
Abstract
Osteoarthritis (OA) is a chronic joint disorder that causes degeneration of cartilage, synovial inflammation, and formation of osteophytes. Aging, obesity, and sex are considered the main risk factors of OA. Recent studies have suggested that metabolic syndrome (MetS) disorders, such as hypertension, hyperlipidemia, diabetes mellitus, and obesity, may be involved in the pathogenesis and progression of OA. MetS disorders are common diseases that also result in atherosclerosis. Researchers believe that OA and atherosclerosis have underlying similar molecular mechanisms because the prevalence of both diseases increases with age. Oxidation of low-density lipoprotein (ox-LDL) is believed to play a role in the pathogenesis of atherosclerosis. Recent reports have shown that ox-LDL and low-density lipoprotein receptor 1 (LOX-1) are involved in the pathogenesis of OA. The purpose of this narrative review is to summarize the current understanding of the role of the LOX-1/ox-LDL system in the pathogenesis of OA and to reveal common underlying molecular pathways that are shared by MetS in OA and the LOX-1/ox-LDL system.
Introduction
Osteoarthritis (OA) is a major and common disease with a prevalence that is continuously increasing because of global aging. 1 The number of patients with knee OA in Japan is estimated to be approximately 25 million (ROAD study). 2 Generally, treatment of end-stage OA requires surgery, such as total knee arthroplasty. The medical costs of arthroplasty have been increasing worldwide.3,4 Until recently, conservative and curative treatments for OA have not been determined. Currently, clarifying the cause of OA and developing fundamental treatment strategies are critical.
OA was originally considered to be caused by mechanical stress due to obesity. 5 Therefore, the cause of OA was believed to be mainly wear and tear of chondrocytes by mechanical stress. Interestingly, recent studies have shown that metabolic syndrome (MetS) disorders are involved in the pathogenesis and progression of OA. 6 Some studies have also suggested involvement of lipid peroxidation in the pathogenesis of degeneration of articular cartilage.7–9 Hypercholesterolemia, which causes atherosclerosis (AS), has been reported to be associated with the risk of knee OA 10 independently of obesity. Investigations to clarify the factors and mechanisms underlying AS and OA are currently underway. In this narrative review, we address the evidence underlying the molecular mechanisms of hyperlipidemia and AS in the pathogenesis of OA in detail.
Epidemiology of the association of dyslipidemia and OA
Epidemiological studies have shown that hypercholesterolemia, which is a representative disease of dyslipidemia, is a risk factor of knee and hand OA.11,12 A cross-sectional study also showed a correlation between hypercholesterolemia and knee OA. 13 A case–control study suggested that serum cholesterol was an independent systemic risk factor for OA. 14 Furthermore, a cohort study showed a correlation between high serum cholesterol levels and generalized OA. 15 Oliviero et al. 16 demonstrated that patients with OA have the highest concentrations of apolipoprotein (APO) A-I and total cholesterol compared with controls. Interestingly, Zhang et al. 17 suggested that dyslipidemia is associated with a higher risk of lumbar disc herniation. These authors also suggested that serum lipid levels could be useful predictors of intervertebral disc degradation in a Chinese population. These studies highlight the relationship between dyslipidemia and OA.
Possible involvement of cholesterol in the pathogenesis of OA
Serum levels of low-density lipoprotein (LDL) are elevated in hypercholesterolemia. LDL is a major group of lipoproteins that transport molecules with cholesterol esters in a hydrophilic shell of phospholipids, triglycerides, APO, and free cholesterol. 18
A recent study that used ApoE knockout mice showed that increased synovial inflammation and accelerated ectopic bone spur formation during experimental OA were derived from high LDL levels. 19 Another study showed that elevated LDL levels induced OA-like changes in an inflammatory OA model in mice with a cholesterol-rich diet or LDL receptor deficiency. 20 This study demonstrated that synovial production of pro-inflammatory cytokines was increased in mice with high LDL levels. Furthermore, this study showed that synovial activation was significantly increased in response to high LDL levels. A further study in ApoE knockout mice showed the effects of hypercholesterolemia on progression of OA. 21 Degradative OA symptoms were reported in rats with destabilized knees that were fed a high-cholesterol diet compared with controls. 7 Taken together, these results emphasize the importance of cholesterol in the pathogenesis of OA. The effects of statins on progression of knee or hip OA have been investigated, but the results are conflicting.22,23 Therefore, while there appears to be a relationship between cholesterol and OA, the effectiveness of statin treatment in OA has not been fully determined.
