
Abstract
Objective
Sirolimus has been used to treat paediatric kaposiform haemangioendothelioma patients. However, there is considerable pharmacokinetic variability among individuals, and it is difficult to develop an initial dosing regimen. The goal of the present study is to recommend an initial sirolimus dose in paediatric kaposiform haemangioendothelioma patients based on population pharmacokinetics and pharmacogenomics.
Methods
This was a retrospective clinical study. A population pharmacokinetics model was established and population characteristics, laboratory test results, drug combinations, and pharmacogenomics were considered as potential covariates. The Monte Carlo method was used to simulate the optimal initial dosage.
Results
The final covariates that affect sirolimus clearance include weight and the CYP3A5 genotype. The initial dosage of sirolimus for individuals with CYP3A5*3/*3 was 0.20 mg/kg split into two doses for 5 to 60 kg body weight. For individuals with CYP3A5*1, the initial dose was 0.23 mg/kg split into two doses for 5 to 30 kg body weight and 0.20 mg/kg split into two doses for 30 to 60 kg body weight.
Conclusion
The recommendation for the initial sirolimus dose in paediatric kaposiform haemangioendothelioma patients was based on population pharmacokinetics and pharmacogenomics. This study may provide practical value for sirolimus clinical use in paediatric kaposiform haemangioendothelioma patients.
Keywords
Introduction
Sirolimus is a macrolide compound that is produced by Streptomyces hygroscopicus, and it was has mainly been used as an anti-rejection medication after solid organ transplantation.1–5 Recently, sirolimus has been used to treat paediatric kaposiform hemangioendothelioma.6–10 However, with considerable pharmacokinetic variability in different individuals, it is difficult to develop an initial dosing regimen.11,12 We previously built a sirolimus population pharmacokinetic model without pharmacogenomics and, unfortunately, this model could not accurately recommend the initial sirolimus dose in paediatric kaposiform haemangioendothelioma patients. 13 That is mainly because sirolimus is metabolised by cytochrome P450 3A enzymes (CYP3A), which are located in the liver and gut mucosa.14–16 Additionally, sirolimus is also the substrate of P-glycoprotein, 17 which is encoded by the multidrug resistance 1 (MDR1 or ABCB1) gene. 18 Therefore, it is particularly important to explore the effect of these gene polymorphisms on the sirolimus clearance rate for dose recommendation. The goal of the present study was to recommend the initial sirolimus dose in paediatric kaposiform haemangioendothelioma patients based on population pharmacokinetics and pharmacogenomics.
Methods
Study design
This is a retrospective clinical study. Chinese paediatric kaposiform haemangioendothelioma patients who were treated with sirolimus from March 2016 to July 2019 at the Children’s Hospital of Fudan University (Shanghai, China) were enrolled. Population characteristics, laboratory test results, and drug combinations were collected from medical reports and therapeutic drug monitoring. Partial basic clinical information data from some patients were collected in a previous study. 13 The rest of the discarded blood samples from therapeutic drug monitoring were stored and used for the pharmacogenomics analysis. The study was retrospective, and blood samples for the pharmacogenomics analysis were leftover or discarded specimens from therapeutic drug monitoring. The analysis was approved by the ethics committee at our hospital without the need for written informed consent. The present study was approved by the Research Ethics Committee at the Children’s Hospital of Fudan University (Ethical code: [2019] 019; Shanghai, China; 27 February 2019).
Sirolimus administration
Sirolimus was orally administered and the dose range was 0.16 to 1.5 mg/day. Sirolimus dose adjustment was based on efficacy, adverse effects, and the therapeutic drug monitoring concentration. All blood concentrations were collected before the subsequent administration and, therefore, these concentrations used in the present study were trough concentrations. Sirolimus concentrations were tested using the Emit 2000 Sirolimus Assay (Siemens Healthcare Diagnostics Inc., Newark, NJ, USA) with a linear response range of 3.5 to 30 ng/ml.
Pharmacogenomics detection
Pharmacogenomics analysis was performed by Admera Health (Suzhou, China) using PGxOne® 160 with the Illumina X10 Sequencing System (Illumina Inc., San Diego, CA, USA). STATA computer software (version 12.0, StataCorp LP, College Station, TX, USA) was used to test the Hardy–Weinberg equilibrium, and P<0.05 was considered to be statistically significant.
Population pharmacokinetics model
The non-linear mixed-effects modelling software (NONMEM, edition 7, ICON Development Solutions, Ellicott, MD, USA) was used to develop population pharmacokinetic model. The pharmacokinetic parameters included apparent oral clearance (CL/F, where CL is clearance and F is bioavailability), volume of distribution (V/F, where V is the volume of distribution and F is bioavailability), and the absorption rate constant (Ka), which was fixed at 0.485/hour. 13
Equation (i) shows the inter-individual variability, as follows:

Equation (ii) shows the random residual variability, as follows:

Covariate model
Equation (iii) shows the relationship between weight and pharmacokinetic parameters, as follows:

Equations (iv) and (v) showed continuous covariates and categorical covariates, respectively, as follows:


