
Abstract
Objectives
In transplantation surgery, the ischaemic organ and reperfusion impairment after cold storage remains a considerable risk factor for impaired function and potential failure of the grafted organ. Substantial logistical efforts have been undertaken to reduce the cold ischaemic time because the demand for available transplant organs and the periods of cold ischaemia are increasing.
Methods
Four molecules were investigated (erythropoietin, sildenafil, lazaroid [U74389G], octreotide) in individual intravenous infusions 1 hour before the organ was harvested. This study was performed in 30 healthy landrace/large-white pigs (male; >10 weeks old; average weight, 22 ± 2 kg) in groups of six. The organs were studied at harvest, and at 8 and 24 hours post-harvest.
Results
The lazaroid molecule increased malondialdehyde (MDA) levels in the liver and pancreas at 8 hours. Hepatic lazaroid molecules improved liver histology at 8 and 24 hours. For kidneys, erythropoietin had a positive effect at 24 hours post-harvest. For the pancreas, octreotide showed better performance. In the lungs, there was less interstitial oedema with erythropoietin and lazaroid compared with the control group at 8 hours post-harvest.
Conclusion
All molecules had a positive effect and decreased ischaemia/reperfusion graft injury. Thus, pretreatment before organ harvest has a beneficial role.
Keywords
Introduction
Ischaemia/reperfusion (I/R) injury is a considerable risk factor for impaired graft function and potential failure of the transplanted organ. We examined logistical efforts to optimise harvested organ preservation until transplantation can occur. Cold ischaemia often worsens the organ’s condition during transplantation. Many studies have been conducted to define substances that minimise I/R injury. I/R must be taken into account in liver, kidney, lung, and heart transplantation procedures.1–3 The shortage of livers and other organs for transplant has justified the value of marginal donor livers to enlarge the donor organ pool. The main aim should be the optimal preservation of organs to minimise reperfusion damage and assist in achieving a successful transplantation. Thus, strategies to improve the graft quality are particularly important when determining the extended criteria for future donor organs. 4
Organs obtained from a cadaveric donor have endothelial injury that is produced from warm I/R. In an experimental setting, nitroglycerin perfusion and inhaled nitric oxide (NO) decreased warm I/R injury in non-beating heart and lung donors by reducing oedema during perfusion. 5 This I/R damage is associated with apoptosis and inflammation.6–8 Erythropoietin, sildenafil, lazaroid (U74389G), octreotide, melatonin curcumin, simvastatin, N-acetyl-cysteine, pentoxifylline, glycine, and methylprednisolone were investigated in an individual or mixed infusion regimen.9,10
Erythropoietin has a haematopoietic effect and other protective roles because of its anti-apoptotic, anti-antioxidant, and anti-angiogenic properties. Studies showed that the pre-ischaemic administration of erythropoietin has a protective role in I/R injury for various organs. The reduction in malondialdehyde (MDA), which is a lipid peroxidation marker, serum level alanine aminotransferase (ALT), and tumour necrosis factor-α (TNF-α) levels reduces cellular apoptosis in organs and might be useful for determining effective and less harmful treatment protocols.5,7,9,13
Octreotide is a synthetic analogue that mimics natural somatostatin, and it was approved by the United States Food and Drug Administration (US FDA) in 1988. It was administered for the management of carcinoid and vasoactive intestinal peptide-secreting tumours and for growth hormone-producing tumours. In clinical trials, it was used in pancreatitis, surgery, transplantation, and short bowel syndrome, and other indications for this analogue are hypercalcaemia, cancer-related pain, polycystic ovary syndrome, oesophageal varices caused from liver cirrhosis, and various cancers. From the pathophysiologic mechanism, octreotide inhibits hepatic fibrosis, bile duct proliferation, and bacterial translocation in obstructive jaundice. Studies have also shown the positive effect of hepatic I/R (HIR) in acute kidney injury. 6
