
Abstract
Objective
To investigate the association between gamma-glutamyl transferase (GGT) and type 2 diabetes mellitus (T2DM) risk.
Methods
This was a secondary analysis based on a publicly available DRYAD dataset that included 15 444 study participants that received medical examinations at a single centre in Japan between 2004 and 2015. Crude, minimally-adjusted and fully-adjusted regression models were used to evaluate the relationship between GGT levels and T2DM risk.
Results
The study participants (mean ± SD age of 43.72 ± 8.90 years; 8415 of 15 444 [54.49%] were male) were followed-up for a median of 1968 days (5.39 years). After adjusting for potential covariates, a non-linear relationship between the baseline GGT level and T2DM incidence was observed. The inflection point for T2DM risk was 10 IU/l GGT; below this point, the T2DM incidence increased by 1.18-fold per unit change in GGT. Above this point, the association between GGT and the incidence rate of T2DM became nonsignificant.
Conclusion
Baseline GGT exhibited a non-linear association with T2DM incidence. Elevated GGT levels should be incorporated into routine screening for individuals at high risk of T2DM, allowing for early intervention targeting GGT to potentially reduce T2DM-related morbidity.
Introduction
Type 2 diabetes mellitus (T2DM) is a major public health problem and the incidence has been continually rising in recent years. 1 According to the Centers for Disease Control and Prevention in the US, approximately one out of every 10 adults currently has T2DM. 1 Advances in medical technology have led to the development of new therapeutic agents, but mortality associated with the complications of T2DM remains high. 2 It is estimated that about five million people died from T2DM in 2015 worldwide, which accounted for 12.8% of all-cause mortality in adults. 3 Therefore, identification of factors associated with the pathogenesis of T2DM is of great importance for improving screening of the high-risk population and facilitating early prevention strategies.
Gamma-glutamyl transferase (GGT) is a liver enzyme involved in the gamma glutamyl cycle, which is related to glutathione (GSH) synthesis and degradation. 4 Previous studies have demonstrated a close relationship between GGT, oxidative stress and insulin resistance, which are two critical pathophysiological processes contributing to T2DM.5–8 Despite extensive research focused on the potential relationship between GGT and the risk of T2DM, no consensus has been reached to date.9–11 Therefore, this current study used publicly available data from a longitudinal study conducted in Japan to further evaluate the role of GGT in T2DM.
Patients and methods
Data source and study population
This current study undertook a secondary analysis of open-access data from the DRYAD database (https://datadryad.org/). The raw data can be freely obtained from this website and reanalysed with rationalcitation (Dryad data package: Okamura et al. (2019) Data from: Ectopic fat obesity presents the greatest risk for incident type 2 diabetes: a population-based longitudinal study, Dryad, Dataset, https://doi.org/10.5061/dryad.8q0p192). 12 This secondary analysis was undertaken in the Department of Cardiology, Luoyang Central Hospital Affiliated to Zhengzhou University, Luoyang, Henan Province, China.
The original study involved a population-based prospective cohort recruited from a medical examination programme at Murakami Memorial Hospital, Gifu, Japan. 12 Data for 15 464 participants between 2004 and 2015 were extracted to explore the relationship between various obesity-related phenotypes and the risk of T2DM. Exclusion criteria were under-medication, alcoholic fatty liver disease, viral hepatitis, T2DM and fasting plasma glucose (FPG) ≥6.1 mmol/l. The original study was approved by the ethics committee of Murakami Memorial Hospital and written informed consent was obtained from all participants.
The database file downloaded from DRYAD contained information for the following parameters: age, sex, body mass index (BMI), waist circumference (WC), ethanol consumption, smoking status, exercise habit, fatty liver, and baseline levels of systolic blood pressure (SBP), diastolic blood pressure (DBP), alanine aminotransferase (ALT), aspartate aminotransferase (AST), triglycerides (TG), high-density lipoprotein cholesterol (HDL-C), FPG, glycosylated haemoglobin (HbA1c) and GGT. Regular exercise was defined as playing any type of sport more than once a week. T2DM was defined as HbA1c ≥6.5%, FPG ≥7 mmol/l or self-reported. 12 In the current study, the baseline GGT level was evaluated as an independent variable and the dependent variable was the risk of T2DM. The median follow-up time was 1968 days (5.39 years).
