
Abstract
Nasal chondromesenchymal hamartoma (NCMH) is a rare destructive benign neoplasm that predominantly develops in infants and young children. The lesion is usually located in the nasal cavity, often in the adjacent paranasal sinuses and orbital region and especially in the ethmoid sinus. Because the imaging characteristics of NCMH often mimic the features of malignant tumors, it is clinically important to study the radiographic appearance of this disease. Therefore, we herein present the computed tomography and magnetic resonance imaging findings of NCMH occurring in a 7-year-old girl. The mass was resected via an endoscopic surgical approach and definitively diagnosed as NCMH based on histologic and immunohistochemical analysis. However, signs of tumor recurrence manifested 45 months after surgery. NCMH can be locally aggressive with an expansive and destructive radiographic appearance, which highly implies a malignant neoplasm. Hence, an accurate diagnosis is essential to avoid potentially harmful therapies, and detailed computed tomography or magnetic resonance imaging should be performed prior to surgery. Selective arterial embolization is also an important part of preoperative management because the degree of enhancement may not be adequate to determine the blood supply of the tumor. Moreover, complete radical excision cannot guarantee that the lesion will not recur.
Introduction
In 1998, McDermott et al. 1 first described a lesion termed nasal chondromesenchymal hamartoma (NCMH), which has histopathological characteristics typical of those of thoracic wall interstitial hamartoma. This tumor mainly manifests as polyposis lesions and is primarily located in the nose and nasal sinuses. Most patients with NCMH are infants and toddlers. 1 Because the vast majority of cases are diagnosed at a young age, the lesion is considered to be congenital and principally consists of chondroid or cartilaginous tissues and mesenchymal elements. 1 The imaging features of NCMH are similar to those of malignancies. In the present case, the tumor showed mild enhancement on imaging studies, although an abundant blood supply was confirmed. Therefore, selective arterial embolization may play an important role in surgical management.
Case report
A 7-year-old girl presented with an approximately 2-week history of nasal obstruction and epistaxis. An otolaryngologic evaluation revealed a large intranasal mass. The patient was referred to our otolaryngology department because the nasal tumor became hemorrhagic upon performance of a biopsy. No palpable cervical lymphadenopathy was identified. Nasal endoscopy revealed a large polypoid mass obstructing the right nasal cavity, and a subsequent computed tomography (CT) examination showed a heterogeneous soft tissue mass with an ambiguous border and irregular contour. The CT scan also indicated evidence of focal plaque-like or zonary amorphous calcification (Figure 1). Intravenous administration of contrast medium resulted in significant marginal enhancement without prominent hypervascular enhancement in the rest of the mass. We performed magnetic resonance imaging (MRI) to further characterize the internal architecture. The MRI results indicated that the signal intensity of the mass was heterogeneous on T1-weighted imaging (T1WI) and T2-weighted imaging (T2WI), the signal intensity on T1WI was lower, and T2WI showed heterogeneous hyperintensity. Streak calcification captured by short T1 and short T2 signals was detected within the lesion, and the high signal intensity in some areas on T2WI indicated cystic changes (Figure 2). Additionally, the diffusion limitation was not significant on diffusion-weighted imaging. The tumor involved the right ethmoid sinus, and the accompanying compression of the opening of the right maxillary sinus had led to extensive opacity, resulting in obstructive inflammation. The remaining paranasal sinuses were not invaded. The nasal septum was deviated to the left side, and the right nasal cavity was dilated. Bone defects were found in the right medial orbital wall, medial wall of the maxillary sinus, and cribriform plate (Figure 3). The right medial rectus muscle and lower rectus appeared to be pushed laterally by the mass, causing slight ocular protrusion, but no visible intraocular or intracranial expansion was present.

Computed tomography scan indicated evidence of focal plaque-like or zonary amorphous calcification.

T2-weighted magnetic resonance imaging showed several areas of high signal intensity inside of the mass, which may indicated cystic change.

