
Abstract
Immunoglobulin G4 (IgG4)-related disease (IgG4-RD) is a novel clinical disease that is characterized by elevated serum IgG4 concentrations and tumefaction or tissue infiltrated by IgG4+ plasma cells. The clinical manifestations of IgG4-RD depend on the type of tissues affected. IgG4-related sclerosing cholangitis is a type of IgG4-RD. We report a patient who initially visited a local hospital with a 5-month history of jaundice. He was found to have a mass in the upper part of the common bile duct that mimicked cholangiocarcinoma. He underwent surgery in our hospital and was later diagnosed with IgG4-related sclerosing cholangitis. We administered prednisolone 40 mg once a day for treatment. Taking into account the possible side effects of moderate-dose hormone therapy, we also administered teprenone, potassium chloride, and calcium carbonate. The patient did not have any recurrence of symptoms or adverse drug reactions during follow-up.
Keywords
Introduction
Immunoglobulin G4 (IgG4)-related disease (IgG4-RD) is a novel clinical disease characterized by elevated serum IgG4 concentrations and tumefaction or tissue infiltration by IgG4+ plasma cells. 1 IgG4-related sclerosing cholangitis is a form of IgG4-RD characterized by jaundice and irregular narrowing of the main bile duct. The presence of a hypermetabolic bile duct mass allows IgG4-related sclerosing cholangitis to mimic cholangiocarcinoma. Distinguishing IgG4-related sclerosing cholangitis from cholangiocarcinoma is important because the clinical course, treatment, and prognosis of these two diseases markedly differ. 2 Most types of IgG4-RD respond well to glucocorticoid therapy, including IgG4-related sclerosing cholangitis, while cholangiocarcinoma may require surgery with or without adjuvant chemotherapy. 3 We report a patient with IgG4-related sclerosing cholangitis who presented with a mass that mimicked cholangiocarcinoma.
Case presentation
A 53-year-old man presented to a local hospital with a 5-month history of jaundice. He was afebrile and had no nausea, vomiting, abdominal pain, or diarrhea. The jaundice was not associated with food, alcohol, or medicine intake, and there was no history of hepatitis infection. Laboratory tests showed markedly elevated liver enzymes as follows: alanine aminotransferase level, 435 IU/L; aspartate transaminase level, 244 IU/L; total bilirubin level, 165.9 μmol/L; and direct bilirubin level, 101.4 μmol/L. Magnetic resonance cholangiopancreatography (MRCP) showed a mass in the common bile duct suggestive of bile duct carcinoma (Figure 1). He was diagnosed with cholangiocarcinoma in the local hospital and referred to our surgical department.
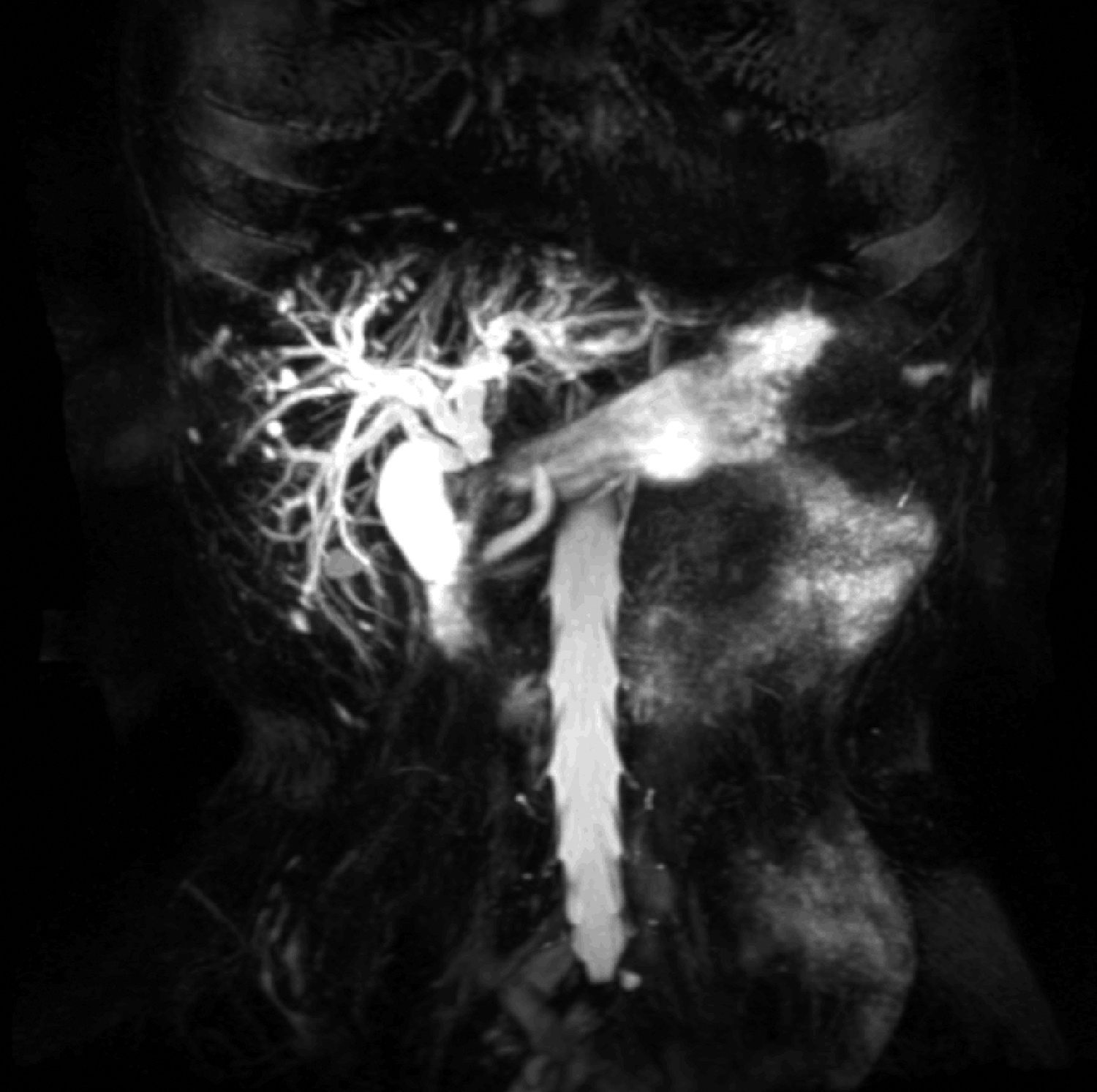
Magnetic resonance cholangiopancreatography shows a mass in the common bile duct suggestive of bile duct carcinoma.
