
Abstract
Objective
To evaluate the effectiveness and safety of allogeneic tendons for functional reconstruction of severe hand injuries.
Methods
From August 2007 to July 2014, we performed functional reconstruction with tendon allografts for severe hand injuries affecting two or more tendons. At the final follow-up, we assessed total active motion (TAM); pincer pinch strength; grip strength; Disabilities of the Arm, Shoulder, and Hand (DASH) score; degree of satisfaction; and adhesion. We measured the white blood cell count, C-reactive protein concentration, erythrocyte sedimentation rate, total T-cell count, and CD4+T/CD8+T ratio to evaluate the immune response and check for infection.
Results
Ten patients received 26 allogeneic tendons to reconstruct hand function. The average follow-up period was 50.0 months (range, 24–82 months). The TAM was 126.4° (12°–253°), pincer pinch strength was 0.83 kg (0–4.5 kg), and grip strength was 13.69 kg (4–41.5 kg). The DASH score was 14.25 (3.3–30.8), and seven and three patients were satisfied and partially satisfied, respectively. One patient developed tendon adhesion. All immune and infectious parameters were within the reference range.
Conclusion
Functional reconstruction using allogeneic tendons for severe hand injuries with multiple tendon defects was effective and safe; however, more research is needed.
Introduction
Severe hand injuries more commonly occur in people who are involved in handicraft-intensive activities and result in both intense pain and surgical challenges. 1 Severe hand injuries often include bone fractures and damage to the tendons, skin, and other tissues. The optimal treatment for severe hand injuries involving tendon defects is autologous tendon transplantation 2 ; however, if patients do not want to sacrifice an autologous tendon or have multiple tendon defects, allogeneic tendon transplantation may be a good choice. Allogeneic tendon grafts have been used since 1967 and their efficacy has been proven, 3 but their application has not become widespread because of concerns regarding immunogenicity and other issues. With the development of modern medicine, allograft tendons have been widely used in cruciate ligament injuries, 4 acromioclavicular ligament injuries, 5 Achilles tendon injuries, 6 hand trauma, 7 , 8 and other injuries. However, few studies have focused on the efficacy and safety of allogeneic tendon grafts in severe hand injuries. Therefore, this study was performed to assess the efficacy and safety of allogeneic tendon grafts for the treatment of severe hand injuries with multiple tendon defects among patients in our hospital.
Patients and methods
This study was approved by our institutional review board, and informed consent was obtained from each participant. From August 2007 to July 2014, we used tendon allografts to repair severe hand injuries (Modified Hand Injury Severity Score 9 of >50) with two or more tendon defects. All patients also underwent postoperative follow-up.
The allogeneic tendons were off-the-shelf products in China. They were harvested and processed by a commercial company (the tissue bank of the Orthopedic Institute of the People’s Liberation Army in Beijing) according to strict guidelines and stored in a deep-freeze environment.
Before surgery, we confirmed that the patients had well-healed wounds, pliable skin and soft tissue, no sign of infection, and normal passive mobility of the hand or wrist joints. Before the operation, patients with two or more tendon defects who did not wish to donate their own tendons were selected to receive tendon allografts (determined by the patients after the risks and benefits of using tendon allografts had been described). The surgeries were performed by five of the authors (GH.W., T.M., SG.X., RG.X., and XZ.Z.). During surgery, the allogeneic tendon was reconstituted with room-temperature saline with gentamicin for 30 minutes before use in the recipient. The rest of the surgical procedure was the same as that for autogenic tendon transplantation, and appropriate tendon suture tension was ensured.
During application of the flexor tendon grafts, we ensured that the repaired finger appeared slightly more flexed than the normal cascade after repair and that the finger could be straightened freely during wrist flexion. During extensor tendon repair, the digit and the wrist were straightened, with finger flexion permitted during wrist dorsal flexion.
Postoperative care
In extensor tendon graft repair, the wrist joint was dorsiflexed approximately 30°, and the metacarpophalangeal (MCP) joint was held straight with a volar splint. In flexor tendon graft repair, the wrist and MCP joints were flexed approximately 30°, and the finger joint was slightly flexed with a dorsal splint. If flexor and extensor tendons were repaired at the same time, the wrist was fixed in the neutral position.
After application of the tendon graft, the surgeon, patient, and rehabilitation physician cooperated regularly to ensure the best outcome. We encouraged the patients to perform a limited range of passive motion 3 to 5 days after surgery. After 3 weeks, full range of passive motion and limited range of active motion were permitted. Full range of active motion began after 6 weeks.