Association between AS and OA
Recent studies have shown that cardiovascular disease and OA also have a clinical relationship. 24 Belen et al.25,26 showed a significant relationship between femoral plaques, carotid intima-media thickness, and hand OA. Cemeroglu et al. 27 also reported a significant relationship between severe coronary stenosis and hand OA. An association between knee OA and the severity of AS was also suggested by Ekim et al. 28 Few cohort studies have demonstrated that hand, knee, and hip OA are associated with AS.29–31 An association between progression of OA and AS has been previously reported.32,33 Some studies have reported that the correlation between OA and AS is more pronounced in female than in male patients.26,29 Recent studies have demonstrated that there is a correlation between AS and cardiovascular disease, 34 and that cardiovascular disease and OA have some common risk factors.24,34
Chronic inflammation and aging are some of the common key factors between AS and OA. 35 “Inflammaging” refers to combined inflammation and aging, and is defined as inflammation according to aging. 36 Inflammaging also refers to chronic inflammation observed histologically. 37 In fact, OA and AS have common molecular mediators that are induced by some inflammatory cytokines. 24
Role of LDL receptor 1 and oxidation of LDL in the pathogenesis of AS
The most likely major contributing factor for the incidence of atherosclerotic lesions is an imbalance between cholesterol influx and efflux within tissues. 38 Transport of cholesterol is regulated by several cell surface receptors, including CD36, ABCA1, and scavenger receptor class B type I. 39 CD36 has been recognized as a binding and internalizing factor in oxidation of low-density lipoprotein (ox-LDL) and a wide range of ligands, such as long-chain fatty acids, apoptotic cells, anionic phospholipids, and other altered LDLs. 40 CD36 also plays a role as a governing scavenger receptor in ox-LDL uptake and recognizes lipid moieties in ox-LDL.
Macrophages and phagocytes perform ox-LDL in the walls of blood vessels. Subsequently, they appear as characteristic foam cells. 41 However, ox-LDL results in endothelial dysfunction.42,43
A receptor of ox-LDL—designated low-density lipoprotein receptor 1 (LOX-1)—was cloned from cultured bovine vascular endothelial cells. 44 LOX-1 has a type II membrane protein structure with a long C-terminal extracellular domain and a short N-terminal cytosolic domain. LOX-1 is also distinct from the types 1 and 2 scavenger receptors, such as CD36 and CD68, respectively. 45 Although the potential role of this receptor in atherogenesis is still unknown, ox-LDL uptake via this receptor, which is expressed in the vascular endothelium, has been suggested to be involved in endothelial dysfunction in atherogenesis. 43 Therefore, LOX-1 and ox-LDL have a crucial role in the pathogenesis of AS caused by hypercholesterolemia.
