
Abstract
Objective
This study aimed to determine the role of uterine artery blood flow (UABF) in recurrent spontaneous abortion (RSA) and to determine a viable option to promote the outcome of pregnancy.
Methods
A total of 421 women were prospectively recruited for this research. UABF indices, including the systolic/diastolic ratio, pulsatility index and resistance index, during the midluteal phase were compared between patients with RSA and women without RSA (controls). After low-molecular-weight heparin (LMWH) was administered to patients with RSA, indices at 7, 10, and 12 weeks of gestation were compared between the two groups.
Results
UABF indices during the midluteal phase were significantly higher in the RSA group than in the control group. After LMWH was administered to the RSA group, UABF indices in the first trimester were similar to those in the control group. The rate of spontaneous miscarriage was also similar between the groups after LMWH treatment.
Conclusions
Our study shows that sufficient uterine perfusion is crucial for a successful pregnancy. LMWH reduces the rate of spontaneous miscarriage in patients with RSA to a similar rate in women without RSA. LMWH might play a role in decreasing UABF resistance and increasing uterine perfusion.
Keywords
Introduction
Recurrent spontaneous abortion (RSA) is defined as at least two consecutive pregnancy losses before 20 weeks’ gestation, and is one of the most common clinical diseases in women. 1 There are many complex reasons for RSA, including chromosomal anomalies, 2 genital malformations, 3 thrombophilic disorders, 4 and immune dysfunction. 5 Nevertheless, approximately 50% of the reason for RSA occurring remains unknown.6,7 Generally, women with a history of repeated spontaneous miscarriages are under a large amount of stress. Therefore, the potential reasons of recurrent miscarriage need to be investigated and a feasible therapy needs to be determined.
The uterine artery is the main blood vessel that supplies the uterus. As a non-invasive technology, color Doppler of uterine artery blood flow can be performed to evaluate uterine perfusion.8,9 Uterine artery blood flow indices, including the systolic/diastolic ratio (S/D), pulsatility index (PI), and resistance index (RI), reflect the situation of uterine blood perfusion, which further affects uterine receptivity.9,10 These blood flow indices gradually decrease during the natural menstrual cycle and reach the lowest values in the middle stage of corpus luteum. Uterine artery perfusion increases accordingly to meet the need of embryo implantation.10–12 Uterine artery perfusion is important for endometrial receptivity, which plays a major role in successful implantation. 8 Impedance to uterine artery blood flow is different between infertile women and women with normal fertility. 13 However, there have been few studies on uterine perfusion of women with RSA with or without pregnancy. Moreover, these studies reached conflicting conclusions.14–16
Low-molecular-weight heparin (LMWH) is a type of anticoagulant. LMWH is composed of 12 to 18 sugar units with a relative molecular weight between 4000 and 5000 D. LMWH is produced by enzymatic or chemical depolymerization from unfractionated heparin, which can prevent thrombosis by enhancing antithrombin III and inhabiting activated factor X. Heparin does not affect platelet aggregation and the combination of fibrinogen and platelets. 17
The present prospective study aimed to compare uterine artery blood flow during the midluteal phase between women with RSA and women without RSA, and confirm the role of sufficient uterine perfusion in the success of pregnancy. We also aimed to examine the effect of LMWH on uterine artery blood flow and the outcome of pregnancy in patients with RSA.
Materials and methods
Patients
Women who attended the Reproductive Medicine Clinic of Ningbo First Hospital between January 2017 and December 2018 were prospectively recruited for this study (Figure 1). Among these women, those with a history of more than two times of consecutive spontaneous abortions were enrolled in the RSA group. Additionally, women without a history of miscarriage were recruited for controls. All subjects with genetic anomalies, anatomical abnormalities, thrombophilia, immune disorders, and chronic diseases or ongoing treatments, especially hormonal treatments or antithrombotic drugs during the past 3 months before entry into the study, were excluded from the study.

