
Abstract
Background
A novel technique of continuous transversus abdominis plane block (TAPB) has been reported to be beneficial to patients undergoing abdominal surgery because it can significantly relieve postoperative pain. The aim of our study is to compare this novel technique with a traditional technique of continuous epidural analgesia (EA).
Methods
We conducted our meta-analysis in accordance with Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. Only randomized controlled trials (RCTs) that compared the efficacy of continuous TAPB and continuous EA to relieve postoperative pain were included. Patients were classified by nationality (Chinese, non-Chinese) for the subgroup analysis.
Results
Nine RCTs with 598 patients were included in our study. Pain levels measured by visual analog scale (VAS) scores at rest on postoperative day 1 were equivalent for continuous TAPB groups and continuous EA groups in non-Chinese and Chinese patients. The TAPB groups experienced a lower rate of hypotension, sensorimotor disorder, and nausea compared with the continuous EA group within 48 hours after surgery.
Conclusion
Continuous TAPB and continuous EA are equally effective in relieving postoperative pain at rest 24 hours after surgery, but EA was associated with more side effects such as hypotension, nausea, and sensorimotor disorder.
Keywords
Introduction
Epidural analgesia (EA) was once one of the most commonly used methods of postoperative analgesia because it resulted in lower visual analog scale (VAS) pain scores and fewer cardiopulmonary complications. 1 Many novel analgesia techniques after surgery are now hot topics such as TAPB and wound infusion of analgesics after surgery. 2 EA is still a commonly used method to relieve postoperative pain, although there is an incidence of inadequate analgesia after surgery, which ranges from 28% to 32%.3,4
Transversus abdominis plane block (TAPB) is a novel local anesthesia technique that provides analgesia to the abdominal wall that was first introduced in 2001. 5 Since then, it has been widely used by anesthetists because it is simple to perform under ultrasound guidance, and it is not associated with some common side effects. 6 However, single-shot TAPB was reported to provide analgesia less than 24 hours after abdominal surgery7–10 and there is only limited evidence showing that single-shot TAPB, alone with multimodal analgesia, was beneficial to relieve postoperative pain.11–15
A recent RCT performed by Kadam and Field 16 showed that continuous TAPB resulted in less rescue analgesic consumption and lower VAS pain scores after abdominal surgery. Niraj et al. 17 showed that intermittent boluses of TAPB resulted in no obvious advantage compared with intermittent boluses of EA after abdominal surgery in 2011. Many studies have been conducted to investigate the efficacy of continuous TAPB for postoperative analgesia compared with continuous EA, but the outcomes remain unclear and controversial.18–21 Thus, we aimed to collect all published studies that reported the comparison of both methods that were used for postoperative analgesia and systematically reviewed them to investigate whether continuous TAPB is better for postoperative pain compared with the traditional gold standard of continuous EA.
Methods and materials
We conducted our systematic review and meta-analysis of efficacy of continuous TAPB with continuous epidural analgesia in patients undergoing abdominal surgery according to the rules of PRISMA. 22 We have registered our study protocol on PROSPERO (CRD number: 42019142824). Because this was a meta-analysis of previously published articles, ethics approval was not required.
Inclusion and exclusion criteria
The inclusion criteria for the articles was as follows: (1) Study is an RCT; (2) investigated the efficacy of continuous TAPB for postoperative analgesia compared with continuous EA; (3) patients were scheduled for elective abdominal surgery with normal coagulation and renal function; and (4) patient age >18 and <85 years. The exclusion criteria were as follows: (1) Study is not an RCT; (2) data could not be extracted; (3) studies including emergency surgeries; (4) contraindications to multimodal analgesia; (5) infection of the puncture site; (6) analgesic dependence; (7) chronic pain; or (8) coagulopathy, major psychiatric illness, or spinal abnormality.
Search strategies and screen of articles
We performed comprehensive searches of PubMed, Cochrane Library, EMBASE, China National Knowledge Network, and Wanfang databases using the key words TAPB, nerve block, abdominal wall block, transversus abdominal wall block, epidural anaesthesia, epidural anesthesia, epidural analgesia, epidural injection, and epidural drug administration. Search strategies differed in different databases, and we present detailed information about the search strategies in the supplementary files. We set a language restriction for English and Chinese, and the last search for studies was completed in July 2019. Searches were re-run just before the final analyses and any further studies that were identified were retrieved for inclusion. Unpublished studies were not be sought.
Initially, our searches identified with 3040 publications, and only 9 studies were included because most of the publications did not meet our inclusion criteria. Two reviewers (Xiangbo Liu and Fei Peng) independently screened all the articles that were located and disagreements were resolved by a third reviewer (Cehua Ou). Detailed information about the study screening is shown in Figure 1.