Ultrasound of the liver and gallbladder in our hospital showed thickening in the middle section of the common bile duct and a dilated intrahepatic bile duct. Computed tomography (CT) of the liver and gallbladder showed a nodular soft tissue density in the upper part of the common bile duct (Figure 2), which measured 12 × 15 mm, swelling of the upper liver, and dilation of the internal bile duct. Repeated liver function tests showed the following: alanine aminotransferase level, 50 IU/L; aspartate transaminase level, 53 IU/L; total bilirubin level, 29.9 μmol/L; and direct bilirubin level, 20.6 μmol/L. The patient was diagnosed with cholangiocarcinoma by a hepatobiliary surgeon and underwent surgery.

Computed tomography of the liver and gallbladder shows nodular soft tissue density in the upper part of the common bile duct, which measures 12 × 15 mm, swelling of the upper liver, and dilation of the internal bile duct.
At 2 weeks postoperatively, the pathology of the excised specimen was reported as proliferative fibrous tissue with plasmocyte infiltration related to IgG4-RD (Figures 3, 4, and 5). He was then transferred to the Department of Rheumatology for treatment and revaluation of his condition. Cardiac ultrasonography showed mitral regurgitation and pulmonary hypertension (44 mmHg). Chest CT showed a slightly thicker bronchial wall and fibrosis in the right middle lung. Ultrasonography of the thyroid gland and bilateral parotid and submandibular glands showed no obvious abnormalities. Ultrasonography of the hepatobiliary system, bile duct, and gallbladder showed a normal-sized liver that contained three cystic dark areas, which measured approximately 1 cm, with clear boundaries. The echoes in the remaining liver parenchyma were evenly distributed. The common bile duct was not observed. Ultrasonography of the pancreas and spleen showed a normal-appearing spleen. The shape and internal echo of the pancreas were normal and the main pancreatic duct showed no obvious dilation or space-occupying lesions. Urinary ultrasonography showed no obvious space-occupying lesions. Ultrasound of the neck, axilla, groin, and posterior peritoneal area showed no obviously enlarged lymph nodes. There were multiple hypoechoic subaxillary lymph nodes. The cortex and medulla were clear. The subaxillary lymph nodes measured 3.21 × 1.36 cm on the left and 2.78 × 1.28 cm on the right. A left axillary lymph node biopsy showed lymphoid-reactive hyperplasia with focal fibrosis and a high number of IgG4 cells. The patient’s serum IgG4 level was 6.55 g/L (normal range: 0.03–2.01 g/L). Other blood tests, including a routine cell count and chemistry, liver and kidney function, anti-nuclear antibody, anti-neutrophil cytoplasmic antibody, hepatitis B antibody, and tumor markers, were normal. We diagnosed the patient with IgG4-related sclerosing cholangitis.