Flowchart of the study procedure. RSA, recurrent spontaneous abortion; UABF, uterine artery blood flow; S/D, systolic/diastolic ratio; PI, pulsatility index; RI, resistance index; LMWH, low-molecular-weight heparin.
The study protocol was approved by the Institutional Review Board of Ningbo First Hospital (No. 2017-R029). All methods were performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants who were included in the study.
Design of the study
Uterine artery blood flow Doppler waves were analyzed and categorized as abnormal Doppler waves (Figure 2b) if there was reverse or an absence of diastolic blood flow. 18 The proportion of abnormal Doppler waves during the midluteal phase was compared between the RSA and control groups (Figure 1). Uterine artery blood flow indices, including the mean S/D, PI, and RI values, were compared between the two groups. Endometrial thickness was also compared between the groups.

Uterine artery blood flow Doppler waves. a, Abnormal uterine artery blood flow Doppler waves (reverse of diastolic blood flow). b, Normal uterine artery blood flow Doppler waves.
Seventy-nine women in the RSA group and seventy-four in the control group became pregnant between January 2017 and December 2018. All of these women received standard pregnancy surveillance. Luteal support was routinely performed until 12 weeks of gestation. This support consisted of 20 mg Duphaston daily (dydrogesterone tablets; Abbott, Amsterdam, The Netherlands). As routine prophylaxis for neural tube defects, all women were encouraged to take folic acid 800 μg daily, starting before conception and continuing until 12 weeks of gestation. A total of 4000 IU LMWH (Enoxaparine; Sanofi-aventis, Paris, France) was injected in the RSA group once daily in addition to standard luteal support after confirmation of pregnancy, and was continued until at least 12 weeks of gestation. 19 Ultrasonic assessments were performed at 7, 10, and 12 weeks of gestation. Uterine artery blood flow indices and crown-rump length (CRL) were compared between the two groups. By the end of 12 weeks of gestation, the proportion of spontaneous miscarriage was compared between the RSA and control groups.
Transvaginal sonography
An ultrasound examination of uterine artery blood flow was performed using a 2.9-MHz (range, 2–5 MHz) transvaginal microconvex probe (GE Voluson E8; GE Healthcare Austria GmbH & Co OG, Zipf, Austria). The examiners were blinded to the history of all subjects.
Ultrasonic Doppler assessment was performed during the midluteal phase at 7 to 10 days after women’s ovulation, which was confirmed by follicular monitoring through an ultrasound examination. Serum progesterone levels were measured during the midluteal phase with an electrochemiluminescence immunoassay (Beckman Coulter, Tokyo, Japan).
Statistical analysis
The data are shown as mean and standard deviation. The Student’s test was used for analyzing baseline differences between the groups, while Pearson’s chi-square test was used to compare ratios between the groups. P < 0.05 was considered statistically significant. The data were analyzed using SPSS for Windows (version 19.0; IBM Corp., Armonk, NY, USA).
Results
A total of 421 patients, including 132 in the RSA group and 289 in the control group, were prospectively recruited for this study (Figure 1). The mean age of women in the RSA group and control group was 29.55±3.83 years (range: 22–39 years) and 28.97±3.30 years (range: 21–42 years), respectively.
During the midluteal phase, 27 women in the RSA group and 18 women in the control group presented with abnormal Doppler waves (Figure 1). The proportion of abnormal Doppler waves was significantly higher in the RSA group than in the control group (P<0.001) (Table 1). This difference between the groups was also observed in normal uterine artery blood Doppler waves (Figure 2a). The mean S/D value for uterine arteries during the midluteal phase was significantly higher in the RSA group than in the control group (P = 0.011) (Table 2). The mean PI and RI values were also significantly higher in the RSA group than in the control group (P = 0.015, P = 0.031, respectively). Endometrial thickness during the midluteal phase in the RSA group was significantly thinner than that in the control group (P<0.001).
Comparison of the proportion of abnormal uterine artery blood flow Doppler waves and the rate of spontaneous miscarriage between the RSA and control groups.

RSA, recurrent spontaneous abortion.