Statistical analyses
Statistical analyses were performed using EmpowerStats (http://www.empowerstats.com, X&Y Solutions Inc., Boston, MA, USA) and R packages (http://www.R-project.org). Continuous variables are shown as mean ± SD or median (interquartile range) according to data distribution. Categorical variables are presented as frequencies and percentages. Differences among groups (GGT tertiles) were detected using one-way analysis of variance (for normally distributed data), Kruskal–Wallis H tests (for skewed distribution), χ2-test analysis (for categorical variables) or Fisher’s exact test. Univariate and multivariate Cox regression analyses were conducted to evaluate the relationship between GGT levels and T2DM risk. According to the STROBE recommendation, results for all three adjusted models are presented. 13 In the crude model, there was no adjustment for additional variables; the minimally-adjusted model only adjusted for sex and age; and in the fully-adjusted model, confounding covariates that could alter the original effect size (hazard ratio) by >10% or with a P-value for the regression coefficient <0.1 were added to the model as confounders. 14 For sensitivity analysis, GGT was also converted into a categorical variable according to tertiles (low, median, high). A trend test was conducted by substituting the median GGT values of the three groups into the Cox proportional hazards regression equation as a continuous variable. The P-value for the regression coefficient of this continuous variable is the P-value for the trend. A potential non-linear relationship of GGT with the risk of T2DM was also evaluated using the Cox proportional hazards regression model with cubic spline functions.15,16 When a remarkable segmented trend was revealed, the inflection point was detected using the recursive algorithm, and a two-piecewise Cox proportional hazard model was applied to both sides of the inflection point. The log likelihood ratio test was employed to determine the most suitable model for describing the association between GGT and T2DM risk.15,16 A P-value < 0.05 (two-sided) was considered to be statistically significant.
Results
A total of 15 444 participants were included in the final analysis after excluding 20 participants with abnormal liver function, which was defined as ALT or AST > 120 U/l (i.e. three-times higher than the normal range). The mean ± SD age of the participants was 43.72 ± 8.90 years and more than half were male (8415 of 15 444; 54.49%). The baseline demographic and clinical characteristics of the study participants are summarized according to the tertiles of baseline GGT level (Table 1) in order to show the distribution of other confounding factors and, at the same time, to explore which variables might be associated with GGT levels. Compared with the other two tertile groups, participants in the high tertile for GGT were more likely to be male, older, ex/current smokers, alcohol drinkers and to have more risk factors for T2DM at baseline, including a higher rate of fatty liver and higher levels of BMI, WC, BP, TC, HDL-C, TG, HbA1c, as well as FPG. Accordingly, they were more susceptible to the development of T2DM later in life (250 of 5400; 4.63%); while, the T2DM incidence rates were only 0.82% (33 of 4009) and 1.46% (88 of 6035) in the low GGT and median GGT groups, respectively.
Baseline demographic and clinical characteristics of the study participants (n = 15 444) that were included in the final analysis of the relationship between gamma-glutamyl transferase (GGT) and type 2 diabetes mellitus (T2DM) risk.

Data presented as mean ± SD, median (interquartile range) or n of participants (%).
aP-value calculated by one-way analysis of variance for normally distributed continuous variables, χ2-test analysis for categorical variables or Fisher’s exact test for categorical variables with expected frequency < 10.
bP-value calculated by Kruskal–Wallis H Test (skewed distribution).
BMI, body mass index; WC, waist circumference; SBP, systolic blood pressure; DBP, diastolic blood pressure; ALT, alanine aminotransferase; AST, aspartate aminotransferase; TC, total cholesterol; HDL-C, high-density lipoprotein cholesterol; TG, triglycerides; FPG, fasting plasma glucose; HbA1c, glycosylated haemoglobin.
The baseline demographic and clinical characteristics between participants with and without T2DM are compared in Table 2. It could be seen that participants with male sex, aging, smoking and drinking, insufficient exercise and elevated levels of all metabolic parameters were at high risk of T2DM.
