
Abstract
Objective
Dexmedetomidine has a good sedative effect and does not affect the judgment of the patient's consciousness level. However, its effectiveness for sedation and cerebral protection after craniotomy in hypertensive intracerebral hemorrhage (HICH) patients is unknown.
Methods
A retrospective study of 164 postoperative HICH patients who underwent sedation with dexmedetomidine or midazolam was conducted. The Ramsay sedation score, mean arterial pressure (MAP), heart rate (HR), pulse oxygen saturation (SpO2), and respiratory rate were measured at the indicated time points. Human soluble protein-100β (S-100β) and neuron-specific enolase (NSE) levels were also compared between the two groups.
Results
Dexmedetomidine treatment showed a significantly better effect than midazolam on decreasing the frequency of apparent agitation. The MAP and HR, but not the SpO2, were significantly decreased and lower than those in midazolam group. Detection of plasma S-100β and NSE proteins revealed a significant decrease in the dexmedetomidine group compared with the midazolam group. The 6-month follow-up evaluation indicated a significantly better prognosis of postoperative HICH patients treated with dexmedetomidine than for those treated with midazolam.
Conclusions
Dexmedetomidine is effective for sedation in postoperative HICH patients and may be beneficial for their outcome.
Keywords
Introduction
Hypertensive intracerebral hemorrhage (HICH) refers to rupture and hemorrhage of small arteries because of pathological changes in the brain caused by prolonged hypertension and cerebral arteriosclerosis. 1 Among the various causes of non-traumatic intracerebral hemorrhage, hypertension accounts for approximately 60% of cases. HICH is one of the most serious complications of hypertension 2 and is common in 50- to 60-year-old patients, and the incidence in men is slightly higher than that in women. HICH is one of the most serious diseases that threaten the health of the elderly. 3 Treatment of HICH is usually conservative. However, some patients suffer from excessive bleeding and coma, often requiring surgical treatment; that is, hematoma removal is performed to relieve the hematoma, brain tissue compression, and secondary brain injury. 4 Postoperative restlessness is a common clinical symptom in HICH patients. Restlessness can lead to sympathetic activation, increased oxygen consumption and brain metabolism, and even cardiovascular events in elderly patients, which are not conducive to disease recovery. 5 Severe agitation can cause great fluctuation of blood pressure, which results in repeat rupture of the blood vessel, leading to increased brain hematoma and even the risk of brain hernia. 6 Proper sedation can improve patient comfort, prevent severe fluctuations in blood pressure, and reduce re-bleeding. 6 Therefore, it is necessary to select reasonable sedative drugs to relieve stress and restlessness.
The benzodiazepine sedative midazolam is widely used in clinical practice. However, in recent years, dexmedetomidine has attracted increasing attention from anesthetic and intensive care unit clinicians because it can produce the approximate sedative effect of natural sleep and exhibits weak respiratory depression. 7 Dexmedetomidine is a highly selective and specific α2 adrenergic receptor agonist and a common adjuvant anesthetic in clinical practice. It mainly acts within the locus coeruleus, produces sedative, hypnotic and anxiolytic effects, activates presynaptic membrane α2 receptors, inhibits the release of norepinephrine, terminates the transmission of pain signals, and inhibits sympathetic activity and the stress response. 8 Some studies have shown that dexmedetomidine also has certain neuroprotective effects. Zhao et al. 9 confirmed that dexmedetomidine has protective and hemodynamic effects in HICH patients during the perioperative period. Therefore, we analyzed the effects of dexmedetomidine on sedation and reducing recurrence after hematoma removal in postoperative HICH patients.
Materials and methods
Statement regarding human participants
All methods and treatments in this study were performed in accordance with the Declaration of Helsinki and the relevant regulations. The protocols for the study and the written consent form were approved by the ethics committee of the First People’s Hospital of Kunshan, China (201907621). The study was approved by the Ethics Committee of each hospital. Written informed consent was obtained from all patients providing tissue specimens prior to surgery, and all patients consented to the submission of this report for publication.
Inclusion and exclusion criteria
Patients were enrolled based on the following inclusion criteria: primary hypertension, evidence of basal ganglia cerebral hemorrhage by computed tomography (CT), and evacuation of hematoma. The exclusion criteria were as follows: (1) patients with hemorrhage in other parts of the brain; (2) patients complicated with chronic liver disease, heart disease or arrhythmia, and diseases of the kidney, lung, and other vital organs; (3) patients complicated with severe coagulation abnormalities; (4) patients complicated with malignant tumors or hematologic diseases.
