedic Implants Based on 3D Metal Printing Technology (Grant No. cstc2014gjhz110003), and Key Neighborhood Technology Innovation Project of The First Hospital Affiliated to the Third Military Medical University: Research and Development and Clinical Application of 3D Printing Medical Products (Grant No. SWH2016ZDCX2010).
Authors’ contributions
ZL, GC, YX, and AM analyzed the data and drafted the manuscript. HF, JL, and CC performed the surgical procedure. JL and CC stored the clinical materials and were in charge of patient follow-up. XW and PH analyzed the radiological data and prepared the 3D implant. FW and LY planned the study, acquired the funds, and coordinated the whole study. All authors read and approved the manuscript.
Supplemental material
Supplemental material for this article is available online.