Comparison of baseline demographic and clinical characteristics between of the study participants (n = 15 444) that were included in the final analysis of the relationship between gamma-glutamyl transferase (GGT) and type 2 diabetes mellitus (T2DM) risk stratified according to whether or not they had T2DM.

Data presented as mean ± SD, median (interquartile range) or n of participants (%).
aP-value here was calculated by T-test for normally distributed continuous variables, χ2-test analysis for categorical variables or Fisher’s exact test for categorical variables with expected frequency < 10.
bP-value calculated by Kruskal–Wallis H Test (skewed distribution).
BMI, body mass index; WC, waist circumference; SBP, systolic blood pressure; DBP, diastolic blood pressure; ALT, alanine aminotransferase; AST, aspartate aminotransferase; TC, total cholesterol; HDL-C, high-density lipoprotein cholesterol; TG, triglycerides; FPG, fasting plasma glucose; HbA1c, glycosylated haemoglobin; NS, no significant between-group difference (P ≥ 0.05).
Three multivariate analysis models were constructed to detect the independent association of GGT with T2DM risk. As shown in Table 3, the GGT level, when calculated as a continuous variable, was positively associated with the incidence of T2DM in both the crude unadjusted model and the minimally-adjusted model (P < 0.0001 for both models), of which a one unit (IU/l) change would lead to a 1% increase in T2DM risk. When being converted as a categorical variable, the influence of GGT on T2DM risk became more pronounced. With the low tertile group as the reference, the T2DM risk increased to 2.24-fold and 6.53-fold in median and high tertile groups, respectively, in the crude unadjusted model (P < 0.0001 for trend); and were 1.97-fold and 5.23-fold after minimal adjustment for age and sex (P < 0.0001 for trend). However, this association became insignificant after the addition of other confounding covariates, including sex, age, ethanol consumption, fatty liver, BMI, baseline ALT, baseline AST, baseline TG, baseline HbA1c, baseline FPG and baseline SBP (median tertile versus low tertile: hazard ratio [HR] 1.08, 95% confidence interval [CI] 0.71, 1.66; high tertile versus low tertile: HR 1.40, 95% CI 0.90, 2.20; P = 0.0563 for trend).
Cox regression analyses of the association between glutamyl transferase (GGT) level and the risk of type 2 diabetes mellitus (T2DM) using three different models.

Multivariate models: crude model unadjusted model did not adjust for other covariates; minimally-adjusted model adjusted for age and sex; fully-adjusted model adjusted for age, sex, ethanol consumption, smoking status, fatty liver, body mass index, baseline alanine aminotransferase, baseline aspartate aminotransferase, baseline total cholesterol, baseline high-density lipoprotein cholesterol, baseline triglycerides, baseline glycosylated haemoglobin, baseline fasting plasma glucose and baseline systolic blood pressure.
HR, hazard ratio; CI, confidence interval; Ref, reference.
As shown in Figure 1, a non-linear relation between GGT and T2DM was identified after adjusting for age, sex, ethanol consumption, smoking status, fatty liver, BMI, ALT, AST, TC, HDL-C, TG, HbA1c, FPG and SBP (log likelihood ratio test, P < 0.001). The inflection point was determined to be 10 IU/l GGT. As shown in Table 4, every unit increase in GGT level would lead to a 1.18-fold increased risk of T2DM (95% CI 1.21, 3.94, P = 0.0095) when GGT was <10 IU/l. Saturation was reached at 10 IU/l (P = 0.1768).

Non-linear relationship between gamma-glutamyl transferase (GGT) and type 2 diabetes mellitus risk. A nonlinear relationship was detected after adjusting for age, sex, ethanol consumption, smoking status, fatty liver, body mass index, alanine aminotransferase, aspartate aminotransferase, total cholesterol, high-density lipoprotein cholesterol, triglycerides, glycosylated haemoglobin, fasting plasma glucose and systolic blood pressure.
The results of two-piecewise Cox proportional hazard model of the relationship between gamma-glutamyl transferase (GGT) and type 2 diabetes mellitus (T2DM) risk.