Evidence for involvement of LOX-1/ox-LDL in OA
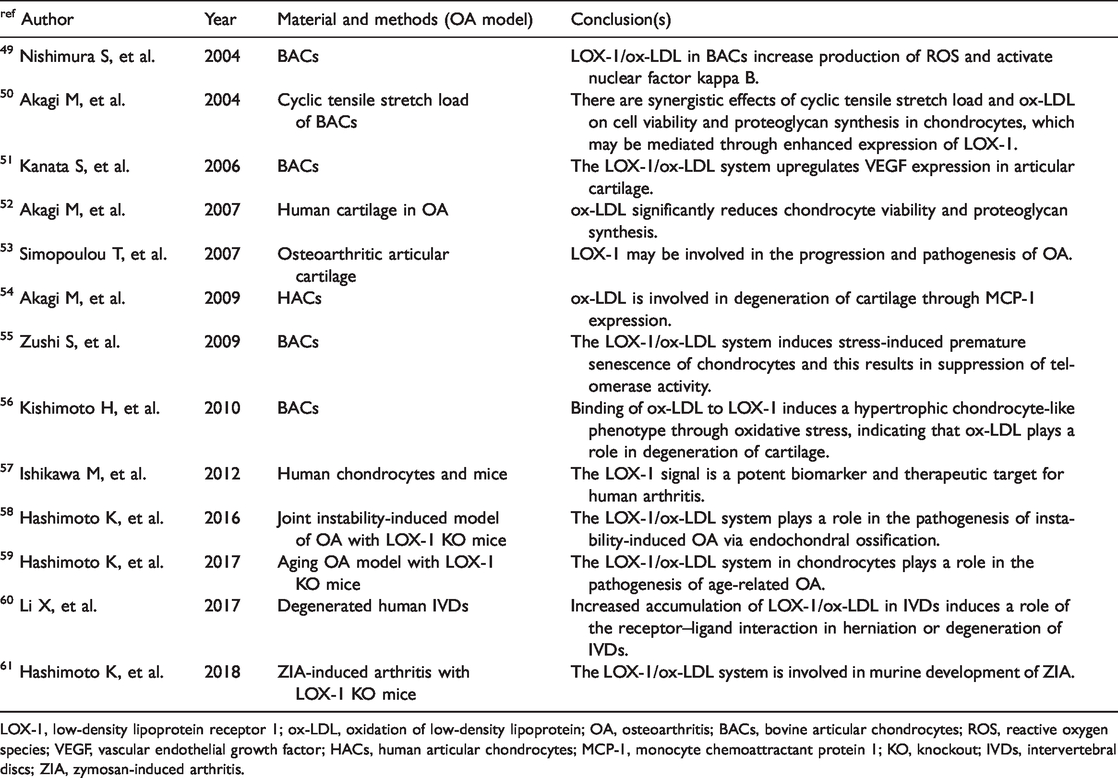
For more than 10 years, several studies have indicated possible involvement of LOX-1/ox-LDL in the pathogenesis of degeneration of cartilage. In their pioneer study, Nakagawa et al. 46 reported LOX-1 expression in articular chondrocytes in a rat arthritis model and the presence of ox-LDL in articular cartilage. Furthermore, these authors found LOX-1 mRNA and protein expression in cultured rat chondrocytes in basal culture conditions and enhanced treatment with interleukin (IL)-1β and ox-LDL. 47 Additionally, ox-LDL dose-dependently reduced viability of chondrocytes, which induced non-apoptotic cell death. 47 These observations suggest that ox-LDL and its receptor LOX-1 are significant regulators of degradation of cartilage. Kakinuma et al. 48 reported ox-LDL in human synovial fluid and expression of LOX-1 and ox-LDL in human rheumatoid arthritis cartilage. Their study was the first to indicate possible involvement of LOX-1 and ox-LDL in synovial fluid. Although these studies indicate possible involvement of the LOX-1/ox-LDL system in degeneration of cartilage, they mainly show that the LOX-1/ox-LDL system is involved in degeneration of cartilage in rheumatoid arthritis and not in OA. We found that ox-LDL binding to LOX-1 increased production of intracellular reactive oxygen species (ROS) in bovine articular chondrocytes (BACs) (Table 1). 49 A novel finding of this study was that ROS induced by the LOX-1/ox-LDL system was involved in the pathogenesis of OA. Additionally, LOX-1/ox-LDL mRNA and protein expression induced by mechanical stress resulted in proteoglycan synthesis and decreased cell viability in BACs. 50 Furthermore, we suggested that binding of ox-LDL with LOX-1 upregulates vascular endothelial growth factor (VEGF) mRNA and protein expression in BACs via activation of peroxisome proliferator-activated receptor (PPAR)-gamma. 51 Our research team, along with Simopoulou et al.,52,53 showed LOX-1 and ox-LDL mRNA and protein expression in human articular chondrocytes. Our findings also suggested that ox-LDL enhanced monocyte chemotactic protein 1 (MCP-1) mRNA and protein expression in human articular chondrocytes and supported the hypothesis that ox-LDL is involved in degeneration of articular cartilage. 54 We also attempted to clarify the role of the LOX-1/ox-LDL system in the pathogenesis of OA induced by aging, and we proposed that the LOX-1/ox-LDL system is involved in premature senescence in chondrocytes by suppressing telomerase activity. 