
Abstract
Objective
To compare the efficacy of ranibizumab plus fufang xueshuantong capsule (cFXST) with the efficacy of ranibizumab alone in treatment of exudative age-related macular degeneration.
Methods
This prospective, randomized, controlled, pilot study included 38 eyes from 38 patients with exudative age-related macular degeneration (AMD) that were randomly allocated into two cohorts of 19 eyes each: ranibizumab (Cr) and ranibizumab plus cFXST (Cfr). All patients received three monthly injections of ranibizumab. Patients in Cfr also received daily oral supplementation of cFXST. Best corrected visual acuity (BCVA) and thickness of the choroidal neovascularization-pigment epithelial detachment (CNV-PED) complex (measured by optical coherence tomography) were recorded at baseline and at 1 and 3 months after the first intravitreal injection of ranibizumab.
Results
In the Cfr, the CNV-PED complex thickness was reduced by 31.7% and 36.1% at 1 and 3 months, respectively; these reductions were significantly greater than the 19.7% and 24.2% reductions in the Cr. BCVA improvement was significantly greater in the Cfr than in the Cr after 3 months; the proportion of patients with functional response was also greater in the Cfr than in the Cr (16/16 vs. 8/17).
Conclusion
Oral cFXST increases the efficacy of short-term ranibizumab treatment for exudative AMD.
Keywords
Introduction
Exudative age-related macular degeneration (wet AMD) is a leading cause of blindness in older individuals worldwide. 1 It is characterized by choroidal neovascularization (CNV), intra- or sub-retinal fluid, and enhanced central macular thickness. 2 , 3 Sight-threatening CNV associated with wet AMD has been managed with variable success through nonpharmacologic methods, including laser photocoagulation, 4 submacular surgery, 5 external beam radiation, 6 and photodynamic therapy with verteporfin. 7 Vascular endothelial growth factor (VEGF) is a major factor in the etiology of AMD 8 ; thus far, anti-VEGF antibody treatment has been effective for wet AMD.9–11 Anti-VEGF treatment began with the approval of ranibizumab in 2006. 12 Four intraocular VEGF inhibitors are currently available for the treatment of wet AMD; three of these are Food and Drug Administration-approved, while one is used off-label. Two seminal clinical trials have demonstrated the efficacy of ranibizumab: approximately 90% of patients receiving monthly intravitreal ranibizumab lost <15 letters after 2 years. 12 , 13
Although anti-VEGF treatment of wet AMD is generally effective, some patients have poor or no response to anti-VEGF agents; persistent fluid is common after therapy. 14 After anti-VEGF treatment, approximately 10% to 15% of patients exhibit visual acuity loss and some remaining exudative lesions.15–17 Thus, alternative or adjunct approaches to anti-VEGF therapy are sought to improve visual acuity outcomes.
Traditional Chinese medicine of the Qing Dynasty identified wet AMD as a “blood stasis syndrome,” which refers to any disease that obstructs micro-circulation, causes irregular hemorheological properties, or abnormal hemodynamic characteristics. 18 Notably, wet AMD has been associated with some hemorheological parameters, such as von Willebrand factor, plasma fibrinogen, and plasma viscosity.19–21 Therefore, blood-promoting and stasis-removing drugs may improve the prognosis of patients with wet AMD.
Fufang xueshuantong capsule (cFXST) is a traditional Chinese herbal formula that has been used empirically to treat vitreous hemorrhage 22 and diabetic retinopathy. 23 , 24 The therapeutic benefit of cFXST has been confirmed in animal models of diabetic retinopathy 25 , 26 and retinal vein occlusion. 27 The bioactive components of cFXST that ameliorate circulatory dysfunction have been identified.28–30 These components influence serum proteins (e.g., von Willebrand factor, plasma fibrinogen, and antithrombin III), thereby attenuating erythrocyte aggregation, plasma viscosity enhancement, and acellular vessel formation. However, randomized controlled clinical studies related to the etiology of cFXST are lacking. This prospective randomized controlled study investigated the efficacy of oral cFXST as an adjunct treatment with intravitreal anti-VEGF therapy for wet AMD.