Flowchart of the article screening process.
Data extraction and risk of bias assessment
The following information was collected from these studies: (1) First authors’ names and publication year; (2) type of surgery and American Society of Anesthesiologists (ASA) status anesthesia methods; (3) numbers of patients (male/female); (4) postoperative analgesia technique; and (5) primary and secondary outcomes of these studies. Characteristics of the included studies are shown in Table 1. The risk of bias was assessed using the review authors’ judgments about each risk of bias item based on the Cochrane Collaboration Risk of Bias Tool. The risk of bias graph and risk of bias summary were presented as follows (Figure 2; Figure 3) . The risk of bias assessment was performed using Review Manager (RevMan) version 5.3.5 (Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014), and the studies were shown to have a high risk of bias regarding blinding of participants and assessors. However, these five studies were also included in a meta-analysis by Baeriswyl et al., 19 who had attempted to contact all the authors of these five studies, and two of them17,21 provided the data requested. Thus, we extracted these data from Baeriswyl et al.’s article directly.
Characteristics of the included studies.

Group T: Patients underwent continuous transversus abdominis plane block; Group E: Patients underwent continuous epidural analgesic.
Group E+T: Patients underwent a single shot of TAPB and continuous epidural analgesic.
TAPB, transversus plane block; PCA, patient-controlled analgesic; PCIA, patient-controlled intravenous analgesic; IV, intravenous; ASA, American Society of Anesthesiologists; BCS: Bruggrmann Comfort Scale.

Risk of bias graph for the included studies.