55 In a subsequent study, we clarified that the LOX-1/ox-LDL system promoted a hypertrophic chondrocyte-like phenotype through oxidative stress in cultured BACs. 56 Interestingly, these findings indicate that oxidative stress induced by LOX-1/ox-LDL is involved in the endochondral ossification process in the pathogenesis of OA. However, these findings were based on an in vitro study using BACs or articular human chondrocytes and not on an in vivo study. As a next step, Ishikawa et al. 57 attempted to confirm whether LOX-1 could be considered a biomarker of arthritis using human arthritis chondrocytes and a murine arthritis model. These authors suggested that serum LOX-1 could be a useful biomarker for diagnosis of arthritis and evaluation of disease activity in arthritis. Furthermore, their results indicated that LOX-1 may be a potent therapeutic target for arthritis. However, these findings have more implications for rheumatoid arthritis than for OA. We also recently attempted to clarify the role of the LOX-1/ox-LDL system in the pathogenesis of OA in an in vivo study in mice. We found that LOX-1 knockout mice showed resistance in a murine knee OA model by destabilizing the medial meniscus. 58 This study suggests that the LOX-1/ox-LDL system is involved in the in vivo pathogenesis of OA induced by mechanical stress. In a subsequent in vivo study, we found that the LOX-1/ox-LDL system was involved in the pathogenesis of murine age-related OA via endochondral ossification. 59 Recently, using a zymosan-induced murine arthritis model, we successfully demonstrated that the LOX-1/ox-LDL system was involved in the pathogenesis of inflammatory OA. 60 Therefore, in vitro and in vivo studies indicate involvement of the LOX-1/ox-LDL system in OA. Recently, Xinhua et al. 61 showed possible involvement of the LOX-1/ox-LDL system in pathogenesis and progression of human intervertebral disc degeneration or herniation. These results indicate that the LOX-1/ox-LDL system is strongly involved in the pathogenesis of OA (Table 1, Figure 1). Interestingly, these findings show that the LOX-1/ox-LDL system is involved in OA through oxidative stress.
Effects of LOX-1/ox-LDL interaction in articular chondrocytes.
LOX-1, low-density lipoprotein receptor 1; ox-LDL, oxidation of low-density lipoprotein; OA, osteoarthritis; BACs, bovine articular chondrocytes; ROS, reactive oxygen species; VEGF, vascular endothelial growth factor; HACs, human articular chondrocytes; MCP-1, monocyte chemoattractant protein 1; KO, knockout; IVDs, intervertebral discs; ZIA, zymosan-induced arthritis.

Effects of LOX-1/ox-LDL interaction in articular chondrocytes.