Bone defects in the right medial orbital wall, medial wall of the maxillary sinus, and cribriform plate.
Surgical excision was recommended. Although the lesion showed poor vascularization radiologically, we hypothesized that it had a rich blood supply because of its significant bleeding tendency during the previous biopsy. Additionally, angiography of the right maxillary artery had shown vessel tortuosity and dilatation. Therefore, preoperative embolization of a branch artery of the right maxillary artery was performed to reduce the perioperative blood loss, shorten the operation time, and facilitate complete mass removal. The procedure was thus less risky and enabled safer surgical resection. The patient underwent endoscopic sinus surgery, which revealed a pink-tan brittle soft tissue mass that was resected in a piecemeal manner. No evidence of orbit or skull base invasion was found. The patient was treated with an adrenaline-soaked cotton slice before surgery and nasal packing with Vaseline gauze postoperatively. About 100 mL of intraoperative bleeding was observed, and complete resection of the tumor was achieved successfully. The mass was submitted for further histological examination and was confirmed to be NCMH.
The total specimen was composed of grayish brown soft tissue, measured 4.0 × 3.5 × 1.0 cm in aggregate, and was characterized by a mixture of various mesenchymal elements. Chondromyxoid and hyalinized nodules were submerged in the background of a mucus-like spindle cell matrix, and chondroid differentiation was predominant (Figure 4). Immunohistochemical studies showed that the mesenchymal-stromal spindle cells demonstrated strong immunoreactivity for vimentin, and S-100 immunoreactivity was evident in the lobules of mature cartilage and scattered stromal cells.
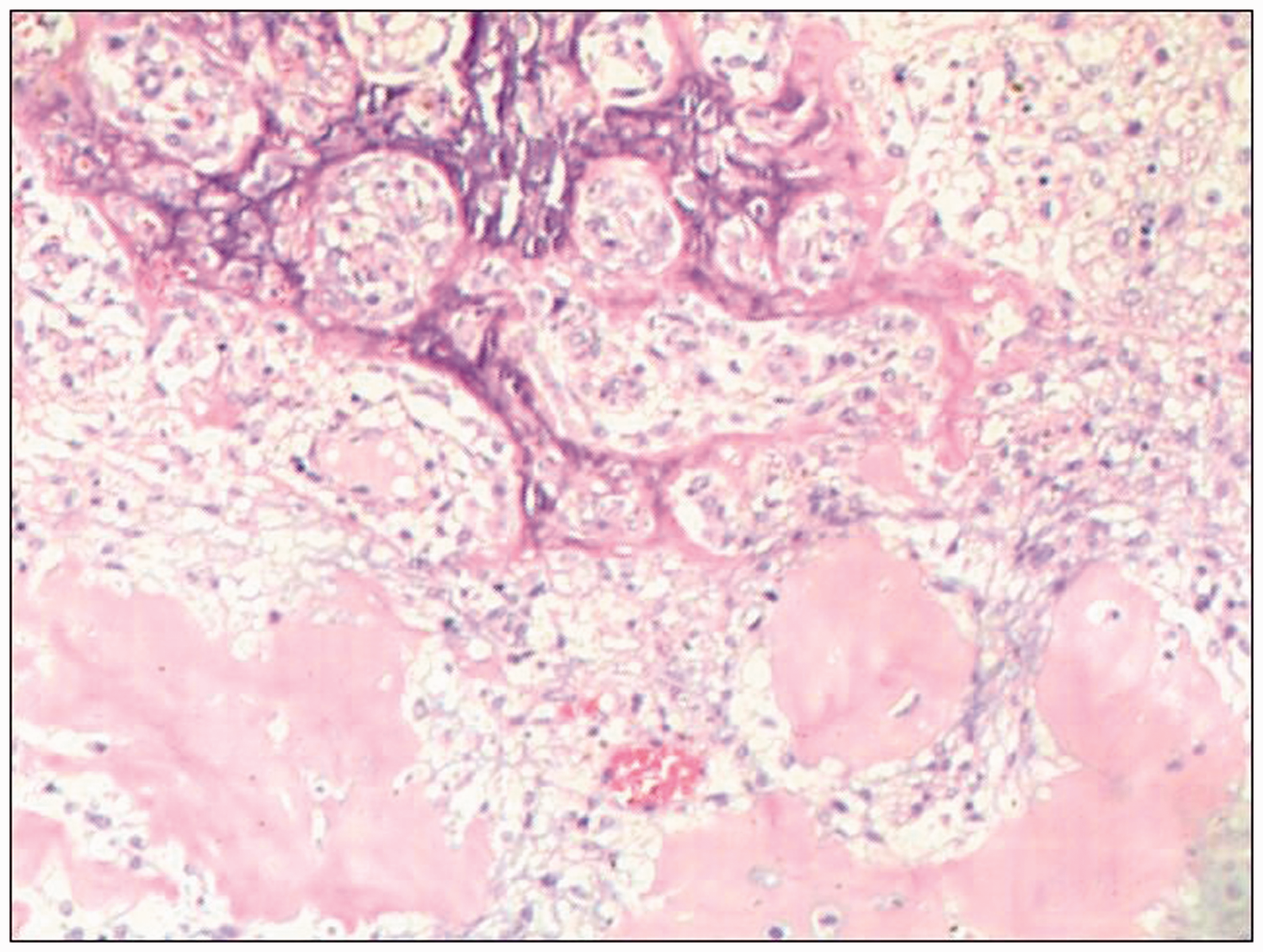
The specimen was characterized by a mixture of various mesenchymal elements, chondromyxoid and hyalinized nodules were submerged in the background of a mucus-like spindle cell matrix.
The patient did well postoperatively and was discharged from the hospital on postoperative day 12. However, clinical and radiologic examinations showed recurrence after 45 months. All procedures performed were in accordance with the ethical standards of the institutional and national research committee. Written informed consent was obtained from the patient’s parent for publication of this case report and its accompanying images.