Design and therapeutic process
All HICH patients underwent surgical intervention, including trepanation of a single burr hole and irrigation of the hematoma with urokinase two times a day or removal of the hematoma through a small bone window. The former procedure was performed on 80 patients, and the latter procedure was performed on 84 patients. All patients underwent general anesthesia. A routine cranial CT examination was performed on the first and second days after surgery. If the patient’s condition worsened, cranial CT was performed again. The drainage tube was usually removed at 2 to 3 days after surgery according to the patient's condition.
Patients in the dexmedetomidine group were first given a loading dose of 1 μg/kg of dexmedetomidine and then maintained on a dosage of 0.3 to 0.6 μg/kg/h. Patients in the control group were first given a loading dose of 0.05 mg/kg of midazolam and then maintained on a dosage of 0.02 to 0.10 mg/kg/h. The medication was adjusted to achieve and maintain a Ramsay sedation score of 2 to 4 for a satisfactory sedation effect. The use of sedative drugs was continued until the patient had no obvious irritability. Labetalol hydrochloride and urapidil were routinely used to control hypertension after the operation. Labetalol hydrochloride (100 mg) was diluted in 250 mL of a 5% glucose and 0.9% sodium chloride solution and administered with an intravenous drip rate of 1 to 4 mg/minute. According to recommendations, urapidil was initially delivered at 2 mg/minute, and the maintenance rate of delivery was 9 mg/hour. The degree of blood pressure decline was determined by the dose of the drug administered within the first 15 minutes, and then drug delivery was maintained at a low dose.
Routine follow-up was generally conducted twice a month until 6 months after the operation.
Ramsay sedation score
The Ramsay sedation score criteria are as follows: 1, the patient is anxious and agitated, restless, or both; 2, the patient is cooperative, oriented, and tranquil; 3, the patient responds to commands only; 4, the patient is asleep and shows a brisk response to a light glabellar tap or loud auditory stimulus; 5, the patient is asleep and shows a slow response to a light glabellar tap or loud auditory stimulus; 6, the patient is asleep and shows no response to a light glabellar tap or loud auditory stimulus.
Monitoring index
The Ramsay sedation score, mean arterial pressure (MAP), heart rate (HR), pulse oxygen saturation (SpO2), and respiratory rate (RR) were recorded before and after the medication was administered. The amount of fentanyl used and the degree of respiratory depression and agitation during the course of sedation were also recorded. An enzyme-linked immunosorbent assay was used to detect the human soluble protein-100β (S-100β) and neuron-specific enolase (NSE) levels in the plasma of the two groups of patients before (0 hours) and after surgery (6 hours and 12 hours).
Glasgow Outcome Scale (GOS) scores
GOS scores were evaluated at the 6-month follow-up evaluation after surgery as follows: 1, death; 2, persistent vegetative state; 3, severe disability; 4, moderate disability; 5, mild or no disability. GOS scores of 4 or higher indicated a good outcome.
Statistical analysis
The data were analyzed using SPSS version 15.0 (SPSS Inc., Chicago, Illinois). Quantitative variables such as age and body temperature are expressed as the mean ± SD. We used the χ2 or Fisher’s test to analyze associations between categorical variables and the t-test to analyze continuous variables. Multiple logistic regression analysis was adopted to analyze correlations between variables. A value of P < 0.05 was considered statistically significant.
Results
Patients
A total of 164 HICH patients with dysphoria after neurosurgery (Ramsay score of 1) who were admitted to various hospitals from 2015 to 2017 were selected as subjects, including 98 men and 66 women. The preoperative Glasgow Coma Scale (GCS) ranged from 8 to 12 points. According to whether dexmedetomidine was used after the operation, the patients were divided into a dexmedetomidine group (86 patients) and a midazolam group (78 patients).
No significant differences in routine monitoring indexes were observed between the two groups
The demographic and clinical characteristics of the two groups are shown in Table 1. No significant differences of monitoring indexes, including age, sex, and weight, MAP, temperature (°C), HR, and RR were found between the dexmedetomidine group and the midazolam group after the operation and before dexmedetomidine or midazolam administration (Table 1). Additionally, the preoperative GCS scores and hematoma volume were also compared and showed no differences (P > 0.05).
The demographic and clinical characteristics of patients in the dexmedetomidine and midazolam groups before drug administration.

MAP, mean arterial pressure; HR, heart rate; RR, respiratory rate; GCS, Glasgow Coma Scale.