Lazaroid (21-aminosteroid, U74389G) is a molecule in the steroid family in which the carbon 21 molecule has been exchanged with an amino group. With this change, lazaroid keeps the membrane stable and prevents the anti-inflammatory side effects of steroids. Lazaroids suppress cytokine production, adhesion molecule expression, and neutrophil activation and infiltration. Pretreatment of organ donors with lazaroid improves the viability of the liver that is harvested from non-beating heart donors. This positive effect has been shown and in other organs such as the heart, kidney, and lung.11–15
Sildenafil consists of a phosphodiesterase-5 inhibitor, which increases the guanosine 3,5-cyclic monophosphate (cGMP) concentration in response to arterial vasodilation. Preconditioning with sildenafil has been protective against endothelial dysfunction in the transplanted heart, and it has shown haemodynamic improvement of auto-transplanted kidneys in an animal model. 16 The mechanism of sildenafil reaction against I/R is based on the activation of antioxidant genes (e.g. Nrf2, HO-1, and NQO-1 anti-apoptotic genes) and attenuation of pro-inflammatory cytokines. 17
In the present experimental model, the effect of erythropoietin, sildenafil, octreotide, and lazaroid molecules that were infused as diluted solutions for 1 hour before harvesting organs including the heart, kidney, pancreas, liver, and lung was studied in swine. The aim of the current study was to identify the effects and differences between these molecules in an experimental model of organ harvest and preservation using five solid organs for transplantation. Despite published evidence for many substances, 18 our experience has shown the mechanism of reaction for four solutions (erythropoietin, sildenafil, octreotide, and lazaroid),7,10,15,19,20 and we have improved their positive effects in our laboratory. 8,21–26
Materials and methods
Animals
The experimental protocol was approved by the Ethics and Research Protocol Evaluation Committee at the ELPEN Experimental, Educational and Research Centre, in accordance with the European Directive 63/2010 (license reference number 8141/16-12-2014).
The study was performed in 30 healthy landrace/large-white pigs (male sex, 10 weeks old, average weight, 22 ± 2 kg). The number of animals was based on the guiding principles for the humane purpose of animals for scientific purposes (the three ‘Rs’: replacement, reduction, and refinement). The animals were fasted overnight and had ready access to water. Before any procedure, animals were randomised into five groups, as follows: control, erythropoietin, sildenafil, octreotide, and lazaroid groups. Each group contained six animals (Table 1). The investigators were blinded to the group allocation during the experiment.
Groups of animals and basic study design.
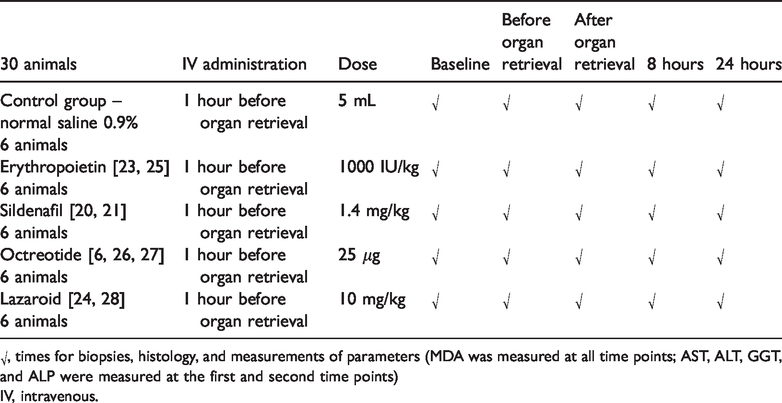
√, times for biopsies, histology, and measurements of parameters (MDA was measured at all time points; AST, ALT, GGT, and ALP were measured at the first and second time points)
IV, intravenous.
Anaesthesia
All animals were pre-medicated using midazolam (0.57 mg/kg body weight [B.W.]) and ketamine (15 mg/kg B.W.), which were both administered intramuscularly (i.m.), and atropine (0.045 mg/kg B.W.) was administered endotracheally 10 minutes before intubation. The intubation was performed with propofol (3 mg/kg), fentanyl (0.012 mg/kg), and cisatracurium besylate (0.5 mg/kg), which were administered as an intravenous (IV) bolus via an ear vein. General anaesthesia was provided using 4% sevoflurane, and sedation was achieved using fentanyl (2 mg = 4 amp in 500 mL of 0.9% saline) and cisatracurium besylate (200 mg = 10 amp Nimbex in 500 mL of 0.9% saline) at 60 to 80 mL/hour IV, which was continuously administered via an ear vein. The animals remained intubated and mechanically ventilated using 40% FiO2 at 20 breaths/minute (Taema Clarys 2000 Antony Cedex, Antony, France). All animals’ vital signs were closely monitored during the procedure (arterial pressure, oxygen saturation, and cardiac rate).