Risk of bias summary for the included studies.
Outcomes and data synthesis
The primary outcome of our study was the VAS score for pain at rest on postoperative day 1, and the secondary outcomes were the incidence of VAS scores for pain at rest on postoperative day 2, VAS scores for pain at movement on postoperative day 1 and day 2, length of hospital stay, time to ambulation, the incidence of hypotension, nausea, and sensorimotor disorder within 48 hours after surgery. The median and interquartile range were used for mean and standard deviation approximations, as follows: the mean was estimated as being equivalent to the median and the standard deviation was approximated to be the interquartile range divided by 1.35, or the range divided by 4. 23 We also performed a subgroup analysis by classifying patients as Chinese or non-Chinese.
We pooled data from all these studies and calculated the relative risk (RR) and the 95% confidence interval (CI) for all the dichotomous outcomes and weighted mean differences for continuous data using RevMan 5.3. Estimate of RRs and mean differences were performed using a random-effects model, which provides an appropriate estimate of the data with a relatively wide range of CI when the outcomes are statistically heterogeneous. We conducted heterogeneity tests to estimate inconsistencies across all these studies using Q test and I2 test. Publication bias was conducted by using a funnel plot to determine whether there was a bias toward publication. Sensitivity analyses were performed using RevMan 5.3 to estimate any impact of study quality on the outcome.
Results
Among the nine RCTs that were included 17,18,20,21,24–28, two focused on cesarean section surgery,20,24 while the other seven focused on gastrointestinal surgery.17,18,21,25–28 Four studies included Chinese patients20,24–26 and the other five studies included non-Chinese patients.17,18,21,27,28 All authors combined the postoperative analgesia with general anesthesia except for two studies.20,24
For the primary outcome, pain levels measured using VAS scores at rest on postoperative day 1 were equivalent for the continuous TAPB and continuous EA groups in non-Chinese patients (mean difference: 0.53; 95% confidence interval [CI]: −0.37 to 1.42; I2 = 87%) and in Chinese patients (mean difference: −0.06; 95% CI: −0.47 to 0.34; I2 = 88%) (Figure 4). We used a funnel plot to evaluate the publication bias. A slightly nonsymmetrical funnel plot (Figure 5) showed a publication bias may exist. The subgroup analysis cannot account for the existing heterogeneity, while the following sensitivity analysis has shown the source of the heterogeneity. For the secondary outcomes, other side effects related to analgesia techniques or complications after surgery were also assessed carefully and reported as secondary outcomes, which showed that the TAPB group experienced a lower rate of hypotension (relative risk: 0.11; 95% CI: 0.03 to 0.41; I2 = 0%; p = 0 .001), sensorimotor disorder (relative risk: 0.04; 95% CI: 0.01 to 0.23; I2 = 0%; p = 0 .0002), and nausea (relative risk: 0.2; 95% CI: 0.10 to 0.42; I2 = 0%; p < 0 .0001) compared with the continuous EA group within 48 hours after surgery (Figure 6). Other secondary outcomes showed no significant differences between the two groups (Figure 7; Figure 8; Figure 9).
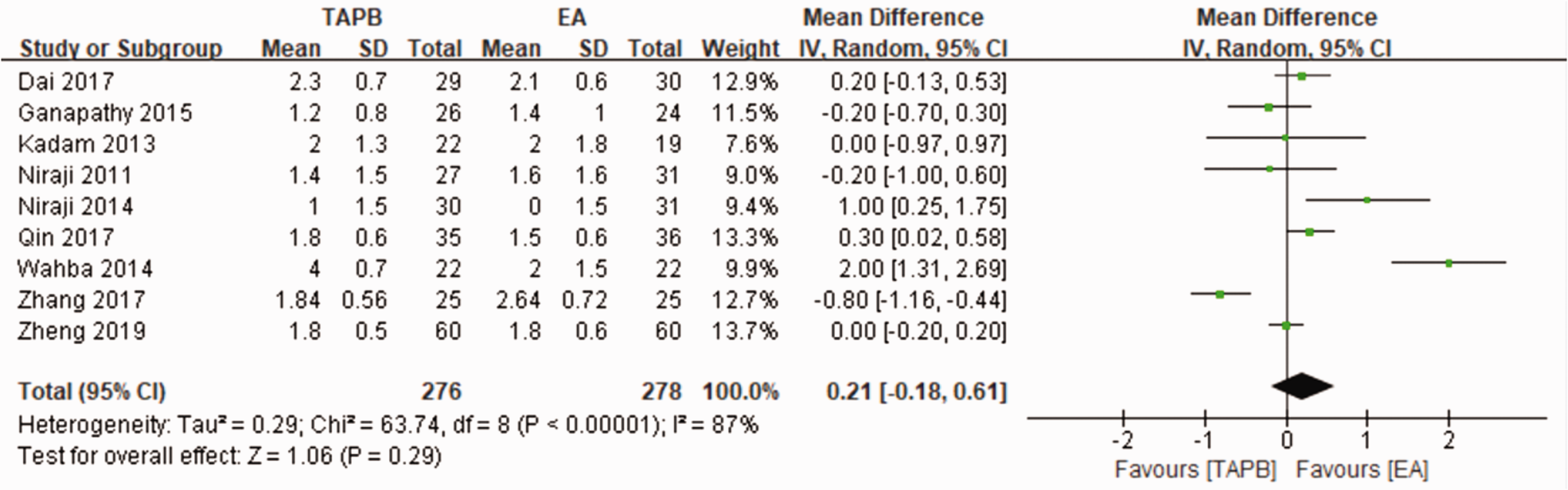
Forest plot of comparison between TAPB and EA for the VAS scores at rest on postoperative day 1.