Comparison of endometrial thickness and uterine artery blood flow indices between the RSA and control groups during the midluteal phase.
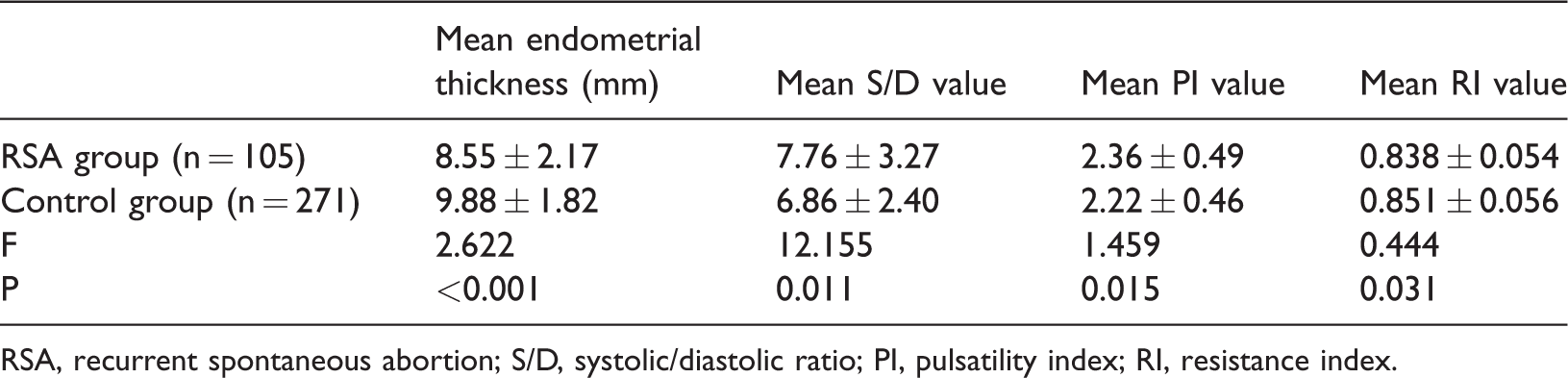
RSA, recurrent spontaneous abortion; S/D, systolic/diastolic ratio; PI, pulsatility index; RI, resistance index.
Among pregnant subjects, the proportion of abnormal uterine artery Doppler waves at 7 weeks of gestation was not different between the two groups (Table 1). The mean S/D, PI, and RI values for uterine arteries at 7 weeks of gestation were not significantly different between the two groups (Table 3). The same outcomes were observed at 10 and 12 weeks of gestation (Table 3). The mean CRL at 7, 10, and 12 weeks of gestation was not significantly different between the two groups (Table 3).
Comparison of the CRL and uterine artery blood flow indices between the RSA and control groups at 7, 10, and 12 weeks of gestation.

CRL, crown–rump length; RSA, recurrent spontaneous abortion; S/D, systolic/diastolic ratio; PI, pulsatility index; RI, resistance index.
Among the pregnant patients, 7.59% (6/79) in the RSA group and 8.11% (6/74) in the control group had spontaneous miscarriage, with no significant difference between the groups (Table 1).
Discussion
The present study showed that the proportion of abnormal uterine artery blood Doppler waves was higher in patients in the RSA group than in patients in the control group. Uterine artery blood flow indices during the midluteal phase, including the mean S/D, PI, and RI, were significantly higher in the RSA group than in the control group. This result indicates that women with recurrent spontaneous miscarriages have decreased uterine blood flow during the midluteal phase compared with those without miscarriage. Therefore, we conclude that uterine perfusion is an important factor that affects the success of implantation, which is consistent with previous studies.8,10 These findings are meaningful because we confirmed that sufficient uterine perfusion has a critical role in the success of pregnancy. Furthermore, we found that endometrial thickness during the midluteal phase in the RSA group was significantly thinner than that in the control group. This finding suggests that repeated spontaneous miscarriages cause direct damage to the endometrium of women.