Surgery, biopsies, and organ flushing and procurement
An abdominal midline incision and sternotomy (chest incision) were performed. Except for the heart, biopsies were taken from all organs that were studied (i.e., kidney, liver, pancreas, and lung). Four catheters were then inserted using the Selinger technique through the cardiac aorta, the pulmonary artery, the portal vein, and the abdominal aorta (inferior to the renal aorta). The entire surgery time for this step was 50 minutes. Then, 1 hour before organ flushing and retrieval, the study molecules (erythropoietin [1000 IU/kg IV], sildenafil [1.4 mg/kg IV], octreotide [25 μg IV], and lazaroid [10 mg/kg]) or saline (0.9% saline; 5-ml bolus IV) for the control group was administered at the respective dose (Table 1).
Five minutes before organ harvesting, 1000 IU of heparin was administered IV as well as ceftriaxone (Elpen Pharmaceuticals, Pikermi, Greece) at a dose of 2000 mg/20 ml as chemoprophylaxis. During organ retrieval, all catheters contained cold University of Wisconsin solution (UW; Bridge to Life, London, UK) solution and the preservation solution was flushed until all organs were fixed for the ultimate step of procurement. Main operational time for organ flushing and retrieval was 20 minutes. Cold UW solution was also used for the next steps of preservation. Organs were placed independently into sterile bags and these bags were placed inside boxes that were preserved at −4°C. In addition to the baseline biopsy that was taken from the organ immediately after the abdominal cavity was opened (except for the heart), biopsies were taken from each organ (except the heart) before organ retrieval, immediately after organ retrieval, and at 8 and 24 hours after organ retrieval.
Malondialdehyde
We calculated the levels of malondialdehyde (MDA), which is a molecule that is used as an indicator of lipid peroxidation, in the organs that were studied (heart, kidney, pancreas, liver, and lung) in all the study groups (control, erythropoietin, sildenafil, octreotide, and lazaroid). A selective third-order derivative method was used to detect MDA. Briefly, 1-g organ samples were thoroughly homogenised (Polytron homogeniser, PCU; Kinematica, Lucerne, Switzerland) with 5 ml of 5% aqueous trichloroacetic acid (Merck, Darmstadt, Germany) and 2 mL of 0.8% butylated hydroxytoluene (Sigma Chemical, St Louis, MO, USA) in hexane (Merck), followed by centrifugation (3000 ×g for 15 minutes). The top layer was discarded, and a 2.5-ml aliquot from the bottom layer was mixed with 1.5 mL of 0.8% aqueous 2-thiobarbituric acid (Sigma) and incubated at 70°C for 30 minutes. Following incubation, the mixture was cooled to room temperature and analysed using conventional spectrophotometry (model UV-160A; Shimadzu, Tokyo, Japan) at 400–650 nm with a scanning speed of 480 nm/minute. Third-order derivative spectra of samples from both the control and drug-treated rats were obtained using electronic differentiation (derivative difference setting, 21 nm) of the conventional absorption spectra. The MDA concentration (nmol/g wet tissue) was calculated based on the third-order derivative peak height at 532 nm, which refers to the slope and intercept data of the computed least-squares fit using the standard calibration curve. 26 MDA levels were measured at baseline, immediately before organ retrieval, immediately after organ retrieval, and at 8 and 24 hours after organ retrieval.