Funnel plot to evaluate the publication bias.
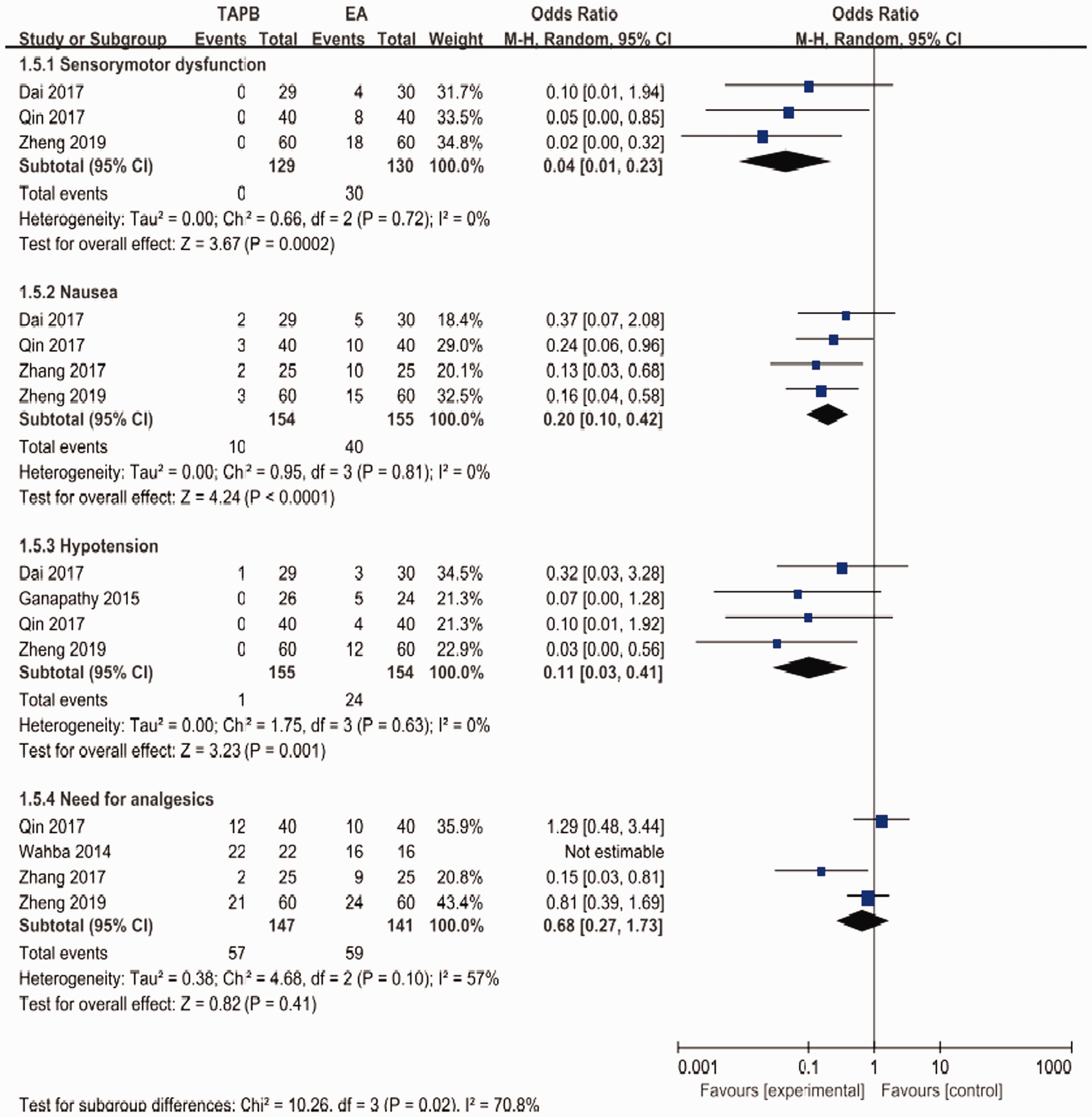
Forest plot to compare between TAPB and EA for sensorimotor dysfunction, nausea, hypotension, and the need for analgesics.

Forest plot to compare between TAPB and EA for VAS scores at rest on postoperative day 2.

Forest plot to compare between TAPB and EA for length of hospital stay and time to ambulation.

Forest plot to compare between TAPB and EA for VAS scores at movement on days 1 and 2.
A sensitivity analysis was performed to investigate the source of the existing heterogeneity. We excluded one or two studies each time and reanalyzed the rest to see whether the I2 change significantly compared with the original analysis. A significant change in I2 was seen when we excluded Wahba and Kamal 28 and Zhang et al., 20 and the result of the primary outcome showed a mean difference of 0.14 (95% CI: −0.08 to 0.35; I2 = 44%) (Figure 10).