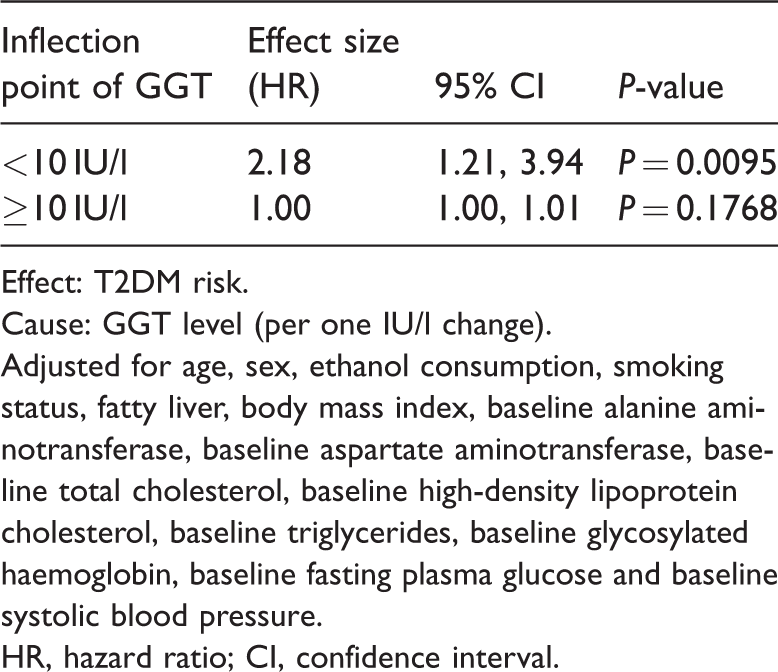
Effect: T2DM risk.
Cause: GGT level (per one IU/l change).
Adjusted for age, sex, ethanol consumption, smoking status, fatty liver, body mass index, baseline alanine aminotransferase, baseline aspartate aminotransferase, baseline total cholesterol, baseline high-density lipoprotein cholesterol, baseline triglycerides, baseline glycosylated haemoglobin, baseline fasting plasma glucose and baseline systolic blood pressure.
HR, hazard ratio; CI, confidence interval.
As the GGT level was affected by various physiological and demographic factors, which could be evidenced by the wide range of GGT levels in Table 1 and other similar studies, many studies have only focused on the association between GGT and T2DM within the normal range of GGT concentrations. Therefore, the current study also evaluated whether there was a non-linear relationship between GGT and T2DM among participants with normal GGT (set to 51 IU/l and 33 IU/l in males and females, respectively). 17 However, the results were consistent with the main analysis including all participants, confirming the non-linear relationship (Figure 2 and Table 5).

Non-linear relationship between gamma-glutamyl transferase (GGT) and type 2 diabetes mellitus risk among study participants exhibiting GGT levels within the normal range (set to 51 IU/l and 33 IU/l in males and females, respectively). 17 A similar nonlinear relationship was detected as observed for the entire study population after adjusting for age, sex, ethanol consumption, smoking status, fatty liver, body mass index, waist circumference, alanine aminotransferase, aspartate aminotransferase, total cholesterol, high-density lipoprotein cholesterol, triglycerides, glycosylated haemoglobin, fasting plasma glucose and systolic blood pressure.
The results of two-piecewise Cox proportional hazard model of the relationship between gamma-glutamyl transferase (GGT) and type 2 diabetes mellitus (T2DM) risk among study participants exhibiting GGT levels within the normal range (set to 51 IU/l and 33 IU/l in males and females, respectively). 17

Effect: T2DM risk.
Cause: GGT level (per one IU/l change).
Adjusted for age, sex, ethanol consumption, smoking status, fatty liver, body mass index, waist circumference, baseline alanine aminotransferase, baseline aspartate aminotransferase, baseline total cholesterol, baseline high-density lipoprotein cholesterol, baseline triglycerides, baseline glycosylated haemoglobin, baseline fasting plasma glucose and baseline systolic blood pressure.
HR, hazard ratio; CI, confidence interval.
The influence of other factors, including sex, age, smoking and drinking habits, BMI, TC, TG, HDL-C, as well as FPG, on the relationship between GGT and DM risk were also explored, but no significant interactions were observed (supplemental data: Table S1).