Histopathologic assessment
Tissue specimens were fixed in neutral formalin (10%) and embedded in paraffin in accordance with standard histologic procedures. Then, 4-μm-thick sections of paraffin-embedded tissue samples from each organ were sectioned, deparaffinised, rehydrated, and finally subjected to conventional haematoxylin and eosin staining. The histopathologic assessment was conducted on swine pancreatic, liver, kidney, heart, and lung tissues by two experienced pathologists (EAT and EL) who were blinded to the experimental protocol. Assessment of the pancreas included many parameters, as described in a previous publication by our group. 25 Briefly, a four-point scale was used to determine the severity of histologic changes in the pancreas (0, no change to 3, severe damage). The presence of oedema, haemorrhage, acinar necrosis, and cell vacuolisation (vacuoles) were classified using a range from 0 to 3 (0, absent to 3, severe). Liver damage was also classified using a range from 0 to 3 (0, absent to 3, severe). For the liver, the following parameters were assessed: portal inflammation, steatosis, leucocyte infiltration, sinusoidal dilation, and congestion. 27 Histology was assessed at baseline, immediately before organ retrieval, immediately after organ retrieval, and at 8 and 24 hours after organ retrieval.
The same parameters (interstitial oedema, alveolar oedema, inflammation, leucocytes, haemorrhage, and alveolar dilation) were used to assess lung tissue alterations. The presence and severity of interstitial oedema, alveolar oedema, chronic inflammatory infiltration, leucocyte infiltration, pulmonary haemorrhage, and alveolar dilation were assessed. 28 Kidney tissue injury was evaluated as well as the presence of tubular dilation, oedema, interstitial infiltrate, and cell sloughing. The parameters of dilation, cell sloughing, and interstitial infiltrate were scored as follows: 0, 0%; 1, 1% to 10%, 2, 11% to 50%; and 3, >50% of each field. The presence of oedema was graded on a binormal scale (0, no; 1, yes). 29 Heart tissue alterations were determined by rating the presence or absence of oedema and leucocyte infiltration using a binary scale (0, no; 1, yes). Tissue samples were assessed at harvesting and at 8 and 24 hours after organ retrieval.
Biomarker assessment
Biochemical markers (aspartate aminotransferase [AST], alanine aminotransferase [ALT], gamma glutamyl transferase [GGT], alkaline phosphatase [ALP], amylase, creatine and troponin) were assessed in the organs before infusion of molecules, before harvesting, at the time of harvest or after 8 or 24 hours. The blood samples were centrifuged at 1,200 ×g at room temperature (21°C). After centrifugation, the plasma was separated and analysed. The concentrations of AST, ALT, GGT, ALP, amylase, creatine, and troponin levels were determined by enzymatic procedures using a Roche/Hitachi Modular System P (Roche Diagnostics, Mannheim, Germany).
Statistical analysis
Data were expressed as the median and interquartile range (IQR) for ordinal variables and as frequencies and percentages for categorical variables. The comparison between groups of ordinal variables at each time point was performed using the Kruskal–Wallis test. Pairwise comparisons were performed using the Mann–Whitney test. The chi-square test was used to compare between groups of categorical variables at each time point. Pairwise comparisons were performed using the z-test. A one-way analysis of variance (ANOVA) followed by the Bonferroni post-hoc test was also used. All tests were two-sided, and statistical significance was defined as p < 0.05. All analyses were performed using the Statistical Package for the Social Sciences (SPSS) version 17.0 (SPSS Inc., Chicago, IL, USA).
Results
Biochemical markers
Biochemical markers including AST, ALT, GGT, ALP, amylase, creatine, and troponin levels were assessed. Biomarker levels in the organs were assessed at two time points: time 1 (before infusion of molecules) and time 2 (before harvesting).
For ALT, there was no difference in the percentage change from time 1 (before infusion of molecules) to time 2 (before harvesting) in all groups. There was a non-significant decreasing trend in the biomarker levels as follows: octreotide, erythropoietin, sildenafil, lazaroid, and the control group (group without any infusion). AST, ALP, GGT, amylase, creatine, and troponin levels also showed no statistical differences.
Malondialdehyde
MDA levels were calculated from tissue samples before the organs were harvested, and after 8 and 24 hours of cold ischaemia. The MDA results are presented in Table 2.
In the peripheral part of the liver, there was a statistically significant reduction in MDA levels in the erythropoietin group compared with the control group (p = 0.010). There were no statistically significant differences in the MDA level between the groups after 24 hours of cold ischaemia (Table 2).
MDA results.