Outcome assessment
The total active motion (TAM) system 10 and the Disabilities of the Arm, Shoulder, and Hand (DASH) questionnaire scores were used to evaluate the functional outcomes. Because the motion of the MCP, proximal interphalangeal, and distal interphalangeal joints may have been affected in our series, the active motions of the three joints were measured using a goniometer for each injured finger. The TAM outcome uses the sum of the MCP, proximal interphalangeal, and distal interphalangeal joint flexions (in the attempted fist position) minus the extensor lag at these joints (in the thumb, TAM is the sum of MCP and interphalangeal joint flexion minus the extensor lag at these joints). The DASH scores were scaled from 0 to 100, with 0 reflecting no disability (good function) and 100 reflecting the worst function. Tendon adhesion was evaluated at the same time.
Two authors (YL.C. and YX.Z.) also measured the grip strength of the injured hand and the pincer pinch strength of the injured finger (a Jamar dynamometer was used to measure grip strength, and a hydraulic pinch gauge was used to measure pincer pinch strength; Sammons Preston Rolyan, Bolingbrook, IL, USA). The pincer pinch strength is determined by measuring the clamping force of the thumb with other injured fingers separately. During measurement of the pinch strength, the patient sat with the elbow flexed at 90° and the forearm in neutral rotation. The strength was measured three times, and the average value was recorded. The white blood cell (WBC) count, C-reactive protein (CRP) concentration, erythrocyte sedimentation rate (ESR), total T-cell count, and CD4+ T/CD8+ T ratio 11 were measured to evaluate the immune response and check for infection. Finally, the patients were asked about their degree of satisfaction with the functional recovery of the tendon allografts (satisfied, partially satisfied, or unsatisfied).
Results
Twenty-six allogeneic tendons were used to reconstruct the hand function in 10 patients (3 women, 7 men). Their mean age was 38.0 years (range, 18–60 years) at the time of surgery. The injuries had been caused by industrial accidents in nine patients and a utility knife in one patient. The injury types were flexor tendon rupture with a defect in six patients, extensor tendon rupture with a defect in three patients, and both flexor and extensor tendon ruptures with defects in one patient. In addition to the partial tendon defects, all patients also had soft tissue or bone injuries. Additional patient details are presented in Table 1.
Data for the 10 evaluated patients.
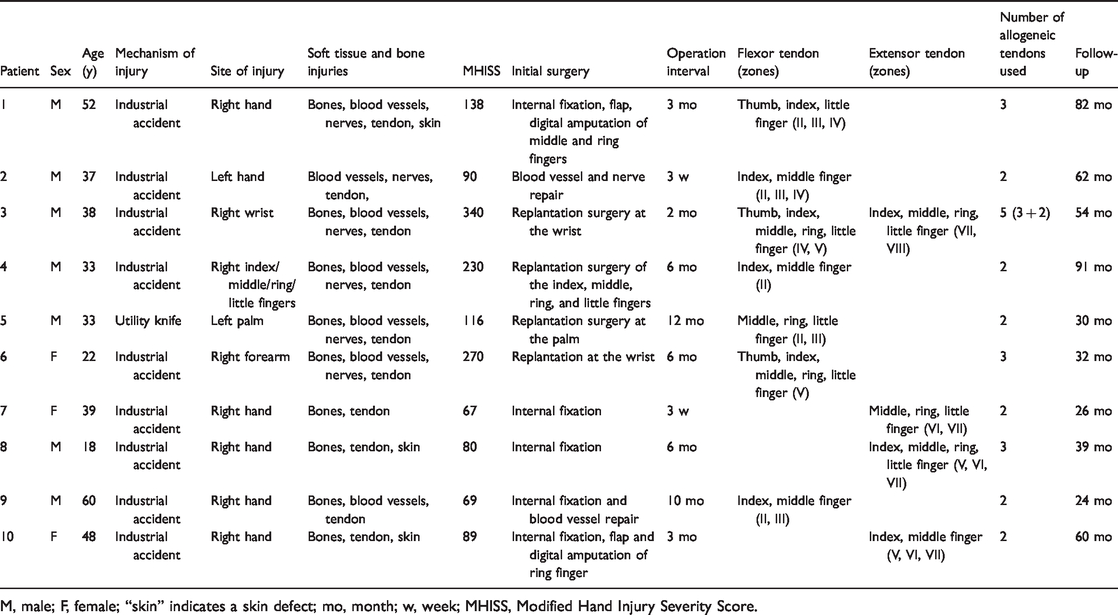
M, male; F, female; “skin” indicates a skin defect; mo, month; w, week; MHISS, Modified Hand Injury Severity Score.