Discussion
This current secondary analysis demonstrated a non-linear relationship between GGT level and T2DM risk. The level of GGT was positively associated with T2DM risk when GGT was less than 10 IU/l. The relationship became insignificant when GGT values exceeded this threshold.
Gamma-glutamyl transferase is a highly glycosylated membrane protein, which is located on the surface of the plasma membrane of almost all cells except erythrocytes. 18 It is encoded by a gene located on chromosome 22 and a total of 13 homologues have been identified on the human GGT gene. 19 Transcription of the various mRNA subtypes depends upon the cell type and stimulating agent. 20 Little is known about the complex and precise regulation of GGT gene expression. The highest level of activity of GGT is in the kidney, being about 10-times of that of the liver, but serum GGT is mainly derived from hepatocyte microsomes and the epithelial cells of the bile capillaries. 21 GGT consists of two subunits: a 50–62 kDa large chain and a 22–30 kDa smaller chain.22,23 The large subunit comprises of an intracellular N-terminal sequence, a transmembrane hydrophobic domain and an extracellular domain.22,23 It is mainly responsible for the anchorage of GGT in the plasma membrane.22,23 The active catalytic centre is located on the small subunit. 24 The primary physiological function of GGT is the catalysis of GSH hydrolysis, transcellular transport and absorption of amino acids, as well as the degradation of toxicants. 25 Elevated serum GGT level have been shown to be associated with hepatobiliary diseases (inflammatory, damage and obstruction), metabolic diseases (acute myocardial infarction, hypertension, diabetes mellitus and stroke) and even tumours (ovarian cancer, gastric cancer and colorectal cancer).26–34
The current secondary analysis demonstrated a significant association between GGT level and T2DM risk, independent of age, sex, ethanol consumption, smoking status, fatty liver, BMI, ALT, AST, TC, HDL-C, TG, HbA1c, FPG and SBP, which might be explained by the following mechanisms. First, in our opinion, GGT is not only a sensitive indicator of an enhanced oxidative stress state, but it is also a direct contributor to oxidative stress. The gamma glutamyl cycle, mediated by GGT, is the most important endogenous antioxidant system. 35 Oxidative stress caused by alcohol abuse, high glucose exposure or some other stimuli could activate multiple signal cascades, including Ras, P38 mitogen-activated protein kinases, protein kinase C ζ, extracellular signal-regulated protein kinases 1 and 2, phosphatidylinositol 3-kinase, Akt, protein kinase C δ and protein kinase A, which promotes the expression of GGT. 19 In turn, the cysteinyl-glycine dipeptide produced by GGT would reduce iron to ferrous iron; and the latter would induce to the development of hydrogen peroxide and endogenous superoxide anion radicals, further aggravating oxidative stress injury. 36 Secondly, in our opinion, increased GGT levels are also a sign of insufficient antioxidant capacity. GGT is essential in the maintenance of GSH homeostasis. 37 In contrast, of the six enzymes involved in the GSH cycle, only GGT is located outside the cell. 38 Therefore, it is the rate limiting enzyme in the whole process. 39 In contrast, the cysteine required in the generation of GSH mainly depends on the extracellular GGT catalytic production. 40 Glutathione depletion could lead to an upregulation of GGT as a compensatory response. 41 Thirdly, GGT levels also reflect the inflammatory state as they have been reported to be positively correlated with a variety of inflammatory substances, including C-reactive protein, tumour necrosis factor-α and interleukin-6.42–44 In addition, GGT itself is also proinflammatory by mediating the transformation of leukotriene C4 containing glutathione into leukotriene D4. 45 Both oxidative stress and inflammation have been shown to be involved in the development of T2DM. 46 GGT level was also reported to be positively associated with many T2DM-related risk factors, including red meat intake, visceral fat accumulation and hyperlipidaemia.47,48