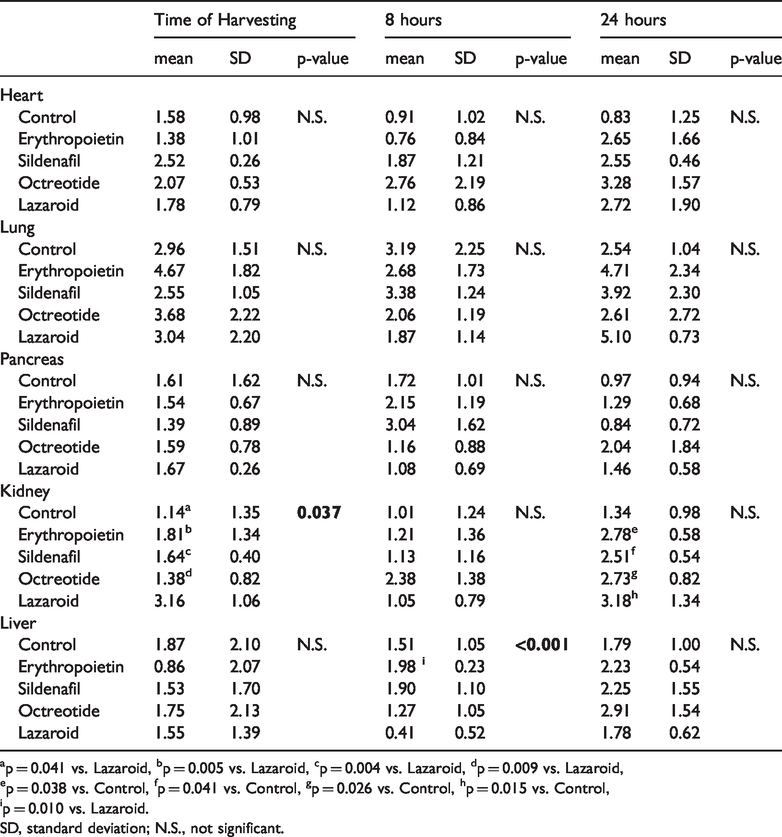
ap = 0.041 vs. Lazaroid, bp = 0.005 vs. Lazaroid, cp = 0.004 vs. Lazaroid, dp = 0.009 vs. Lazaroid,
ep = 0.038 vs. Control, fp = 0.041 vs. Control, gp = 0.026 vs. Control, hp = 0.015 vs. Control,
ip = 0.010 vs. Lazaroid.
SD, standard deviation; N.S., not significant.
At baseline, MDA values were significantly lower in the control group (p = 0.041), erythropoietin group (p = 0.005), sildenafil group (p = 0.004), and the octreotide group (p = 0.009) compared with the lazaroid group. After 24 hours of cold ischaemia, MDA values were significantly lower in the control group compared with the erythropoietin (p = 0.038), sildenafil (p = 0.041), octreotide (p = 0.026), and lazaroid (p = 0.015) groups (Table 2).
MDA levels in the pancreas, heart, and lungs showed no statistically significant differences at 8 or 24 hours after organ removal (Table 2).
Histopathology assessment
Five parameters (portal inflammation, polymorphonuclear leucocytes, steatosis, dilation, and congestion) were assessed from the central and peripheral liver. In the central part of the liver, portal inflammation was significantly higher in octreotide (p = 0.041) and sildenafil (p = 0.041) groups compared with the control group after 8 hours of cold ischaemia. There was no significant difference in portal inflammation after 24 hours of cold ischaemia. Similarly, there was no significant difference for polymorphonuclear leucocytes, steatosis, and dilation at harvest or after 8 or 24 hours of cold ischaemia. After 8 hours of cold ischaemia, the lazaroid group showed minimal dilation compared with erythropoietin (p = 0.017) and sildenafil (p = 0.041) groups. Additionally, congestion was not significantly difference between the groups at harvest, or after 8 or 24 hours of cold ischaemia (Table 3).
Liver histology.

ap = 0.041 vs. Control, bp = 0.041 vs. Lazaroid,
cp = 0.041 vs. Lazaroid, dp = 0.009 vs. Lazaroid.
fp = 0.025 vs. Lazaroid, gp = 0.015 vs. Lazaroid.
hp = 0.015 vs. Control, ip = 0.009 vs. Control, jp = 0.017 vs. Lazaroid, kp = 0,041 vs. Lazaroid.