Sedative effect of dexmedetomidine and midazolam
As shown in Table 2, to achieve a satisfactory sedation effect with a Ramsay sedation score of 2 to 4, dexmedetomidine administration for 17.97 ± 6.59 minutes was required, while midazolam administration for 16.72 ± 6.01 minutes was required. Statistical analysis showed no difference in sedation between the two groups. However, during the 48 hours following sedation, the frequency of apparent agitation in the dexmedetomidine group was 4.53 ± 2.48 events, which was significantly lower than that in the control group (9.50 ± 4.22 events) (P < 0.05). Respiratory depression is a frequent occurrence during sedation. We further analyzed the frequency of respiratory depression during sedation and found no cases in the dexmedetomidine group, but six cases were found with midazolam treatment (P < 0.05). These data suggest that dexmedetomidine is more effective and safer for sedation after craniotomy in HICH patients.
The Sedative effects of dexmedetomidine and midazolam.

Changes in vital signs after dexmedetomidine or midazolam treatment
Postoperative HICH patients were immediately administered dexmedetomidine or midazolam. As shown in Table 3, after dexmedetomidine administration for 1 hour or 2 hours, the MAP and HR were more obviously decreased than those in the midazolam group (P < 0.05) when neither group of patients was given oral or intravenous antihypertensive drugs. However, both of these variables could be controlled within the normal ranges. Additionally, the RR was lower after treatment than before treatment in both groups (P < 0.05); however, no significant differences in RR were found after dexmedetomidine or midazolam treatment. There was also no obvious difference in the SpO2 at various time points between the dexmedetomidine and midazolam treatment groups. These data showed that dexmedetomidine treatment could affect the MAP and HR of HICH patients after surgery. Considering that patients with primary HICH usually suffer from excessive blood pressure after surgery, we suggest that dexmedetomidine is a good choice for sedation.
Changes in vital signs after dexmedetomidine or midazolam treatment.
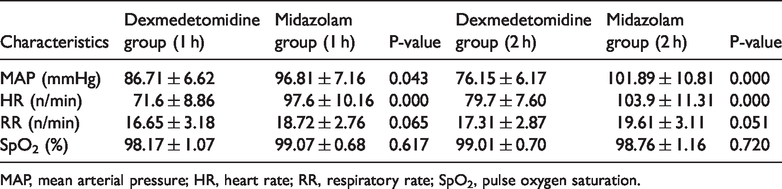
MAP, mean arterial pressure; HR, heart rate; RR, respiratory rate; SpO2, pulse oxygen saturation.
Dexmedetomidine decreased the plasma S-100β and NSE protein levels in postoperative HICH patients
S-100β and NSE are known outcome predictors of cerebral damage. 10 Here, these two markers were used to confirm whether dexmedetomidine has neuroprotective effects on postoperative HICH patients. We compared the plasma S-100β and NSE protein levels at the indicated times after dexmedetomidine or midazolam administration. Our results showed no statistically significant difference in plasma S-100β and NSE protein levels between the two groups before the operation. However, the plasma S-100β and NSE protein levels at 6 and 12 hours after surgery were significantly decreased in dexmedetomidine-treated patients compared with midazolam-treated patients (Table 4).
Changes in plasma human soluble protein-100β and neuron-specific enolase protein levels in postoperative hypertensive intracerebral hemorrhage patients.
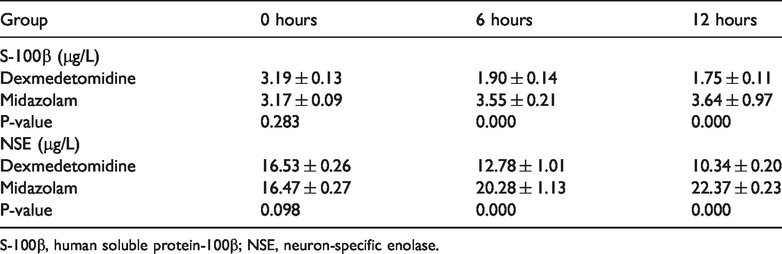
S-100β, human soluble protein-100β; NSE, neuron-specific enolase.
Dexmedetomidine was beneficial for the outcome of postoperative HICH patients
A GOS score of 4 or 5 was considered to be a good outcome for patients. After 6 months, two patients in the midazolam group were lost to follow-up. In total, 72/86 patients in the dexmedetomidine group had a GOS score of 4 or 5 compared with 53/76 patients in the midazolam group. Additionally, the χ2 test showed a significant difference in the prognosis between the dexmedetomidine and midazolam groups (P < 0.05), which indicates that dexmedetomidine administration is beneficial for the outcome of postoperative HICH patients (Table 5).