Sensitivity analysis for the primary outcome.
Discussion
Kadam and Field 16 showed that continuous TAPB resulted in less rescue analgesic consumption and lower VAS pain scores after abdominal surgery. In 2011, Niraj et al. 17 showed that intermittent TAPB boluses resulted in no obvious advantage compared with intermittent EA boluses after abdominal surgery. Thus, there has been no clear conclusion until now.
Our study systematically analyzed the analgesic efficacy and side effects of continuous TAPB compared with continuous epidural analgesia in patients undergoing abdominal surgery. Based on the nine RCTs with 598 participants, the outcomes showed that both techniques that were used in patients who underwent abdominal surgery were associated with equivalent VAS pain scores at rest or movement on postoperative days 1 and 2, rescue consumption of narcotics, length of hospital stay, and time to ambulation, while side effects related to analgesia techniques such as nausea, hypotension, and sensorimotor disorders were significantly reduced in the continuous TAPB group compared with the EA group. There are several studies that investigated single-shot TAPB and EA for postoperative analgesia, but dynamic analgesia after surgery is a crucial factor for Enhanced Recovery after Surgery (ERAS). 29 Thus, from this point of view, we strongly recommended using continuous TAPB for postoperative analgesia.
Continuous TAPB, which has a safe and effective profile, is widely used to block the anterolateral abdominal wall nerve and the lower intercostals nerve to provide postoperative analgesia for patients. In addition, continuous epidural nerve block produces a continuous analgesic effect by administering local anesthetic continuously into the epidural cavity to block the nerve root. The causes of postoperative hypotension, sensorimotor disorder, and nausea in the two groups were analyzed, which may be related to the continuous amount of local anesthetic and the use of extra analgesic drugs in the two groups. However, there are no techniques without drawbacks. Both techniques have a failure or inadequate analgesia rate of around 30%.4,17 Ultrasound-guided continuous TAPB is always difficult to perform in basic level hospitals while continuous EA has rare but life-threatening complications such as spinal hematoma and damage to the spinal cord. 30 The benefits and risks of both techniques should be weighed under certain conditions, and the technique that is more beneficial to the patients should be chosen.
It should be emphasized that there are inconsistencies between the included studies, which contributed to the existing heterogeneity. For the different anesthetic techniques, patients’ conditions, and surgery types, these factors all increased the heterogeneity, which we cannot control.
Limitations
There were some limitations in our study. First, the total number of patients in these nine RCTs is relatively small, but the clear and practical search strategies for comprehensive searches of five official databases, definite inclusion and exclusion criteria, and rigorous consideration of data may compensate for this limitation. Second, the existing publication bias may be a threat to the quality of our meta-analysis. Third, some observational indexes, such as time to first bowel sound and time to passing flatus, are also important factors that may impact the patients’ prognosis, but only a few articles on postoperative analgesia have reported these observational indexes among patients with continuous TAPB and continuous EA. Thus, further studies should focus on these observational indexes. Fourth, when we performed our study, we wanted to complete a subgroup analysis based on different medications that were used in different studies. However, we found that the medications for TAPB and EA were different among the included studies, and thus, we could not perform this subgroup analysis. The use of different medications may have resulted from the physicians’ personal preferences. Fifth, the type and amount of postoperative opioid consumption is an important parameter because it may also have an impact on the VAS score, and we thought about this question when we were performing our study. However, we found that the opioids that were consumed postoperatively varied significantly among different studies because of the different types of surgery or possibly because of the physicians’ personal preferences. For example, we included studies that reported about patients who underwent cesarean section and laparoscopic surgery, and the postoperative pain level is likely different among patients who underwent these two types of surgery. Thus, opioid consumption after surgery was significantly different.
Conclusion
The results of this meta-analysis showed that both continuous TAPB and continuous EA could provide equivalent analgesia in patients after abdominal surgery. Because patients in the continuous TAPB group experienced a lower rate of hypotension, sensorimotor disorder, and nausea within 48 hours after abdominal surgery, we recommend the continuous TAPB technique for postoperative analgesia after abdominal surgery, if possible.
Footnotes
Acknowledgements
We thank Xiangbo Liu and Fei Peng for screening the articles, data synthesis, and data collection; Xiangbo Liu, Fei Peng, and Guo Mu for their assistance with the study design and preparing the primary manuscript; and Cehua Ou for his funding support and help with editing this article.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
Our study was supported by the Foundation of Health Commission of SiChuan Province (16PJ567).