
Abstract
Objective
To assess ovarian reserve through antral follicle count (AFC) and ovarian volume (OV) determination after decapsulation (stripping technique) or CO2 laser vaporization in the surgical treatment of patients with bilateral ovarian endometriomas.
Methods
This prospective, randomized, blinded, self-controlled pilot study was set in a tertiary university hospital between January 2017 and December 2017, and included consecutive patients with bilateral ovarian endometriomas ≥3 cm. The study was registered with ClinicalTrials.gov under the title ‘Impact on ovarian reserve according to the type of ovarian endometrioma excision: laser versus conventional cystectomy’; NCT 03826355. For each patient, the endometrioma on one side was randomly selected to undergo CO2 laser vaporization and the contralateral endometrioma to undergo laparoscopic decapsulation.
Results
A total of 16 patients were included. There were no statistically significant between-group differences in OV and AFC levels at baseline. At the 6-month follow-up, OV and AFC levels were significantly higher in the laser-treated group versus the stripping technique.
Conclusion
Lower OV and AFC levels following excisional surgery for endometrioma versus CO2 laser vaporization suggest a higher impact on ovarian reserve after the stripping procedure.
Keywords
Introduction
Endometriosis affects 10–20% of women of reproductive age, and may be found in up to 50% of women who have chronic pelvic pain and/or infertility.1,2 Ovarian endometriomas are frequent endometriotic lesions and may be bilateral in almost a third of patients.3,4 Laparoscopic decapsulation (stripping technique) is the gold standard surgical treatment for ovarian endometriomas, 5 although it has been associated with damage to ovarian reserve due to excessive removal of ovarian tissue. 6 In contrast, ablative techniques, such as CO2 laser vaporization, might be better in preserving ovarian reserve and present similar recurrence rates.7,8 Even so, the best surgical option remains controversial and treatment must be patient-tailored.5–7,9 In women wishing to conceive after surgery, appropriate procedure election is crucial, particularly when bilateral endometriomas are present.
A woman’s reproductive potential and/or fertility are indirectly determined by anti-Müllerian hormone levels, antral follicle count (AFC), ovarian volume (OV), and other available surrogate markers.10–12 Although anti-Müllerian hormone has been widely used, it does not allow for the discrimination of ovarian reserve between each ovary. Thus, sonographic markers comparable to anti-Müllerian hormone, such as OV and AFC, that allow assessment of ovarian reserve for each separate ovary are useful, particularly when bilaterality is present.13,14
Several studies have tried to clarify whether excision or ablation surgical technique is better in terms of ovarian preservation.9,12,13,15 Among them, Muzii et al. 12 evaluated ovarian preservation in bilateral endometrioma using a self-controlled study design. Since their conclusions could not be extrapolated to the combined technique using CO2 laser energy, the authors encouraged further studies to compare CO2 laser vaporization or other energy sources with stripping, using ovarian reserve evaluation as the primary outcome. 12 To the best of the present authors’ knowledge, comparison of ovarian reserve following removal of endometrioma using laser CO2 vaporization in one ovary, and cystectomy in the contralateral ovary, has not yet been evaluated. Thus, the aim of the present pilot study was to compare AFC and OV, as surrogate markers of ovarian reserve, between excision and ablation with laser vaporization in the same patient with bilateral endometriomas.
Patients and methods
Study population
Female patients with bilateral ovarian endometriomas were sequentially recruited into this prospective, randomized, blinded, self-controlled pilot study, at the Hospital Clínic of Barcelona, between January 2017 and December 2017. Participation in the study was voluntary, and patients compliant with inclusion/exclusion criteria were included.
Inclusion criteria were: age between 18 and 45 years, bilateral symptomatic endometriomas ≥3 cm, premenopausal status, and pain and/or infertility as indication for surgical treatment. The exclusion criteria were: history of cancer, suspected malignancy, and pre-surgical suspicion, or evidence of, premature ovarian failure. Medical treatment and/or previous ovarian surgery were not classified as exclusion criteria.
This study was approved by the Clinical Research Ethics Committee of the Hospital Clinic de Barcelona, and registered under the clinical trial registry name and number ‘Impact on ovarian reserve according to the type of ovarian endometrioma excision: laser versus conventional cystectomy’ NCT 03826355 (registration date, 01/02/2019). All participants provided written informed consent after being informed of the aims and procedures of the study, and all the procedures were performed in accordance with relevant guidelines and regulations.