SD, standard deviation; IQR, interquartile range; N.S., not significant.
Histology of the kidney.

ap = 0.087 vs. Erythropoietin at 24 hours.
N.S., not significant.
In the peripheral areas of the liver, portal inflammation was significantly reduced in the lazaroid group compared with the erythropoietin (p = 0.041), sildenafil (p = 0.041), and octreotide (p = 0.009) groups after 8 hours of cold ischaemia. The number of polymorphonuclear leucocytes was not significantly different at organ harvest or after 8 or 24 hours of cold ischaemia. There was less steatosis in the sildenafil (p = 0.015) and erythropoietin (p = 0.025) groups compared with the lazaroid after 24 hours of cold ischaemia. There was no significant difference between groups for dilation and congestion at harvest or after 8 or 24 hours of cold ischaemia (Table 3; Figure 1); Photo Figure 1).

Central part of the liver parenchyma after 8 hours of cold ischaemia and treatment with sildenafil. There is minimal portal inflammation, congestion, and polymorphonuclear lymphocytes and no steatosis is observed. H&E staining (magnification ×200).
The following four parameters were assessed in the kidney: oedema, dilation, interstitial infiltrate, and sloughing at organ harvest and after 8 or 24 hours of cold ischaemia. There was no significant difference for kidney dilation, interstitial infiltrate, and oedema between the groups at harvest or after 8 or 24 hours of cold ischaemia. Sloughing in the erythropoietin group showed a statistically significant increase in the kidney at 24 hours (10% of sloughing) compared with the control group (p = 0.036; Table 4; Figures 2 and 3).

Kidney parenchyma after 8 hours of cold ischaemia and treatment with lazaroid. Minimal sloughing is observed, and there is also no dilation, interstitial infiltrate, or oedema. H&E staining (magnification ×400)

Kidney parenchyma after 8 hours of cold ischaemia and treatment with octreotide. Minimal sloughing is observed, and there is no dilation, interstitial infiltrate, or oedema. H&E staining (magnification ×400)

Lung parenchyma after 8 hours of cold ischaemia and treatment with erythropoietin. There is minimal alveolar dilation, while no interstitial oedema, alveolar oedema, inflammation, leucocytes, or haemorrhage is observed. H&E staining (magnification ×200)

Histology images from all phases of the experiment.
Histomorphologic alterations in the pancreas were assessed using a four-point scoring system that ranged from absent to severe (0, 1, 2, 3) (Table 5). Pancreatic oedema, haemorrhage, polymorphonuclear leucocytes, vacuoles, and acinar necrosis were also investigated. No significant differences were found for haemorrhage, polymorphonuclear leucocytes, vacuoles, and necrosis. For oedema in the pancreas, there was a significant increase in the erythropoietin (p = 0.004), octreotide (p = 0.015), and lazaroid (p = 0.026) groups compared with the control group when the organ was harvested. There was no oedema in the control group. There was no significant difference in oedema between the sildenafil group and the control group. No groups showed haemorrhage at any of the three observation times. To indicate the presence or absence of vacuoles, the following scoring system was used: ‘0’ indicated no vacuoles; and ‘1’ indicated the presence of vacuoles. Statistical analysis showed a statistically significant difference, with vacuoles present in 50% of the pancreas cells in the octreotide group compared with 0% in the control group, lazaroid group, and sildenafil group (P < 0.182) when the pancreas was harvested. There was no statistically significant difference at 8 and 24 hours compared with the control group (Table 5).
Histology of the pancreas.

ap=0.004 vs. Control, bp=0.015 vs. Control.
cp=0.0182 vs. Control, dp=0.0182 vs. octreotide.
*‘0’ indicates no vacuoles; ‘1’ indicates the presence of vacuoles.
SD, standard deviation; IQR, interquartile range; N.S., not significant.
Polymorphonuclear leucocytes and oedema were assessed in the heart. There was no statistically significant difference between the polymorphonuclear leucocytes and oedema at all time points (Table 6).
Histology of the heart.

SD, standard deviation; N.S., not significant.