The potential covariates included gender, age, weight, albumin, alanine transaminase, aspartate transaminase, creatinine, urea, total protein, total bile acid, direct bilirubin, total bilirubin, haematocrit, haemoglobin, co-medications (phenobarbitone and omeprazole), and pharmacogenetics. Objective function value (OFV) changes were identified using covariate inclusion, and a decrease in OFV >3.84 (P<0.05) and an increase in OFV >6.64 (P<0.01) were considered to be sufficient for significance in the final model.21,22
Model evaluation
The results of bootstrapping with 1000 repetitions with different random sampling, medians, and 2.5th to 97.5th percentiles, were used to evaluate the final model pharmacokinetic parameters. Goodness-of-fit plots and prediction-corrected visual predictive check plots were used to evaluate the final model. 23
Simulation
The simulation was made up of the following two parts: (I) individuals who carry the CYP3A5*3/*3 allele; and (II) individuals who carry the CYP3A5*1 allele. Seven weight groups (5, 10, 20, 30, 40, 50, and 60 kg) were simulated using 1000 virtual patients with different initial dosages. Based on previously published reports, the sirolimus target concentration in paediatric kaposiform haemangioendothelioma patients was fixed at 10 to 15 ng/ml.24,25
Results
Patients’ data
There were 14 patients enrolled in the study, with an average age of 1.53 ± 1.40 years. Nine patients were male and five were female. Other demographic information on the patients and drug combinations are shown in Table 1. Partial basic clinical information from some patients that were collected in a previous study 13 and the pharmacogenetics analysis and Hardy–Weinberg equilibrium are shown in Table 2. Table 2 also shows the Pearson chi-squared test result of each gene was >0.05, which meets the Hardy–Weinberg equilibrium.
Demographic data of patients and drug combinations.
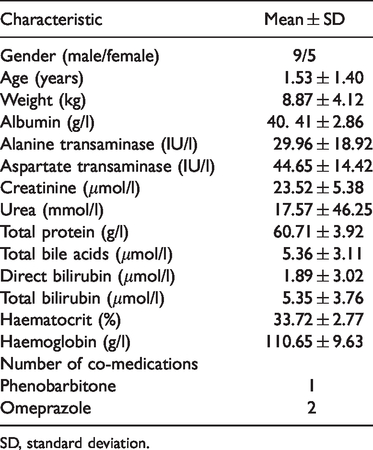
SD, standard deviation.
Pharmacogenetics analysis and Hardy–Weinberg equilibrium.
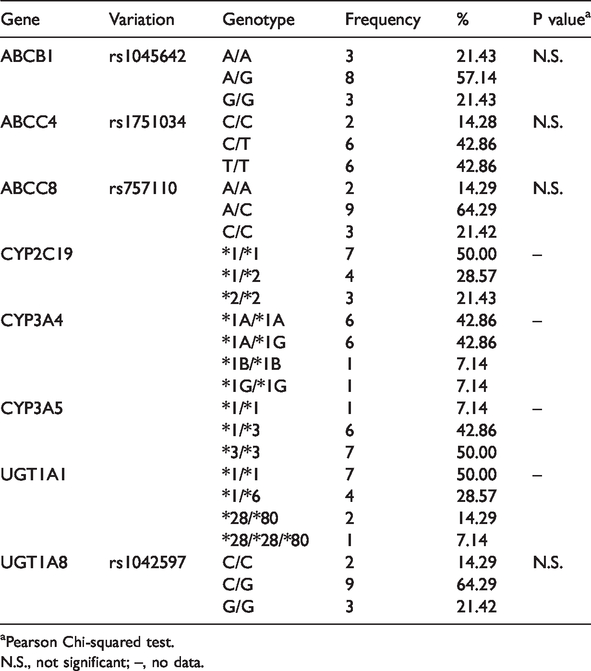
aPearson Chi-squared test.
N.S., not significant; –, no data.
Modelling and validation
The final model was as follows:


Figure 1 shows the goodness-of-fit plots for the final population model (goodness-of-fit plots for the base population model are shown in Supplementary Figure 1S), and Figure 2 showed the visual predictive check plots for the final model, indicating the predictive power of the final model. As shown in Table 3, the median values from bootstrapping were similar to the values estimated in the final model, and the absolute value of all the bias was <12%, showing that the final model was dependable.

Goodness-of-fit plots of the final population model.

Prediction-corrected visual predictive check for the final model.
Parameter estimates of the final model and bootstrap validation.