Discussion
According to the literature, the average age of patients with NCMH is 9.6 years. 2 It is a rare lesion with typical histological, clinical, and imaging features, but the exact etiology and pathogenesis remain unclear. Hamartomas are benign and self-limited lesions; thus, NCMH is considered a benign entity. To date, the only reported case of malignant transformation of NCMH in an adult was published in 2013. 3 The most commonly reported symptoms and clinical manifestations are correlated with the location and size of the tumor and include breast-feeding difficulty, nasal obstruction, epistaxis, rhinorrhea, and middle ear effusion. Additionally, involvement of the orbit or cranial cavity may cause exophthalmos or enophthalmos, oculomotor disorders, and neurological dysfunction. 4 Although NCMH is a benign tumor, it can be misdiagnosed as a malignancy because of its locally destructive appearance. 2
Among the available diagnostic imaging techniques, radiological assessment with CT or MRI is the preferred method. Although CT and MRI cannot provide comprehensive information regarding the mass, they are helpful for characterization of the anatomic extent and invasion of the lesion as well as localization of its site of origin. The true degree of the lesion and its relationship with and effect on surrounding structures provide more helpful information for planning the nasal endoscopy procedure and resection technique. 5 , 6 The imaging findings reflect the underlying pathology. Imaging typically reveals NCMH as a nonencapsulated mass with a poorly defined boundary containing both solid and cystic components. Calcifications are frequently observed on CT or MRI. 7 , 8 Moreover, the degree of contrast enhancement is proportional to the degree of tumor vascularity. 5 In our case, the mass contained multiple internal foci of calcifications and cystic components. It also showed a destructive pattern on imaging, which may arouse suspicion for a malignant neoplasm. Although the tumor had a rich blood supply, it showed less enhancement than common cases of NCMH.