Common molecules between MetS in OA and LOX-1/ox-LDL
OA is associated with hypertension and LOX-1/ox-LDL
Generally, hypertension is a major common component of MetS. One role and mechanism of hypertension in MetS is considered to be impaired bone metabolism due to interrupted blood flow in the subchondral bone, while another mechanism involves apoptosis of osteoblasts.62,63 Recently, we showed that the renin–angiotensin system (RAS) component is expressed in mouse growth plates. 64 We also showed that the local RAS was involved in differentiation of chondrocytes in the ataxia–telangiectasia group D complementing cell line. 65 Furthermore, we found that the Tsukuba spontaneous hypertension mouse model had more severe OA than controlled wild type mice in the forced running model. 66 These findings indicate that the RAS is involved in the pathogenesis of OA. Activation of LOX-1 contributes as a mediator of the RAS system. 67 Angiotensin II mediates vasoconstriction through activation of the angiotensin 1 receptor. The LOX-1 receptor mediates ox-LDL internalization and upregulates angiotensin 1 receptor via the NADPH oxidase, mitogen-activated protein kinase, and nuclear factor kappa B pathways. 68 As positive feedback, angiotensin II upregulates LOX-1 expression.69,70 Therefore, LOX-1 is responsible, at least in part, for physiological and pathological effects via angiotensin II, regulating important functions of this pathway as a normotensive factor, and initiating cardiovascular disease and OA. These findings indicate that angiotensin II (RAS component) is a common factor between OA and LOX-1/ox-LDL associated with hypertension (Table 2).
Common molecules between MetS components and the LOX-1/ox-LDL system.

MeTs, metabolic syndrome; LOX-1, low-density lipoprotein receptor 1; ox-LDL, oxidation of low-density lipoprotein; HT, hypertension; RAS, renin–angiotensin system; HL, hyperlipidemia; LDL, low-density lipoprotein; MCP-1, monocyte chemotactic protein 1; DM, diabetes mellitus; AGEs, advanced glycation end-products; ROS, reactive oxygen species; PPAR-γ: peroxisome proliferator-activated receptor γ.
OA is associated with obesity and LOX-1/Ox-LDL
Although progression of OA is induced by mechanical stress with obesity, obesity also has other systemic effects. “Adipokine” is a generic term for bioactive proteins that are secreted from fat cells. 71 Adipokines are released from adipose tissue subjected to mechanical stress and are inflammatory cytokines, which contribute to degeneration of cartilage. 72 Adipokines include tumor necrosis factor-α, plasminogen activator inhibitor type 1, and heparin-binding epidermal growth factor, which act to promote arteriosclerosis, and leptin and adiponectin, which act prophylactically in arteriosclerosis. 73 Tumor necrosis factor-α is also an inflammatory cytokine that is secreted by macrophages and from large fat cells, and has been reported to contribute to insulin resistance. 74 In the state where visceral fat is accumulated, abnormal secretion of adipokines occurs, and insulin resistance is increased. 75 In particular, MCP-1 is a common adipokine that is involved downstream in the LOX-1/ox-LDL system (Table 2).
OA is associated with diabetes mellitus and LOX-1/ox-LDL
The negative effects of diabetes on joints can be explained by induction of oxidative stress and pro-inflammatory cytokines. 76 Because of the susceptibility to ROS-induced oxidative stress in hyperglycemic conditions, 77 endothelial cells favor production of IL-6 and prostaglandin E2. 78 Catabolism of hyperglycemia in human cartilage is neutralized by the PPAR-γ activator. 79 However, the negative effects caused by diabetes can also be explained by accumulation of aging products in joint tissues that are exposed to chronic high glucose concentrations. Hyperglycemia results in accumulation of advanced glycan end-products (AGEs). 80 AGEs release pro-inflammatory cytokines and destroy the cartilage matrix. Moreover, LOX-1 is thought to be a ligand of AGEs.67,69 Insulin resistance can also damage joint tissue not only because of local insulin resistance of the diabetic synovium, but also owing to systemic low-grade inflammatory conditions associated with obesity and conditions of insulin resistance. 81 Therefore, ROS, AGEs, and PPAR-γ are common factors in the effects of the LOX-1/ox-LDL system and diabetes mellitus in OA (Table 2). Release of common inflammatory cytokines and maintenance of an ROS-induced oxidative status 82 may contribute to progression of OA, which may then contribute to the oxidatively stressed microenvironment present in the articular joint (Figure 2).