Patients and Methods
Patients and ethical approval
This randomized controlled clinical trial was conducted at the First Affiliated Hospital of Nanjing Medical University (Nanjing, China). Inclusion criteria were as follows: (1) age ≥50 years; (2) best-corrected visual acuity (BCVA) < 70 Early Treatment Diabetic Retinopathy Study (ETDRS) letters; and (3) active CNV, manifesting as wet AMD on fluorescein angiography (HRA 2 or Spectralis; both from Heidelberg Engineering, Heidelberg, Germany), and the presence of subretinal fluid (SRF) on optical coherence tomography (OCT) scans (Cirrus; Carl Zeiss Meditec, Inc., Dublin, CA, USA). Exclusion criteria were as follows: (1) subretinal fibrosis or atrophy; (2) polypoidal choroidal vasculopathy, verified by indocyanine angiography; (3) previous treatment with anti-VEGF drugs, photodynamic therapy, or vitrectomy; (4) cardiovascular or cerebrovascular events within the prior 12 months. This trial was performed in accordance with the tenets of the Declaration of Helsinki (Tokyo Revision); the protocol was approved by the Ethics Committee of the First Affiliated Hospital of Nanjing Medical University (approval no. 2015-SR-190). Written informed consent was obtained from all patients prior to participation in the study.
Treatment
Patients were randomly assigned to either the cFXST (Cfr) cohort or the ranibizumab (Cr) cohort. In total, three 0.05-mL intravitreal injections containing 0.5 mg ranibizumab (Genentech, Inc., South San Francisco, CA, USA) were administered to each patient (one injection per month for 3 months). After the first intravitreal ranibizumab injection, patients in the Cfr cohort began to receive three oral doses of cFXST per day (total dose of 4500 mg/day; batch no. 150201, state medical license no. Z20030017, Zhongsheng Pharmacy Co., Ltd, Guangdong, China). Patients in the Cr cohort received placebo pills, similar in appearance to the cFXST supplement. The same batch of cFXST was used throughout the trial to ensure consistent quality; this supplement comprised Panax notoginseng (Burkill) F.H. Chen, Astragalus membranaceus (Fisch) Bunge, Salvia miltiorrhiza Bunge, and Scrophularia ningpoensis Hemsl at a ratio of 25:8:5:8. 30
Outcomes
The primary outcomes were maximum SRF height and total center point thickness of the pigment epithelial detachment (CNV-PED) complex, as determined using OCT. The CNV-PED complex comprised retinal pigment epithelium thickness, retinal pigment epithelium elevation thickness, and subretinal hyper-reflective material thickness at the foveal center. These measurements were performed by a masked examiner (Z.H.) at baseline and at each subsequent visit. The OCT parameters at each visit were compared with their values at baseline; the change ratio was defined as follows: ratio = (value at baseline - value at visit)/value at baseline. The secondary outcome was BCVA, determined using an ETDRS letters chart at 4 m. Functional response was defined as BCVA improvement, compared with baseline. 31 , 32 The following data were collected at enrollment: age, sex, duration since wet AMD diagnosis, slit-lamp biomicroscopy findings for anterior and posterior segments, and intraocular pressure.
Statistical analysis
Statistical analysis was performed using SPSS Statistics, version 19.0 (IBM Corp., Armonk, NY, USA). Paired t-tests were used to compare follow-up and baseline data within each cohort. Student’s t-test was used for comparisons of continuous data between the two cohorts; Fisher’s exact test or the χ2 test was used for comparisons of categorical data between the two cohorts. Data are expressed as mean ± standard error of the mean. Differences with a two-tailed P-value of < 0.05 were considered to be statistically significant.
Results
In total, 38 patients were included in this study: 19 patients each in the Cfr and Cr cohorts. Baseline parameters were similar between the two cohorts (Table 1). In both cohorts, the center point thickness of the CNV–PED complex was significantly reduced at each visit, compared with the baseline value (Figure 1a). In the Cfr cohort, the reductions of CNV–PED thickness from baseline were 63 ± 11 µm and 72 ± 11 µm after 1 and 3 months, respectively; these did not significantly differ from the 27.1 ± 8.5 µm and 46 ± 9 µm reductions measured in the Cr cohort. However, change ratios significantly differed between the two cohorts. In the Cfr cohort, the CNV–PED thickness was reduced by 31.7% and 36.1% at 1 and 3 months, respectively; these reductions were greater than the 19.7% (P < 0.05) and 24.2% (P < 0.05) reductions in the Cr cohort (Figure 1b).
Characteristics of patients and baseline parameters in Cfr and Cr.

Abbreviations: Cr: cohort treated with ranibizumab alone; Cfr: cohort treated with fufang xueshuantong capsule plus ranibizumab; BCVA: best corrected visual acuity; ETDRS, Early Treatment Diabetic Retinopathy Study; PED: pigment epithelial detachment; SRF: subretinal fluid; IRF: intraretinal fluid; CNV: choroidal neovascularization.