Study design
Following study enrolment, patients were allocated to surgery for endometrioma. Treatment allocation was performed by a computer-generated randomization list, and concealed in an opaque, sealed envelope for each enrolled patient, which was opened by a member of the surgical team at the time of surgery. Patients and personnel involved in the study were blinded to treatment allocation, apart from the surgical team. The endometrioma of one side was randomly assigned to treatment with cystectomy, and the contralateral endometrioma was treated with drainage and laser coagulation of the inner lining. The surgery was scheduled irrespective of the menstrual cycle day.
Operative laparoscopy was performed through insertion of a 10-mm umbilical trocar and two or three 5-mm ancillary trocars in the lower abdomen. All interventions were performed by the same team of surgeons (FC and MR) who had a wide experience in both techniques, having performed endometriosis surgical operations ≥2–3 times per week over the preceding 5 years. Standard laparoscopic instruments and 0-degree video laparoscope (Karl Storz GmbH, Tuttlingen, Germany) were used in all procedures. The stripping technique consisted of identifying the cleavage plane, and then the cyst wall was carefully stripped from the healthy surrounding normal ovarian tissue and sent for histologic examination. The laser vaporization procedure consisted of drainage of the cyst content and irrigation and inspection of its inner wall. A biopsy of the cyst wall was sent for routine histologic examination to confirm the diagnosis of endometriosis. The cyst was everted to expose the inner cystic wall completely. Vaporization of the internal wall was performed using an AcuPulse Duo fibre CO2 laser (Lumenis, Yokneam, Israel) in a radial way, starting from the centre to the periphery, at a power density of 12 W/cm2 in the continuous mode. In patients who had deep infiltrating endometriosis, the surgery was completed by excision of these nodules as normal practice.
AFC and OV measurements
Sonographic variables for each ovary were assessed by an expert sonographer (CR), who was blinded to the treatment allocation, and assessments were performed within 30 days prior to surgery, and at 3 and 6 months after surgery. For AFC determination, the total number of antral follicles with a mean diameter of 2–9 mm was counted. Ovarian volume was calculated using the prolate ellipsoid formula (length × width × height × 0.523).
All transvaginal ultrasound examinations were carried out using a microconvex endocavity probe (type RIC5-9, Voluson-V730 Expert; GE Medical systems, Munich, Germany).
Statistical analyses
Statistical analyses were performed using SPSS software, version 20.0 (SPSS Inc., Chicago, IL, USA). Values from quantitative parameters are presented as mean ± SD, or number and percentage. Continuous variables without normal distribution were analysed using Mann–Whitney U-test to compare results between the two treatment groups (stripping or laser), or Wilcoxon test for intragroup comparisons of pre- and post-surgery data. A P value ≤0.05 (two-sided) was considered statistically significant.
Results
Study population characteristics
A total of 16 patients with bilateral endometriomas and indication for surgery were sequentially included in this pilot study (Figure 1). Demographic and clinical data for the patients are summarized in Table 1. The mean age of this study population was 32.13 ± 6.56 years, and the indication for surgery was infertility and/or pain in all cases. Four patients had received previous surgery for endometriosis, two patients due to bilateral endometriomas, one for peritoneal endometriosis and one for a diagnostic laparoscopy conducted at another centre twelve years previously. All women presented with bilateral endometrioma, with a mean cyst size of 56.75 ± 21.89 mm on the left side and 51.12 ± 23.80 mm on the right side. No differences were detected in cyst size between the laser and stripping treatment group at baseline. There were no intraoperative or postoperative complications, and no differences regarding operative duration, blood loss or duration of hospital stay were recorded. Following surgery, pathologic analyses confirmed endometriosis diagnosis and ruled out any malignancies in all patients. Notably, 10 patients (62.5%) showed deep infiltrating endometriosis in the transvaginal ultrasound at baseline.