In the lungs, the following parameters were studied: interstitial oedema, alveolar oedema, inflammation, leucocytes, haemorrhage and alveolar dilation. At the time of harvest, there was less (no) interstitial oedema in the erythropoietin (p = 0.017) and sildenafil (p = 0.04) groups compared with the octreotide group. Additionally, there was less (no) oedema in the erythropoietin (p = 0.017) and lazaroid (p = 0.017) groups after 8 hours of cold ischaemia compared with the control group. There was no difference in alveolar oedema inflammation, leucocytes, haemorrhage, and alveolar dilation between the groups (Table 7; Figures 4 and 5).
Histology of the lung.
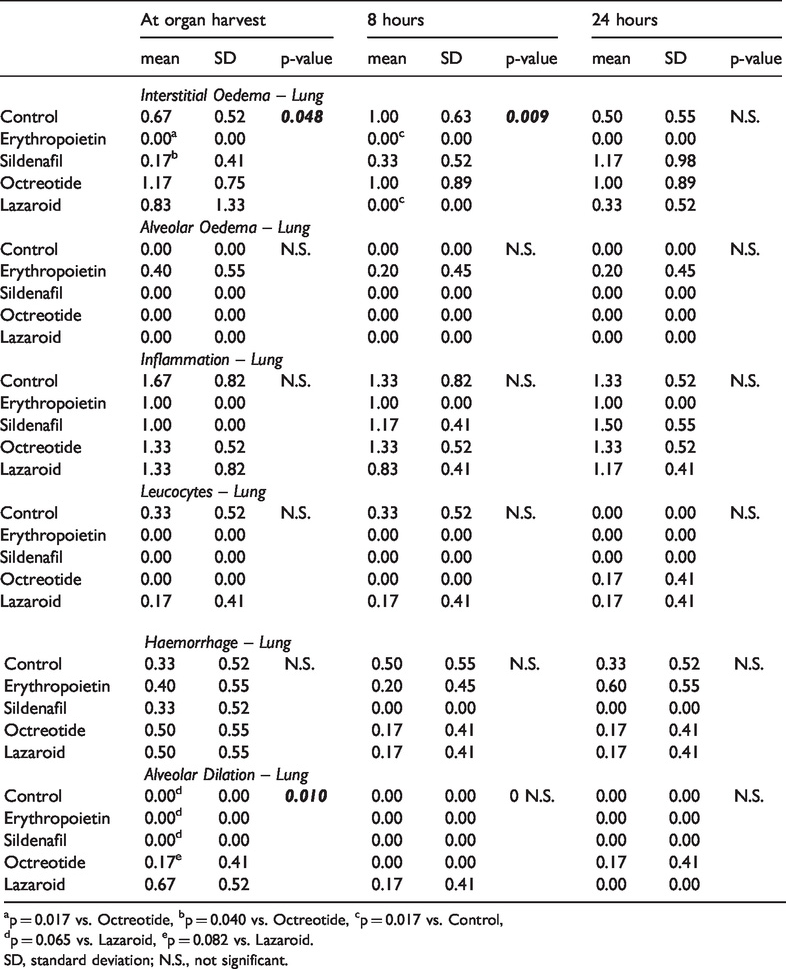
ap = 0.017 vs. Octreotide, bp = 0.040 vs. Octreotide, cp = 0.017 vs. Control,
dp = 0.065 vs. Lazaroid, ep = 0.082 vs. Lazaroid.
SD, standard deviation; N.S., not significant.
Discussion
In this study, we evaluated the effect of intravenous pretreatment with erythropoietin, sildenafil, octreotide, and lazaroid on the liver, heart, pancreas, kidney, and lungs before the organs were harvested in an animal model of organ preservation and cold ischaemia for 8 and 24 hours. To the best of our knowledge, this study is the first study to investigate the effects of sildenafil, octreotide, lazaroid, and erythropoietin in cold ischaemia in landrace/large-white swine to improve organ preservation before transplantation.
The increase in free radicals after I/R is broadly discussed in the literature. 30 Additionally, the protective effect of each of these solutions (erythropoietin, sildenafil, octreotide, and lazaroid) has been shown. Many markers, such as MDA, have been used to investigate I/R. MDA is generally accepted as a sensitive marker for the rate of lipid peroxidation, and it exists as the final product of lipid peroxidation. 31 Current results showed that pretreatment with lazaroid resulted in a decrease in hepatic MDA levels compared with the erythropoietin group.