The average follow-up period was 50.0 months (range, 24–82 months), and the wounds were well healed. No deep infection, infectious disease transmission, or obvious immune rejection was observed in this series. The mean TAM was 126.4° (range, 12°–253°), the mean pincer pinch strength was 0.83 kg (range, 0–4.5 kg) (n = 22), the mean grip strength was 13.69 kg (range, 4–41.5 kg) (n = 8), and the DASH score was 14.25 (range, 3.3–30.8). Seven and three patients were satisfied and partially satisfied with the results, respectively. One patient developed tendon adhesion and underwent tendon release surgery with flap shaping 3 months after the tendon graft procedure (Table 2). Six patients underwent immune-related blood tests, which showed that immunity-related parameters (WBC count, CRP concentration, ESR, total T-cell count, and CD4+ T/CD8+ T ratio) were mostly within the reference range (Table 3).
Outcome assessment of function.
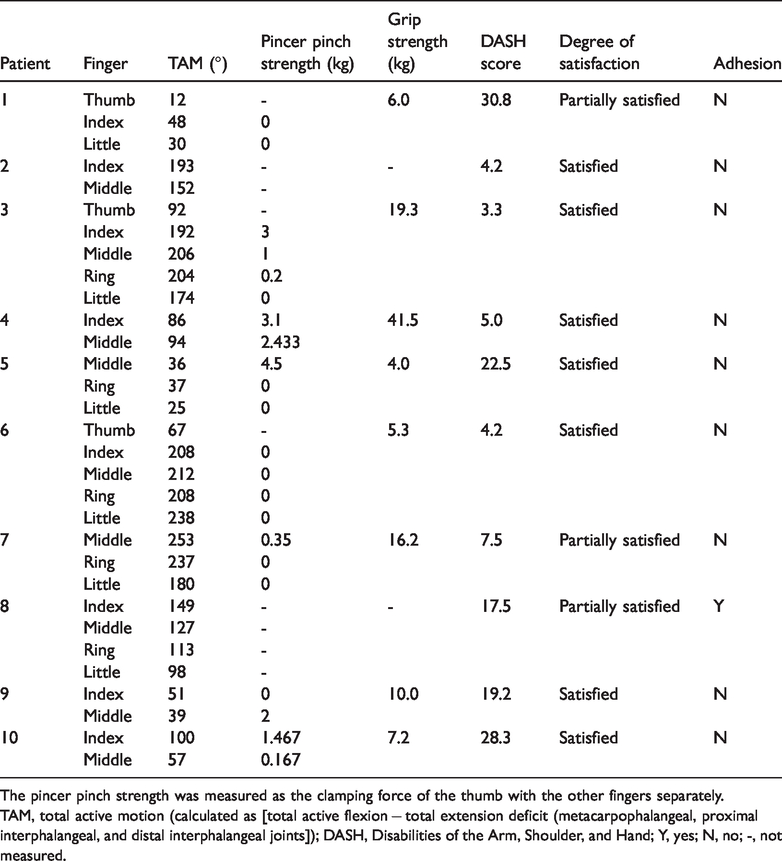
The pincer pinch strength was measured as the clamping force of the thumb with the other fingers separately.
TAM, total active motion (calculated as [total active flexion − total extension deficit (metacarpophalangeal, proximal interphalangeal, and distal interphalangeal joints]); DASH, Disabilities of the Arm, Shoulder, and Hand; Y, yes; N, no; -, not measured.
Outcome assessment of blood test results.

WBC, white blood cell; CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; –, not measured.
Discussion
The treatment process for severe hand injuries is complex. Several surgeries may be required to recover hand function. Before tendon grafting, surgical procedures such as internal fixation and repair of vessels, nerves, or wounds may be performed. After the initial surgery, infection must be prevented. One patient in our series developed an infection, and we performed functional reconstruction after treating this condition. Functional reconstruction is generally performed 3 months after the wound has healed.