Change in center point thickness of CNV-PED complex. a: CNV-PED complex thickness was significantly reduced after treatment in both Cfr and Cr. b: change ratios of CNV-PED complex thickness at each visit for both cohorts. Change ratio = (value at baseline - value at visit)/value at baseline. *P < 0.05; **P < 0.01; ***P < 0.001.
Furthermore, the SRF height was remarkably reduced in both cohorts (Figure 2). The change ratios of SRF height at each visit did not significantly differ between the cohorts. Two representative patients from each cohort are shown in Figure 3. One patient who received combined therapy exhibited a remarkable reduction of CNV–PED thickness (Figure 3a, c, e, g), while a patient who received ranibizumab alone exhibited less improvement (Figure 3b, d, f, h).
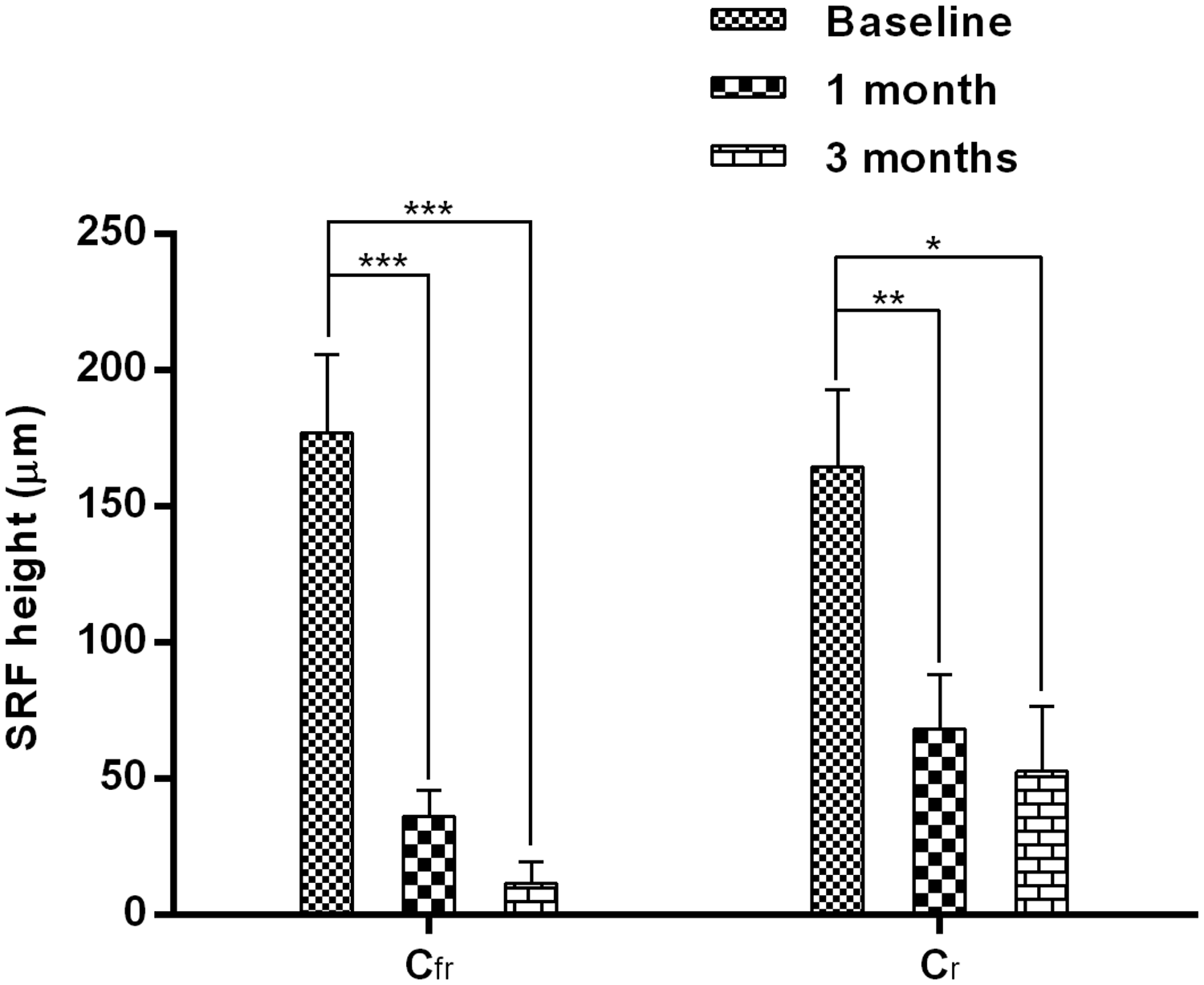
Change in SRF height. SRF height was significantly lower after treatment in both Cfr and Cr. *P < 0.05; **P < 0.01; ***P < 0.001.