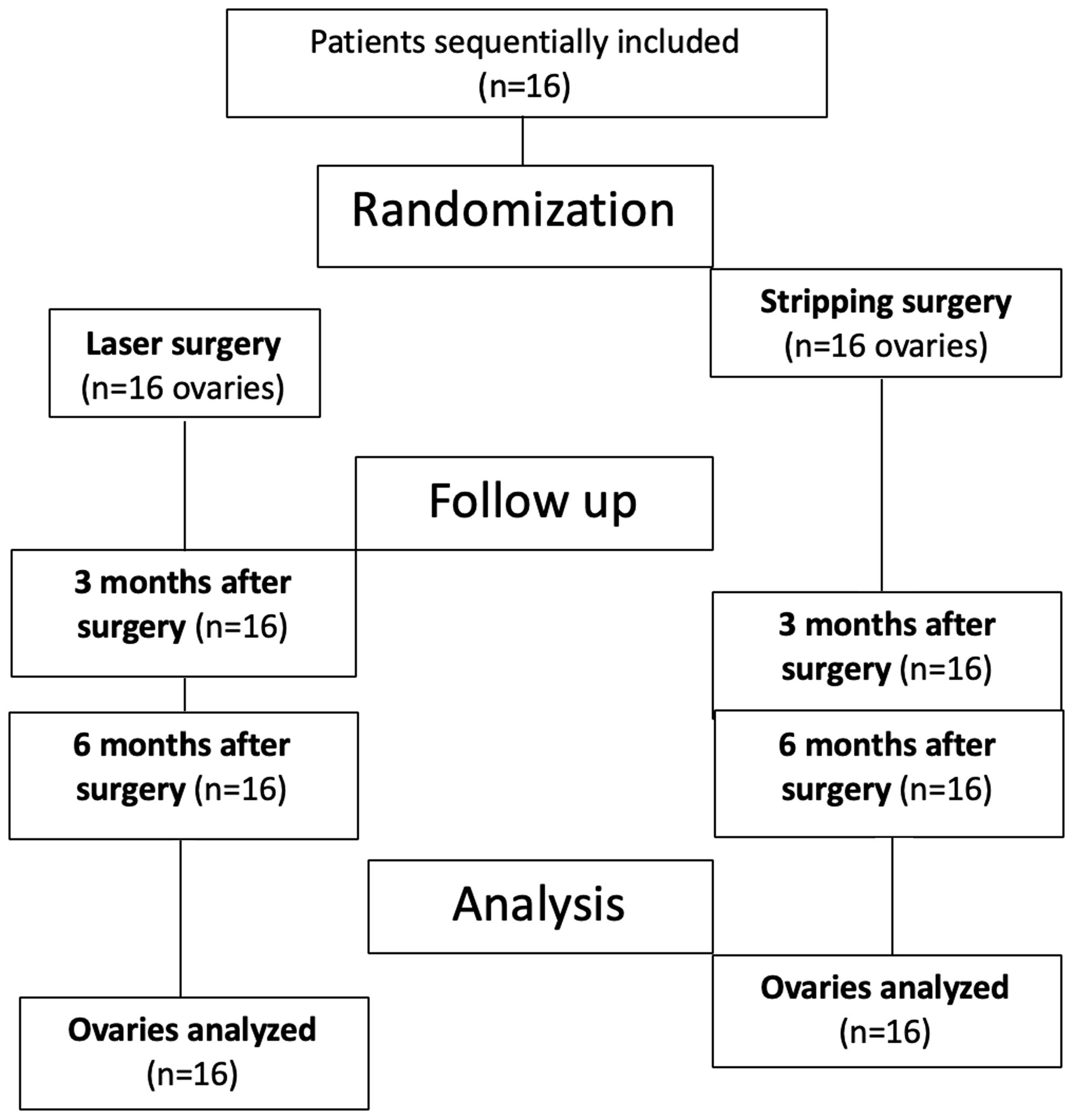
Flow chart of treatments and analyses of patients with bilateral endometriomas included in the study.
Demographic and clinical characteristics of patients with bilateral endometriomas included in the study.

Data presented as mean ± SD or n (%) prevalence.
TVUS, transvaginal ultrasound.
aAge when the first TVUS was performed; bAt least 3 months before the first TVUS exam.