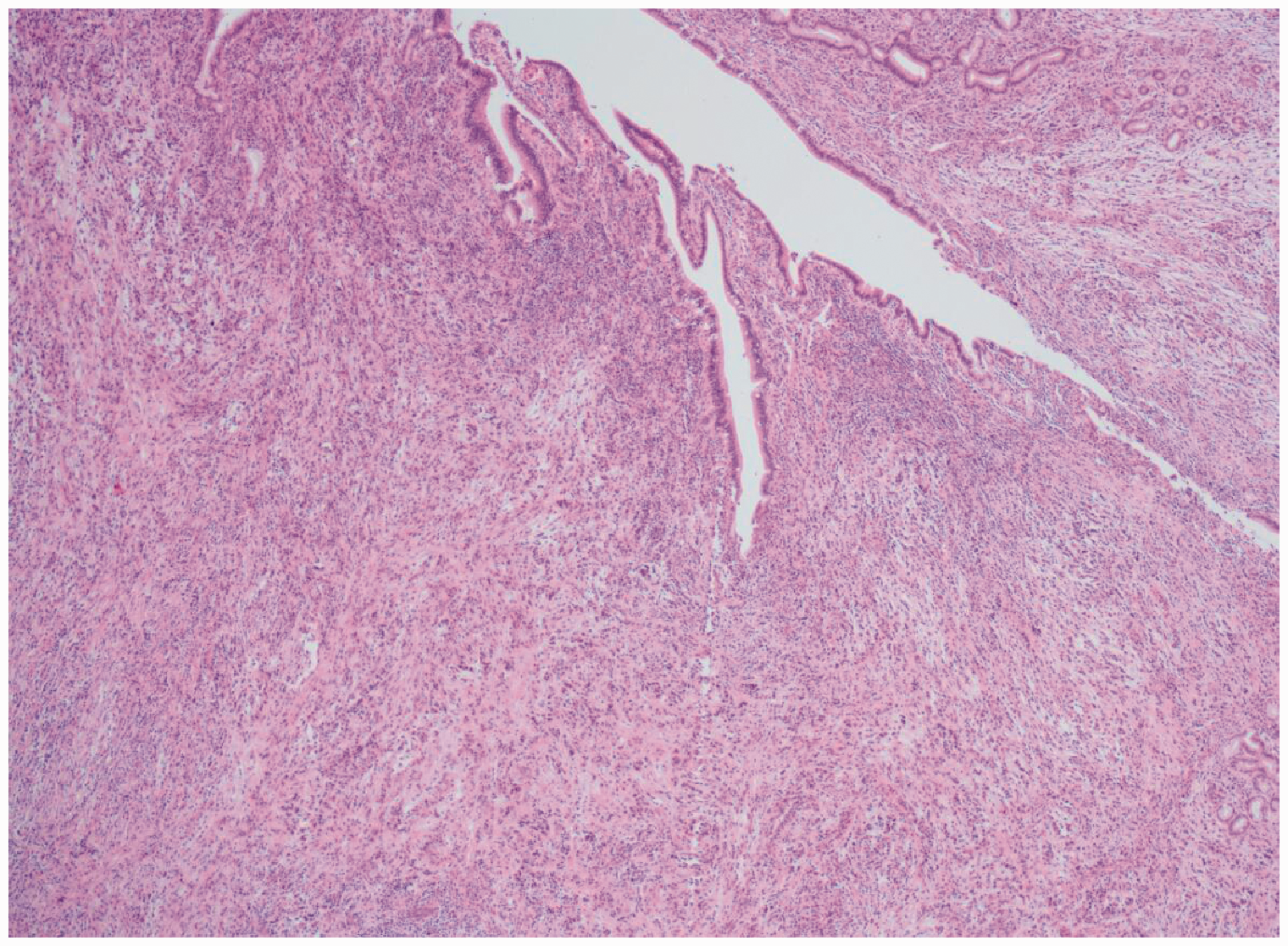
Histology using hematoxylin and eosin staining shows extensive fibrotic tissue and infiltration of lymphocytes. Magnification, ×40.

Histology using hematoxylin and eosin staining shows obliterative venulitis (arrow). Magnification, × 100.

Immunohistochemistry shows a large number of immunoglobulin (Ig) G4-positive plasma cells infiltrating the tissue. The IgG4+/IgG+ ratio is approximately 50% to 60%. Magnification, × 200.
We followed the recommendations of guidelines and initially administered prednisone 40 mg once a day for 2 weeks for treatment. 4 The prednisone dose was then reduced by 5 mg every 2 weeks. When prednisone was reduced to 20 mg per day, we reduced the dose more slowly. Currently, the patient is being treated with 2.5 mg prednisone per day. Taking into account the possible side effects of moderate-dose hormone therapy, we also administered teprenone 50 mg three times a day, potassium chloride sustained-release tablets 1 g twice daily, and calcium carbonate D3 tablets 0.6 g orally once a day. The patient did not show recurrence of symptoms or adverse drug reactions during follow-up. We are currently following the patient.