The non-linear relationship between GGT and T2DM risk found in this current study was also previously reported by a meta-analysis, 10 which evaluated 24 eligible studies and found that the GGT level contributes to an increased risk of T2DM in a non-linear dose-dependent manner. The previous meta-analysis identified an inflection point of 35 IU/l in which one unit change in GGT led to a 34% increase in the risk of T2DM. 10 Although this inflection point was higher than that identified in this current study, both analyses indicated that a saturation effect was reached. 10 The non-linear relationship identified between GGT and T2DM not only has a very important clinical value, but also improves the understanding of the role of GGT in T2DM. The findings of this current study suggest that GGT level was closely associated with T2DM risk even when the level was under 10 IU/l. This effect might be reversible during this period. The timely intervention in terms of GGT level and its related T2DM risk factors may provide some clinical significance for T2DM prevention in the future. Meanwhile, as the regulation of translation, existence form in serum and the catalytic specificity of GGT remain to be elucidated fully, the discovery of this non-linear relationship between GGT and T2DM risk, which is more complicated than a simple linear association, would support the further exploration of GGT. For example, though GGT does not depend on the transport of specific lipoproteins in serum, four interchangeable serum GGT fractions have been identified according to their molecular weight: big-GGT (b-GGT; 2000 kDa), medium-GGT (1000 kDa), small-GGT (250 kDa) and free-GGT (70 kDa); among which, there is limited evidence that b-GGT might be closely associated with metabolic syndrome. 49 However, the routine method used to measure serum GGT is the initial rate method, with a normal range of 0–50 IU/l, which is sensible, but non-specific because it cannot discriminate between the four existing GGT fractions. To a certain extent, this limitation of the GGT detection method hinders further interpretation of the relationship between GGT and T2DM, which makes it difficult to determine whether the complex non-linear relationship is caused by the different specificity of the GGT fractions.
All limitations of the original study are also applicable to the current study. 12 First, as all of the participants were of Japanese descent, further analyses are needed to establish the generalizability to populations with other genetic backgrounds. Secondly, the insulin concentration was not measured in the original study, so the interaction between insulin and GGT was not considered. Thirdly, the incidence of T2DM might be underestimated due to the lack of oral glucose tolerance testing. Lastly, as participants with under-medication, alcoholic fatty liver disease, viral hepatitis or abnormal liver function at baseline were excluded from the final analyses, the conclusion reached in this current study might not be applicable for the general population. Because of limited data availability, other potential covariates were not included in the adjusted model.
In conclusion, this current secondary analysis of a large-scale, long-term dataset in a Japanese population suggests that an increase in the circulating level of GGT might be a risk factor in the development of T2DM. This suggests the potential clinical value in considering the non-linear impact of GGT for routine screening of high-risk individuals to improve early intervention for T2DM prevention.
Supplemental Material
sj-pdf-1-imr-10.1177_0300060520937911 - Supplemental material for Non-linear relationship between gamma-glutamyl transferase and type 2 diabetes mellitus risk: secondary analysis of a prospective cohort study
Supplemental material, sj-pdf-1-imr-10.1177_0300060520937911 for Non-linear relationship between gamma-glutamyl transferase and type 2 diabetes mellitus risk: secondary analysis of a prospective cohort study by Hao Wang, Lixia Li and Shouyan Zhang in Journal of International Medical Research
Supplemental Material
sj-pdf-2-imr-10.1177_0300060520937911 - Supplemental material for Non-linear relationship between gamma-glutamyl transferase and type 2 diabetes mellitus risk: secondary analysis of a prospective cohort study
Supplemental material, sj-pdf-2-imr-10.1177_0300060520937911 for Non-linear relationship between gamma-glutamyl transferase and type 2 diabetes mellitus risk: secondary analysis of a prospective cohort study by Hao Wang, Lixia Li and Shouyan Zhang in Journal of International Medical Research
Footnotes
Acknowledgement
The authors thank all the staff members in their institutions. The authors specially thank the data providers of this study. They completed the whole study and shared their data selflessly and kindly.
12
They are (the rankings and institutions of these researchers are ranked according to the original reference12): Professor T Okamura, Professor Y Hashimoto, Professor M Hamaguchi, Professor A Obora, Professor T Kojima and Professor M Fukui (corresponding author) (Department of Diabetology, Kameoka Municipal Hospital, Kameoka, Japan. ![]() ) for English language editing.
) for English language editing.
Author contributions
Hao Wang and Lixia Li contributed to data acquisition, analysis and manuscript drafting. Shouyan Zhang contributed to data interpretation, manuscript conception design and revision. All the authors read and approved the final manuscript.
Declaration of conflicting interests
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.