After showing that uterine artery blood indices were related to the success of pregnancy, our next step was to determine a feasible therapy for improving uterine artery blood flow. In the present study, pregnant women with RSA were administered a daily dose of 4000 IU LMWH in addition to standard luteal support in accordance with previous reports. 19 We found that there were no significant differences in uterine artery blood flow indices between the RSA group and the control group at 7, 10, and 12 weeks of gestation. Furthermore, there was no difference in the spontaneous miscarriage rate between the two groups. The risk of spontaneous abortion is related to the patient’s previous reproductive history, which is an independent predictor of future pregnancy outcome.20,21 Regan et al. showed that the risk of spontaneous miscarriage increased after each successive pregnancy loss, reaching approximately 40% after three consecutive pregnancy losses. 21 In our study, the rate of spontaneous abortion in the RSA group declined to that in the control group after receiving LMWH treatment. Furthermore the CRL in the RSA group was similar to that in the control group from 7 to 12 weeks of gestation. Therefore, we speculate that LMWH plays an important role in improving the outcome of pregnancy.
In recent years, studies have shown that LMWH also promotes proliferation, invasion, and differentiation of trophoblast cells, inhibits apoptosis of trophoblast cells, protects the vascular endothelium, and promotes placental formation in addition to its anticoagulation effect.22,23 In our study, the finding of no differences in uterine artery blood flow indices between RSA and control groups in the first trimester suggested that uterine perfusion of patients with RSA after receiving LMWH treatment was greatly improved to the level of uterine perfusion in women without RSA. Our result is consistent with previous studies.24–27 Nevertheless, a multicenter, randomized, controlled trail performed by Abheiden et al. showed the opposite conclusion. 28 These authors showed that LMWH did not affect uterine arterial Doppler. These authors might have compared differences in the uterine artery between women who used LMWH combined with aspirin and women who used aspirin only at a single time-point in mid-pregnancy. However, we focused on the effect of LMWH on pregnant outcome in the first trimester. Furthermore, the participants in Abheiden et al.’s study 28 were women with inheritable thrombophilia, while our research subjects were patients with RSA for unknown reasons. In our study, using LMWH starting from confirmation of pregnancy could have reduced the abortion rate of patients with RSA. These data support the hypothesis that LMWH improves the outcome of pregnancy in patients with RSA by decreasing uterine artery blood flow resistance and increasing uterine perfusion.
The strengths of the present study are measurement of noninvasive Doppler ultrasound, the strict inclusion criteria, and the early start of treatment. In our study, we showed an association between uterine perfusion during the midluteal phase and spontaneous abortion. Doppler ultrasound measurement, as a noninvasive method, can be performed for screening the high-risk abortion population before pregnancy. This provides a time window for treatment of patients with RSA. Furthermore, to the best of our knowledge, we showed the effect of LMWH on uterine artery blood flow in the first trimester for the first time. Our results could have been more convincing if we had divided patients with RSA into two groups and no treatment was performed in one of the groups. However, designing a study providing no treatment to patients with RSA with a high risk of abortion is unethical, especially considering the current tense physician–patient relationship in our country.
In conclusion, we conclude that sufficient uterine perfusion plays a critical role in the success of pregnancy. Insufficient uterine artery perfusion may lead to implantation failure and early loss of pregnancy. For patients with unknown repeated spontaneous miscarriages, uterine arterial blood flow indices can be used to evaluate uterine perfusion. A reduction in uterine artery blood flow resistance might improve the outcome of pregnancy. LMWH could play a significant role in improving the outcome of pregnancy in patients with RSA, probably by reducing uterine arterial blood flow impendence and increasing uterine perfusion.
Footnotes
Acknowledgements
We thank Yunfei Lu for providing help in statistical analysis. We also thank Dr. Bo Xiong and Rozita Petri for providing assistance with grammar of the manuscript.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This work was supported by the Medical and Health Science and Technology Plan Project of Zhejiang Province (2018KY675) and the Natural Science Foundation of Ningbo (2016A610161).