Biochemical marker levels were not different at baseline or after 8 and 24 hours of cold ischaemia, indicating that these biomarkers did not play a role in organ preservation during cold ischaemia. This means that all surgical procedures were safe and the molecules did not have an influence on the biochemical profile.
In transplantation research, important parameters for the evaluation of organ quality are oxidative stress and analytical histopathological evaluation. 32 Histolo-gical analysis of the liver was divided into two parts: central and peripheral. In the central part of the liver, octreotide and sildenafil played a role in reducing portal inflammation after 8 hours of cold ischaemia because dilation seems to be reduced in the sildenafil group at 24 hours after starting cold ischaemia. However, all other markers for these groups did not show any statistically significant results to improve the protective effect of sildenafil in a central part of the liver. The lazaroid showed a reduction in portal inflammation, which was in contrast to octreotide and sildenafil after 8 hours of cold ischaemia preservation in a peripheral part of the liver. Sildenafil in the peripheral part of the liver showed an improvement in steatosis (absent) after 24 hours of liver cold preservation. Based on this result, sildenafil may play a more critical role in protection against ischaemia up to 24 hours after organ harvest. Both sildenafil and lazaroid have a potential effect against portal inflammation through their protective role against free radicals. Sildenafil induces NO production because it is a selective PDE5 inhibitor, and this could enhance the beneficial action, which was demonstrated in the current model after 24 hours of cold ischaemia.8,27 The effect of sildenafil and lazaroid were also shown to be beneficial in the kidney.
Erythropoietin plays a leading role against tubular necrosis. Thus, the role of a free radical scavenger may be significant for cold ischaemia. In the present model, lazaroid, sildenafil, and octreotide showed additional sloughing compared with the erythropoietin and control groups. Similar findings were presented in a review paper. 33
Histopathological injury in the pancreas comprises various cytoplasmic vacuoles, massive interstitial oedema, and inflammatory cell infiltration, as was previously described. 34 In our study, histopathological findings indicated a reduction of vacuoles in the lazaroid and sildenafil groups compared with the octreotide group when the organ was harvested. Histopathology analysis from the lung showed that erythropoietin compared with the control group had a more positive effect with no interstitial oedema after 8 hours of cold ischaemia. These findings are explained by erythropoietin’s interaction with Toll-like receptor-4/nuclear factor-κB in lung tissue, as shown by an improvement in interstitial oedema during lung ischaemia and injury in an experimental rat model. 35
Limitations and further study
In the present study, only MDA was tested. TNF-α and all the other parameters were excluded because of the excessive cost. Another limitation was studying the molecules separately with no comparison between them. Additionally, there was no group that contained all four molecules. In the literature, other techniques are discussed based on the cell metabolism in the organs, and this may reduce I/R injury. One of these methods is oxygenation during machine perfusion (MP) at a different temperature (hypothermic, subnormothermic, or normothermic). The findings show that the re-introduction of tissue adenosine triphosphate (ATP) levels in the current method may be valuable for improving the viability assessment of organs that are harvested for transplantation. 36 These findings may help with future investigations. Our purpose was to investigate each of these molecules (erythropoetin, sildenafil, lazaroid, and octreotide), and based on the results, to design further studies.
Conclusion
I/R injury is a multifactorial reaction, and many mechanisms play an essential role. All molecules had a specific effect against injury in a particular way. Pretreatment before organ harvesting seems to have a beneficial role. New designs for improvement of solid organ preservation can be designed. For example, the use of more than one molecule may protect against I/R injury and extend the period of organ preservation. Thus, other preservation protocols can be studied based on the presented results.
Footnotes
Acknowledgements
Statistical analysis was performed by Mr Antonis Galanos, PhD. The authors would like to express their sincere thanks to Mrs A. Zacharioudaki, Mr G. Stagias, Mrs M. Karamperi, Mrs E. Karampela, Mr N. Psychalakis, Mrs K. Tsarea, Mr E. Gerakis, and Mr S. Gerakis for their assistance during the experiments.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This study was funded as a Research Scholarship by the Experimental, Educational and Research Centre, ELPEN.