CT can show destruction and pressure remodeling of bone and coarse calcification of the inner focal length of adjacent bone. However, CT may show poor-quality images in newborns and young children because the bone of their skull base is thin. MRI of NCMH demonstrates a heterogeneous signal intensity on T1WI and T2WI, and the contrast enhancement is significantly heterogeneous. 9 , 10 MRI is particularly helpful in evaluating intracranial extension, considering that the bony plate of very young children is movable and their skull is not yet completely ossified. In addition, when orbital extension is present, MRI is superior to CT in assessing whether the tumor has invaded the intraorbital contents, including the extraocular muscles, optic nerve, and eyeball. MRI is much safer than CT and is being increasingly used for detailed evaluation of pediatric sinonasal masses. 11 Furthermore, MRI has more advantages in differential diagnosis, and it is the preferred imaging tool for investigation of suspected sinonasal masses. In short, NCMH can be locally aggressive with an expansive, destructive radiographic appearance, and it tends to invade most of the surrounding tissues, which highly implies a malignant neoplasm. Hence, an accurate diagnosis is essential to avoid potentially harmful therapies. 8
The list of differential diagnoses based on radiological imaging of NCMH is relatively long because all entities are rare. Many benign pediatric tumors have imaging features that can mimic NCMH, such as hemangioma, angiofibroma, nasal glioma, inverted papilloma, giant cell reparative granuloma, ossifying fibroma, and chondro-osseous respiratory adenomatoid hamartoma. Malignant pediatric tumors such as rhabdomyosarcoma, esthesioneuroblastoma, and chondrosarcoma should be excluded, with the latter two usually seen in adolescence. All of these potential tumors should be considered as differential diagnoses. 12 The initial diagnosis of NCMH can be difficult or mistaken by radiography, and the definitive diagnosis mainly depends on histopathologic analysis.
NCMH can be easily debulked via endonasal endoscopic surgery without significant intraoperative hemorrhage. 13 In our case, the blood loss of 100 mL was not negligible during removal of a nasal tumor in a young girl who had undergone preoperative embolization. Complete surgical resection is curative, and there is no need for adjuvant radiotherapy or chemotherapy. 14 However, our patient developed tumor relapse 45 months after surgery, indicating that radical excision cannot absolutely guarantee that the lesion will not recur.
Mutations of the DICER1 gene, which is located on the long arm of chromosome 14, region q32.13, can lead to cancerous and non-cancerous tumors as well as a range of rather rare neoplasms, including NCMH, pleuropulmonary blastoma, and ovarian Sertoli–Leydig cell tumor. 15 Pathogenic germline and somatic mutations of the DICER1 gene imply that NCMH appears to be biologically associated with pleuropulmonary blastoma. 16 A genetic pedigree survey showed that our patient’s family was negative for NCMH and other cancers proven to be related to mutation of the DICER1 gene.
CT and MRI are two dominant complementary radiological techniques that can help to determine the texture of the mass and aid in planning surgical resection. Therefore, performing a detailed CT or, preferably, MRI examination prior to surgical excision is essential.
In conclusion, we have herein reported the CT and MRI features of an NCMH, which is a rare benign hamartoma that generally presents in pediatric patients. Because the imaging features of NCMH are similar to those of malignancies, the recognition and initial accurate diagnosis of this entity is imperative to avoid misdiagnosing it as a malignancy and potentially implementing harmful therapies. Although the case of NCMH described herein was hypervascular, the tumor demonstrated only mild enhancement on imaging. Our research strongly suggests that superselective arterial embolization may play an important role in preoperative management.
Abbreviations
NCMH: nasal chondromesenchymal hamartoma
CT: computed tomography
MRI: magnetic resonance imaging
T1WI: T1-weighted imaging
T2WI: T2-weighted imaging
Footnotes
Acknowledgement
Dr. Gang Huang is the scientific guarantor of this publication.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Ethical approval
This study was approved by the Ethics Committee of Gansu Provincial Hospital (No. 2019-086).
Funding
This study was supported by a grant from the Gansu Provincial Hospital of China (No. 16GSSY1-7).