Discussion
Our patient visited the hospital because of jaundice, which is a non-specific finding. His CT and MRCP results suggested cholangiocarcinoma. The diagnosis of IgG4-related sclerosing cholangitis was confirmed after examination of the surgical specimen showed inflammation of the bile duct and IgG4+ plasma cell infiltration, and laboratory tests showed an elevated serum IgG4 level. 5 Unfortunately, the patient underwent unnecessary surgery. The patient was initially misdiagnosed because IgG-RD is easily overlooked by doctors because of its low incidence. In fact, this disease was not recognized until 2003, 6 and the prevalence of various organ manifestations remains unclear. The estimated prevalence of IgG4-related autoimmune pancreatitis in Japan is 2.2 cases per 100,000 population. 7
Although imaging is an important part of the diagnostic approach to many diseases, imaging findings of most organs are not always specific because distinguishing tumors can be difficult. IgG4-related sclerosing cholangitis is characterized by irregular narrowing or a mass in the main bile duct because of massive infiltration of IgG-positive plasma cells with associated fibrosis within the bile duct walls, resulting in focal wall thickening. On the basis of such characteristics, IgG4 sclerosing cholangitis is divided into four types by cholangiography. 8 Type 1 IgG4 sclerosing cholangitis involves stenosis in the lower bile duct. In type 2 IgG4 sclerosing cholangitis, stenosis is diffusely distributed throughout the intrahepatic and extrahepatic bile ducts. Type 3 IgG4 sclerosing cholangitis is characterized by stenosis in the hilar hepatic lesions and lower bile duct. Type 4 IgG4 sclerosing cholangitis presents with strictures of the bile duct only in hilar hepatic lesions. After we re-evaluated our patient’s cholangiography, type 4 IgG4 sclerosing cholangitis appeared to be present. This finding can appear to be similar to cholangiocarcinoma. Typically, IgG4-RD is a subacute, slowly progressive disease and patients may not develop symptoms for months or years. 1 Clinicians cannot easily diagnose IgG4-RD because of its hidden course.
Patients who are diagnosed with IgG4-RD can have multi-organ involvement, including the pancreas, lacrimal, and salivary glands, orbital or periorbital tissue, pachymeninx, hypophysis, thyroid, lungs, pleura, pericardium, kidneys, prostate, mediastinum, and retroperitoneum. 9 Therefore, we carefully assessed these areas in our patient using CT and ultrasound. Positron emission tomography-CT can help to determine the extent of organ involvement and can also be helpful for monitoring disease activity after treatment. 10 We did not perform positron emission tomography CT because of the cost.
With regard to the treatment of IgG4-RD, prednisone with a dose of 30 to 40 mg/day is a common initial treatment. 4 Japan also has relevant diagnosis and treatment guidelines. These guidelines suggest oral prednisolone at 0.6 mg/kg/day for 2 to 4 weeks for initial remission-induction therapy. 11 Prednisolone is recommended to be reduced by 5 mg every 1 to 2 weeks after induction of remission, while confirming the response to steroid therapy by laboratory tests and imaging studies (e.g., ultrasonography, CT, or MRCP). Prednisolone should then be gradually tapered further to a maintenance level by 2 to 3 months. Our approach to treating our patient was based on these guidelines. We administered an initial dose of 40 mg prednisone for 2 weeks. The patient is currently being treated with 2.5 mg prednisone per day. During follow-up, the patient did not show recurrence of symptoms or obvious adverse drug reactions. A previous case report on IgG4-related sclerosing cholangitis showed that the response rate with steroid treatment was 72.3% to 97%, while the disease relapse rate was 19% to 66.1% after steroid withdrawal. 12 For some patients with a poor response to prednisone treatment or relapse repeatedly after hormone reduction, immunosuppressive therapy can be considered. 13
Conclusion
Findings in our case suggest that clinicians should have some understanding of IgG4-RD, especially surgeons. Only a few patients with IgG4-RD who develop symptoms present to the Rheumatology Department in a timely manner. Physicians should not rely on imaging and serum IgG4 levels for a diagnosis, although serum IgG4 levels have a reference value. 14 Histopathology is the gold standard for diagnosis of IgG4-RD. Awareness of the differences between IgG4-related sclerosing cholangitis and cholangiocarcinoma may avoid misdiagnosis and unnecessary surgical intervention.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Ethics statement
The study protocol was approved by the Ethics Committee of Zhejiang University School of Medicine Sir Run Run Shaw Hospital. The patient participating in the study provided verbal informed consent for publication. To protect the privacy of the patient, we de-identified the details such that the identity of the patient may not be ascertained in any way.
Funding
This study was supported by Grant No. 2017KY399 from the Health Commission of Zhejiang Province.