Patients with severe hand injury may have several tendon defects requiring reconstruction with tendon grafts. 7 The use of allogeneic tendons for reconstruction was determined by the patients in this study. Some patients may prefer allogeneic tendon grafts because of concerns regarding decreased functioning after sacrificing the tendon. The use of allogeneic tendons can quickly restore the continuity of tendon defects without the restriction of tendon number that limits the use of autologous tendons. However, tendon allografts have some disadvantages. 12
Tendon allografts are associated with risks of rejection and disease transmission, which have prevented their widespread use. However, with advances in tissue processing, including acellularization and extensive donor screening for transmissible diseases, we can now better address the reconstructive needs of patients with allogeneic tendons for multiple tendon defects. We used allograft tendons provided by a professional tissue transplant library and used γ-irradiation sterilization treatment, which mostly eliminates disease spread. Before the allograft tendon was implanted into the recipient, it was placed in saline with gentamicin for 30 minutes. We observed no signs of infectious disease transmission in our study. Tang et al. 13 reported no infectious disease transmission, deep infection, or obvious immune rejection in 24 patients who received tendon allografts. Similarly, Harner et al. 14 also reported no evidence of immune reactions or disease transmission throughout 3 to 5 years of follow-up. In the present study, the CD4+ T/CD8+ T ratio, which is considered to be related to the immune status in tendons, 11 was normal. The levels of other immune markers such as the WBC count, CRP concentration, and ESR were mostly within the reference ranges in the six patients who underwent this testing. Therefore, we believe that the use of allogeneic tendons is safe. DeGeorge et al. 15 and Drake et al. 1 also expressed optimism about the application of allogeneic tendon grafts.
Even with optimum surgical treatment and physical therapy, postoperative adhesion formation, especially in allografts, is a fundamental problem that remains challenging for hand surgeons, 16 therapists, and patients. In our series, one patient developed tendon adhesion for which tendon release surgery with flap shaping was performed after 3 months, and the patient was partially satisfied with the final hand function. Therefore, effective postoperative rehabilitation exercises to prevent adhesion are extremely important. Although we have always stressed the importance of rehabilitation exercises to patients, some patients find it difficult to perform these exercises after discharge from the hospital.
Before deciding to transfer a tendon, we must ensure that the tissue condition permits the procedure and that the finger joints are not stiff. Severe hand injury is often accompanied by multiple tissue injuries. Therefore, tendon transfer is usually performed in a two-stage procedure, 16 , 17 with separate consideration for the recovery of soft tissue coverage. In severe hand injuries, tendon grafts are usually applied 3 months after covering the skin defect. 17 Patients should also perform exercises to avoid joint stiffness. In the present study, we performed surgeries 3.5 months after wound healing and instructed the patients to perform exercises before surgery.
Because the goal of the surgery was to restore the overall hand function, we did not separately evaluate the outcomes of the flexor and extensor tendon reconstruction. We hoped that the patients would be able to flex and extend their fingers freely. In our series, the DASH score was 14.25 (range, 3.3–30.8), suggesting that tendon allografts can restore the patient’s hand function to some extent. Of course, many factors affect the functional recovery of patients with severe hand injuries. Some patients in our study had experienced serious injuries and required multiple operations. For example, one patient underwent internal fixation for phalangeal and metacarpal fractures, amputation of the middle and ring fingers at the distal interphalangeal joint level, and anterolateral thigh flap repair of the wound in the first stage. The allogeneic tendon was transplanted in the second stage. Finally, because of serious injury, the functional recovery may not be ideal. In addition, patients with poor postoperative compliance and unwillingness to exercise will also experience difficulty in obtaining good function. Clinicians should fully understand the strengths and weaknesses of tendon allografts before use. It is very important to be aware of the indications. If a patient has a severe injury or is unable to cooperate after surgery, this method should be used with caution. Patients undergoing allogeneic tendon repair require regular follow-up visits and timely and effective functional exercise.
The main strength of this study is that few similar studies have evaluated the long-term function of allogeneic tendons in severe hand injuries. One limitation of this study is the small sample size and incomplete patient participation. Another limitation is the lack of comparison with similar surgeries. Future studies comparing allogeneic and autogenic tendons may provide additional useful information.
The results from this small sample indicate that in severe hand injuries with multiple tendon defects, functional reconstruction of the flexor and extensor tendons using allogeneic tendons was safe and effective; however, more research is needed.
Footnotes
Acknowledgment
Drs. Yi Feng Gao and Xing Wang helped to review the patient data in this paper.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This work was supported by the Key Research and Development Projects of Jiangsu Province (No. BE 2017681) and the Gusu Key Medical Talents Foundation of Suzhou (No. 20015).