The 95% confidence interval was displayed as the 2.5th, 97.5th percentile of the bootstrap estimates.
CL/F, apparent oral clearance (L/hour); V/F, apparent volume of distribution (L); Ka, absorption rate constant (hour−1); θCYP3A5, the coefficient of CYP3A5 genotype; ωCL/F, inter-individual variability of CL/F; σ1, residual variability, proportional error; Bias, prediction error, Bias = (Median−Estimate)/Estimate×100%; –, no data.
Simulation
As shown in Figure 3, with the same body weight, the sirolimus clearance rates in individuals with CYP3A5*3/*3 and CYP3A5*1 were 1:1.999, and with the same CYP3A5 genotype, low body-weight individuals had a higher sirolimus clearance rate than those with a high body weight. In Figure 4, the 95% confidence interval of the simulation from an initial dose of 0.20 mg/kg that was split into two doses was between nearly 10 and 15 ng/ml of the target concentrations in CYP3A5*3/*3 individuals. As shown in Figure 5, in individuals with CYP3A5*1, for a weight of 5 to 30 kg, the initial dose of 0.23 mg/kg was split into two doses, which obtained the optimal probability to achieve the target concentrations. For a body weight of 30 to 60 kg, 0.20 mg/kg was split into two doses to obtain the optimal probability to achieve the target concentrations.

CL/F of sirolimus in paediatric kaposiform haemangioendothelioma patients.

Initial dose recommendation for sirolimus in paediatric kaposiform haemangioendothelioma patients with CYP3A5*3/*3.

Initial dose recommendation for sirolimus in paediatric kaposiform haemangioendothelioma patients with CYP3A5*1.
Discussion
The incidence of kaposiform haemangioendothelioma, a rare kind of vascular tumour, is estimated to be 0.07/100,000 children per year. 26 It is associated with some life-threatening complications such as airway obstruction, severe infection, and characteristic consumptive coagulopathy, as well as Kasabach–Merritt phenomenon.26,27 Thus, a treatment for kaposiform haemangioendothelioma is required.
Fortunately, sirolimus, the prototypical inhibitor of the mammalian target of rapamycin (mTOR), plays an important role in conditions involving disorders of the mTOR cell signalling pathway, 28 and it also has substantial antitumor activity. 29 For example, sirolimus has been administered to patients after liver transplant, 5 kidney transplant, 30 heart transplant,1,31 lung transplant, 4 hematopoietic stem cell transplant,2,3 neurofibromatosis type 1, 32 tuberous sclerosis complex, 33 and others.6–10,13 Sirolimus has also been widely used to treat paediatric kaposiform haemangioendothelioma. However, with considerable pharmacokinetic variability in between individuals, it is difficult to determine an initial dosing regimen in paediatric kaposiform haemangioendothelioma patients. Thus, the present study aimed to recommend the initial dose of sirolimus in paediatric kaposiform haemangioendothelioma patients based on population pharmacokinetics and pharmacogenomics.
In our study, we found the final covariates that affect sirolimus clearance, which were weight and the CYP3A5 genotype. The sirolimus clearance rates in individuals with CYP3A5*3/*3 or CYP3A5*1 were 1:1.999 at the same body weight. Additionally, in patients with the same genotype CYP3A5, patients with a low body weight had a higher sirolimus clearance rate than those with a high body weight, meaning that children with a lighter weight need larger doses than heavier children. We also simulated different initial dosing regimens in different body weights and CYP3A5 genotypes, and the sirolimus target concentrations were fixed to 10 to 15 ng/ml, in accordance with previous publications.24,25 In individuals with CYP3A5*3/*3, the initial dose recommendation for sirolimus, 0.20 mg/kg split into two doses, was for a body weight of 5 to 60 kg and the 95% confidence interval of the simulated sirolimus concentrations was between almost 10 and 15 ng/ml. Thus, the initial dose recommendation for sirolimus in paediatric kaposiform haemangioendothelioma patients with CYP3A5*3/*3 was 0.20 mg/kg split into two doses. The same initial dose (0.20 mg/kg split into two doses) for individuals with CYP3A5*1 who weighted 30 to 60 kg, can obtain the optimal target concentrations within the treatment window. Patients who carry CYP3A5*1 with a weight of 5 to 30 kg need a larger dose, and based on the simulation, we recommend 0.23 mg/kg split into two doses. Additionally, the probability of achieving the target concentrations from the recommended initial dosing regimens (0.23 mg/kg split into two doses for a body weight of 5 to 30 kg and 0.20 mg/kg split into two doses for a body weight of 30 to 60 kg) in individuals with CYP3A5*1 were all above 80%.
As a retrospective clinical study, this study has some limitations. Because of the low incidence of the paediatric kaposiform haemangioendothelioma in children, collecting patient data was extremely difficult, which was why there was a small number of patients in this study. Additionally, the present study had a poor fit and large confidence intervals, which may be because our modelling data came from a real-world dataset with a sparse sampling schedule, and it may not be sufficiently intensive. Therefore, a large-scale, prospective, intensive sampling-point study is needed to verify our results in the future.
In conclusion, these are the first recommendations for the initial sirolimus dose in paediatric kaposiform haemangioendothelioma patients based on population pharmacokinetics and pharmacogenomics. The present study may provide practical value for sirolimus clinical use in paediatric kaposiform haemangioendothelioma patients.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This work was funded by the Scientific Research Project of Science and Technology Commission of Shanghai Municipality (grant no. 18DZ1910604/19DZ1910703), the Shanghai Science and Technology Commission (grant no. 19XD1400900), and the China Scholarship Council (grant no. 201906100164).