Macular images obtained by spectral domain optical coherence tomography before and after treatment, in representative patients from Cfr (a, c, e, g) (patient 1) and Cr (b, d, f, h) (patient 2). After combined therapy (Cfr), the subretinal fluid (*) was quickly alleviated and CNV-PED complex thickness (white arrows) was reduced, with localized PED (△). After treatment with ranibizumab alone (Cr), subretinal fluid (*) and CNV-PED complex (white arrows) did not show remarkable changes.
In the Cfr cohort, the mean BCVA ETDRS letters at baseline, 1 month, and 3 months were 47.6 ± 5.5, 59.7 ± 5.9 (P < 0.001), and 62.2 ± 6.0 (P < 0.001), respectively. In the Cr cohort, the mean BCVA ETDRS letters at baseline, 1 month, and 3 months were 59.1 ± 3.8, 65.9 ± 3.3 (P < 0.001), and 64.9 ± 3.6 (P < 0.05), respectively (Figure 4a). At 3 months, the change in BCVA was significantly greater in the Cfr cohort than in the Cr cohort (14.7 ± 2.8 vs. 5.8 ± 3.1, P < 0.05) (Figure 4b), which was consistent with the OCT findings. At 3 months, the proportion of patients with functional response to treatment was also higher in the Cfr cohort than in the Cr cohort (16/16 vs. 8/17, P < 0.05).

Change in visual acuity. a: BCVA ETDRS letters were significantly larger after treatment in both Cfr and Cr. b: Change in BCVA (ETDRS letters) at each visit for both cohorts. *P < 0.05; ***P < 0.001. Change = BCVAvisit – BCVAbaseline.
Discussion
cFXST has been empirically used in Chinese clinics for many years, but no randomized controlled trials have been performed to assess its efficacy. To the best of our knowledge, this pilot study is the first such randomized controlled clinical trial. In this prospective, randomized study, involving patients with wet AMD, the major finding was that the clinical outcomes of combined anti-VEGF treatment with cFXST supplementation were significantly better than the outcomes of anti-VEGF treatment alone. The major outcomes measured in this study were the center point CNV-PED complex thickness and SRF height, the most commonly measured parameters used for assessment of wet AMD. Specifically, the change ratio of CNV–PED thickness at each visit showed significantly greater improvement in the Cfr cohort than in the Cr cohort. Furthermore, BCVA improvement at 3 months was superior in the Cfr cohort compared with Cr cohort . The current findings are consistent with the results of studies in animal models.28–30 The following alternative treatment strategies have yielded inconsistent results: combination therapy with photodynamic therapy, 33 core vitrectomy, 34 epimacular brachytherapy, 35 low-dose transpupillary thermotherapy, 36 switch to biweekly anti-VEGF dosing or algorithms, 37 adjunct pharmacologic treatment with intravitreous corticosteroids, 38 omega-3 supplementation, 39 and topical dorzolamide-timolol eyedrops. 40 As expected, intravitreal ranibizumab treatment alone induced significant functional and morphological improvement, as reported previously. 12 , 13 No statistically significant difference was detected in terms of the change in SRF height between the two cohorts; both treatments resulted in remarkable reduction of maximum SRF height.
The limitations of the current study include its small sample size and limited follow-up duration. In addition, this study did not investigate which components of the cFXST formula were responsible for the observed beneficial effects. Future studies should focus on the effectiveness of specific bioactive components administered orally, topically, or intravitreously. Another limitation of the current study was that patient compliance was evaluated by self-reporting measures. Finally, this study relied on manual measurements of CNV-PED thickness and SRF height rather than automated computer algorithms; this may have introduced bias.
In summary, we believe that supplementation of cFXST can serve as an effective adjunct therapy for further alleviation of retinal microcirculatory disturbance, especially for patients with poor or no response to anti-VEGF treatment. Adjunct therapy comprising daily oral supplementation of cFXST might increase the short-term effectiveness of anti-VEGF therapy for patients with wet AMD. Because this was a pilot study, larger sample sizes and longer follow-up periods are needed to confirm our results.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This study was supported by the National Natural Science Foundation of China (grant no. 81900875), Natural Science Foundation of Jiangsu Province (grant no. BK20191059), and National Key Project of Research and Development Plan (grant no. 2017YFA0104101), and General Project of the National Natural Science Fund (grant no. 81770973).