Cycle of MetS in OA.
Non-pharmacological treatment in OA
Physical activity
Generally, exercise is important for preventing MetS, such as obesity. Onset and continuation of fatty liver disease may be associated with other aspects of lifestyle. 83 The body mass index, a sedentary lifestyle, loose-fitting clothing, sleep deprivation, and a lower frequency of food intake daily are associated with the presence of non-alcoholic fatty liver disease. Tailored and adapted physical activity can also be used in treatment of MetS and OA as part of a correct and healthy lifestyle to prevent diabetes mellitus. 84 Furthermore, a lifestyle incorporating exercise is an important preventative strategy because glucose derivatives, AGEs, sorbitol, and diacylglycerol promote and involve activation of the inflammatory process. 84 Moderate physical activity may act as a preventive measure for knee OA and synovitis. The knee joint of active people expresses lower inflammatory cytokines, such as Il-1β, IL-6, tumor necrosis factor-α, and matrix metalloproteinase-13, and it expresses higher levels of cytokines that are protective for the synovium, such as IL-4, IL-10, and lubricin. 85 Therefore, moderate physical activity may rescue type B synoviocyte dysfunction at the early stage of OA. 85
Nutrition
A healthy diet is important for preventing MetS. The Mediterranean diet has a protective effect on early OA. 86 A diet enriched by olive tree compounds that are found in extra virgin olive oil and olive leaf extract has a recovery effect for cartilage in the early phase of OA. Vitamin D is also a recommended supplement. 87 Healthy cartilage turnover depends on suitable accessibility of vitamin D. 88 Adequate levels of vitamin D stimulate mature chondrocytes to synthesize the proteoglycan matrix. 89 Deficiency in vitamin D is widely associated with several musculoskeletal diseases. 90 In the young healthy sedentary rat model, vitamin D supplementation with the diet has a favorable effect on articular development of cartilage thickness, joint lubrication, and deposition of extracellular matrix fibers. 91 Additionally, coenzyme Q10 suppresses ox-LDL-induced endothelial oxidative injury by modulation of LOX-1-mediated ROS generation via the AMP‐activated kinase/protein kinase C/NADPH oxidase signaling pathway. 92 The authors speculate that coenzyme Q10 suppresses LOX-1-induced ROS, and then may suppress all reciprocally generated ROS related to MetS.
Future prospects
These studies mentioned above that suggest a relationship between the LOX-1/ox-LDL system and OA have some limitations. First, the direct mechanisms connecting mechanical stress and expression of the LOX-1/ox-LDL system have not been determined. Second, the origin of ox-LDL has not been clarified. Third, whether ox-LDL or LOX-1/ox-LDL double-knockout mice also demonstrate resistance against OA is unclear. Similarly, involvement of the LOX-1/ox-LDL system in the pathogenesis of OA in subchondral bone has not been clarified. The LOX-1 index or soluble LOX-1 has recently attracted attention as a clinical biomarker.92–94 The relationship between the prognosis of OA and the LOX-1 index needs to be investigated in the future.
Conclusions
We reviewed articles that investigated the relationship between OA and AS, especially studies that investigated the LOX-1/ox-LDL system in OA. We also clarified molecules that are common to the underlying pathological mechanisms of MetS and the LOX-1/ox-LDL system. We speculate that there is involvement of the oxidative environment of the joint in inducing OA. Evidence shows a correlation between MetS in OA and the LOX-1/ox-LDL system. Suppressing the environment of the cartilage joint that enhances oxidative stress involving the LOX-1/ox-LDL system, which contributes to MetS in OA, may lead to prevention and suppression of OA. In the future, a potential approach for treatment of OA may involve development of anti-oxidative agents and management of patients, promoting a healthy lifestyle free from factors affecting oxidative stress.
Footnotes
Author contributions
KH: study concept and design; and KH and MA: analysis and interpretation of data. Both authors drafted the manuscript and approved the final version.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.