Evaluation of the long-term prognosis of patients in the two groups via the Glasgow Outcome Scale score.

GOS, Glasgow Outcome Scale.
Discussion
Midazolam is a medication used for anesthesia, procedural sedation, sleep disorders, and severe agitation that produces its effect by inducing sleepiness, decreasing anxiety, and causing a loss of the ability to create new memories. 11 Dexmedetomidine is an α2 adrenergic receptor agonist that is used in veterinary medicine because of its analgesic and sedative properties. Dexmedetomidine is notable for its ability to provide sedation without risk of respiratory depression, unlike other commonly used sedatives such as midazolam, and can produce cooperative or semi-arousable sedation. 12 As two commonly used sedative drugs, many studies have been conducted to evaluate the sedative effects of dexmedetomidine and midazolam. In a systematic review of its efficacy and safety, Barends et al. reported that dexmedetomidine is a promising alternative to midazolam for use in procedural sedation and provides increased comfort during the procedure for the patient and clinician. 13 A prospective randomized trial comparing dexmedetomidine and midazolam for conscious sedation conducted by Elnabtity and Selim showed that dexmedetomidine was an effective analgesic alternative to midazolam during oocyte retrieval for in vitro fertilization. 14 Gupta et al. 15 noted that when dexmedetomidine was added to intravenous regional anesthesia, it provided a longer duration of analgesia than midazolam. In contrast, Kumari et al. 16 found that oral midazolam was superior to oral dexmedetomidine, with faster onset of sedation, a higher sedation score, and a lower anxiety score in children. Additionally, midazolam and dexmedetomidine showed no significant differences in reduction of brain activation in the auditory cortex. 17 Srivastava et al. 18 found that dexmedetomidine was safe and equally effective for sedation of mechanically ventilated neurosurgical patients compared with midazolam. However, a comparison of the effects of dexmedetomidine and midazolam in postoperative HICH patients had not been performed.
In this study, we compared the effects of dexmedetomidine and midazolam on sedation in HICH patients and found no difference in the time required to achieve a satisfactory sedative effect with a Ramsay sedation score of 2 to 4. However, the results also suggested that dexmedetomidine has a greater hemodynamic impact on postoperative patients than midazolam. The MAP and HR decreased more significantly in the dexmedetomidine group than in the midazolam group, and the degree of decrease depended on the concentration of dexmedetomidine (data not shown). Dexmedetomidine is an effective α2 adrenergic receptor agonist, and its affinity for α2 adrenergic receptors is eight times higher than that of clonidine. Therefore, dexmedetomidine can lower blood pressure. However, midazolam has no such pharmacological mechanism. Bhana et al.19,20 found that this effect was induced by a reduction in plasma catecholamines, which further resulted in peripheral vasoconstriction and sympatholytic properties. Consistent with the study by Bhana et al., we found no clinically apparent respiratory depression during dexmedetomidine administration in postoperative patients. 19 The SpO2 also showed no apparent decrease.
Considering that many studies have noted that dexmedetomidine has neuroprotective effects, we examined the plasma expression of the S-100β and NSE proteins after dexmedetomidine administration.21,22 S-100β protein and NSE are confirmed markers of cerebral injury. 23 Consistent with our hypothesis, dexmedetomidine effectively reduced the S-100β and NSE protein levels in patients compared with midazolam, indicating that dexmedetomidine plays a more beneficial role in brain protection. The potential mechanism might be that dexmedetomidine reduces the release of inflammatory mediators and neuroendocrine hormones. 24 Zhang et al. 25 reported that dexmedetomidine improved the short-term outcome of lung tissues of rats with sepsis. However, until now, the effects of dexmedetomidine on the outcome of postoperative HICH patients were unknown.
In the present study, all patients were followed up for 6 months, and the good prognosis rate in the dexmedetomidine group (83.72%) was higher than that in the midazolam group (69.74%), suggesting that dexmedetomidine administration improved the outcome of postoperative HICH patients. However, this study is limited by its small sample size.
Conclusion
Our study shows that dexmedetomidine is more effective for sedation and is more beneficial for brain protection and the long-term outcome in postoperative HICH patients than midazolam.
Footnotes
Author contributions
L.S. conceived and designed the study. W.G. collected the data. S.Z. and X.L. analyzed the results. W.G. and L.S. drafted the manuscript. All authors participated in the discussion of results and reviewed the manuscript.
Data availability
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This work was supported by the Brain Clinic and Basic Research Team Program of the First People’s Hospital of Kunshan (KYC004). The funders had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.