Antral follicle count and ovarian volume
In order to analyse ovarian reserve after removal of ovarian endometriomas, AFC and OV were determined at baseline (30 days prior to surgical treatment), and at 3 and 6 months, following surgery. All patients attended the follow-up visits; thus, no loss of follow-up was recorded. AFC and OV data over time for both groups are presented in Table 2. Mean AFC at baseline was similar between procedures (6.75 ± 4.1 and 6.67 ± 6.3, stripping group versus laser group, respectively). AFC levels were increased in the laser-treated group at 3 months and 6 months post-surgery compared with baseline (P < 0.05), and although not statistically significant, there was a slight numerical decrease in AFC in the stripping group. At the 6-month follow-up, AFC levels were significantly higher in the laser group compared with the stripping group (P = 0.05).
Antral follicle count and ovarian volume at baseline, and at 3 and 6 months, following surgery in patients with bilateral endometriomas.

Data presented as mean ± SD.
AFC, antral follicle count; OV, ovarian volume.
NS, no statistically significant between or within-group difference (P > 0.05).
aBetween-group comparisons (Mann–Whitney U-test); bWithin-group comparisons (Wilcoxon test).
The mean OV for the ovary that was treated using the stripping technique was 98.51 ± 30.9 ml at baseline, and fell to 19.98 ± 3.5 ml at 6 months after the procedure, although this reduction in volume was not found to be statistically significant. The mean OV in the laser-treated group fell from 67.33 ± 16.7 ml at baseline to 27.10 ± 9.1 ml at 6 months after the procedure (P < 0.05 versus baseline). In addition, at the 6-month follow-up, mean OV was significantly higher in the laser-treated group versus the stripping group (P = 0.03). There were no statistically significant differences in OV at baseline or at the 3-month follow-up between the two treatment groups.
Recurrence and pregnancy rates
Patients were followed for up to 6 months, and no recurrence of ovarian endometriomas was found at the end of the study by sonographic follow-up. Nine patients wished to conceive following surgery. The pregnancy rate observed during the 6-month follow-up period was three out of nine patients (33%): one patient was pregnant at the 3-month follow-up, and two further patients were pregnant at the 6-month follow-up. Interestingly, in all three cases, corpus luteum was detected in the ovary subjected to laser surgery.
Discussion
To the best of the authors’ knowledge, this is the first self-controlled study to compare ovarian reserve (AFC and OV) after treatment with CO2 laser vaporization and stripping technique in patients with bilateral endometriomas. By comparing surgical treatment between contralateral ovaries, this pilot study showed that AFC and OV were higher at 6 months after laser ablation for ovarian endometriomas than at 6 months after cystectomy.
Previous studies have stated that cystectomy may damage ovarian reserve due to accidental healthy tissue removal. 6 In contrast, CO2 laser vaporization and other non-excisional techniques have been identified as tissue-sparing procedures.7,8,16 Deleterious tissue removal translates into diminished ovarian reserve correlating with infertility, and has traditionally been determined by anti-Müllerian hormone levels.10,11 Anti-Müllerian hormone is a serum systemic marker and does not allow differentiation of ovarian reserve between each ovary. Thus, in order to discriminate ovarian reserve for each of the ovaries, the present study utilised specific sonographic markers. AFC is a widely-used accurate marker of ovarian reserve, as it has good inter-cycle reliability and inter-observer reliability in experienced centres.17,18 Serum anti-Müllerian hormone levels are well correlated to early AFC measured by ultrasound and also correlate with the pattern of age-related oocyte loss observed histologically. 19 Thus, both anti-Müllerian hormone and AFC are considered the most reliable indirect methods for ovarian reserve assessment.18,20
The present study demonstrated an increase in AFC from baseline to 6 months following laser treatment (from 6.67 ± 6.3 to 9.33 ± 6.2; P < 0.05) and higher AFC levels at the 6-month follow-up in patients treated by laser versus those treated by cystectomy (9.33 ± 6.2 in the laser group versus 4.38 ± 3.3 in the stripping group; P = 0.05). The results concur with previous studies that also reported a significant increase in AFC at 6 months after laser vaporization, but not after stripping.7,15,16 In addition, Ottolina et al. 9 reported that AFC levels are significantly increased as early as 1 and 3 months after CO2 laser vaporization (P = 0.002 and P = 0.005, at 1- and 3-month follow-up, respectively).
An OV ultrasound assessment was also used in the present study to measure the size of the remaining follicular pool, and demonstrated significantly higher OV at 6 months after the laser procedure compared with the stripping technique (P < 0.05). In line with the present results, Var et al. 13 evidenced more frequent decreases in OV and AFC after cystectomy than after coagulation in women with bilateral endometriomas. Compared with cystectomy, other non-excisional techniques, such as plasma energy ablation have also have been identified with statistically significant increases in both OV and AFC.21,22
In the present study, a pregnancy rate of 33.3% was observed at the 6-month follow-up, and in all cases, corpus luteum was detected in the ovary subjected to laser surgery. These results concur with a previous study, in which the response to in vitro fertilization after cystectomy was statistically significantly reduced compared with the response obtained in coagulated ovaries. 13 In addition, a meta-analysis reported a significantly decreased number of mature or dominant follicles and total number of oocytes retrieved in women with endometriomas who had a history of cystectomy. 23
Endometrioma treatment must be personalized and targeted to pain relief, to delay recurrence, and to preserve ovarian function and reserve in women wishing to conceive. 24 It has been suggested that ovarian suspension after endometrioma treatment may improve adhesion formation and thus pain after surgery, 25 although it was not one of the objectives of the present study and no data can be reported regarding this issue. Overall, the post-operative recurrence rate of ovarian endometriomas is high (21.5% at 2 years). 26 Muzii et al. 12 reported comparable rates at 6-months follow-up for ovaries treated with a combined excisional/ablative technique and for the contralateral treated with the stripping technique (5.9% and 2%, respectively, P = 0.62). In agreement with these results, the present study found no recurrences at 6-months follow-up in either treatment group, however, this lack of recurrences may be related to a short follow-up period. Endometrioma size may be one of the decision factors when considering surgical treatment techniques, as reported in a recent study that showed the bigger the endometrioma, the higher the detrimental effect on ovarian reserve, especially if a stripping technique is used. 27 The present study could not confirm these findings, since the study groups were not designed according to endometrioma size.
The main strength of the present study is based on the methodological design. This is the first study comparing stripping and laser vaporization with each patient being their own control. The strict inclusion and exclusion criteria allowed the limitation of additional factors that impact on AFC and OV levels, and sonographer and personnel involved in the study (except from the surgical team) were blinded to treatment allocation. Inadvertent removal of tissue has been shown to correlate with the surgeon’s expertise.28,29 Biases regarding inter-observer and intra-observer variability were avoided because the two different surgical techniques were performed by the same surgical team in a single centre with wide experience in both procedures.
On the other hand, the present study results may be limited by several factors that should be noted. First of all, this was a preliminary pilot study with a small sample size and therefore limited statistical power. The number of patients recruited was small from a biometric point of view, as the study was only intended to be exploratory in nature. However, results coming from such exploratory analyses may be considered for inclusion in larger reviews or meta-analysis. Secondly, as this was a preliminary study, the sample size was decided arbitrarily, but was large enough to detect between-group differences in AFC at 6 months follow-up. Taking into account the results from this study, a sample size of 25 patients (calculated using the OpenEpi website tool from the Centre for Disease Control and Prevention) would have enough power to detect significant differences for future studies. Thirdly, some of the patients included in the study were on hormonal treatment; however, these patients did not discontinue the treatment, thus the results were still comparable during the follow-up period. Finally, four patients had received previous endometriosis surgery. It is reported in the literature that previous surgery may damage ovarian reserve, 30 but only two of the patients had received surgery due to ovarian endometriosis, and they were bilateral endometriomas, thus the impact on the results its low, since each patient was her own control.
In conclusion, CO2 laser treatment for ovarian endometriomas was associated with higher OV and AFC levels than excisional surgery at 6 months following treatment. Lower OV and AFC levels following excisional surgery for endometrioma suggest a higher impact on ovarian reserve. Future directions on research should include larger long-term follow-up studies that simultaneously assess ovarian reserve, as well as fertility and recurrence rates, comparing both surgical techniques (laser and stripping) in contralateral ovaries.
Footnotes
Declaration of conflicting interest
The corresponding author reports a grant from Lumenis to partially finance this study and personal fees as a consultant for Lumenis. All other authors declare that they have no conflicts of interest and nothing to disclose.
Funding
This research received partial grant funding from Lumenis Ltd.