
Abstract
Objectives
To investigate the clinical efficacy and mechanism of Jianpi Huatan Tongfu granule in treating acute exacerbation of chronic obstructive pulmonary disease (AECOPD).
Methods
Sixty patients with AECOPD were enrolled in either of two groups: integrative treatment (Western medicine combined with Jianpi Huatan Tongfu granule) (n = 30) and Western medical treatment (n = 30). Thirty healthy individuals were included in the control group.
Results
Compared with healthy participants, patients with AECOPD had elevated clinical symptom and dyspnea severity scores. Patients with AECOPD had worsened lung function, compared with healthy participants. The therapeutic efficacy for integrative treatment was superior to Western medical treatment. Inflammatory proteins and cytokines were significantly elevated in patients with AECOPD, including C-reactive protein, interleukin-6, interleukin-8, and tumor necrosis factor-α; these were alleviated by both treatments, with more obvious effects for integrative treatment. Integrative treatment significantly changed the intestinal flora in patients with AECOPD, reaching levels comparable with those of healthy participants. Firmicutes abundance was significantly higher in healthy participants, whereas Bacteroidetes abundance was significantly higher in patients with AECOPD. After treatment, Verrucomicrobia abundance was significantly reduced in patients with AECOPD.
Conclusion
Jianpi Huatan Tongfu granule could alleviate inflammatory responses and improve clinical therapeutic efficacy in patients with AECOPD.
Keywords
Introduction
Chronic obstructive pulmonary disease (COPD) is a common respiratory disease characterized by airflow limitation, which can be managed clinically. 1 Acute exacerbation of chronic obstructive pulmonary disease (AECOPD) comprises rapid deterioration of COPD. 2 Kelly et al. 3 reported that the hospital mortality rate was approximately 4% for patients with AECOPD; for 91% of these patients, the primary disease was COPD. Notably, patients with AECOPD have a high admission rate; the disease often rapidly progresses after admission, accompanied by a high hospital mortality rate. 4
Treatments for AECOPD currently focus on disease symptoms, 5 but have various disadvantages; therefore, additional treatments for AECOPD are urgently needed. Improvement of gastrointestinal microbiota has been shown to reduce inflammatory responses, 6 which is effective treatment for inflammatory bowel diseases. 7 Traditional Chinese medicine (TCM) considers the lung and large intestine to be exterior and interior; therefore, lung diseases are presumably closely related to intestinal injuries. 8 Imbalances in intestinal flora and microecological internal environment are reportedly related to the pathological progression and disease severity of COPD. 9 Altered intestinal flora may be associated with the pathogenesis of inflammatory diseases; affected patients have increased proportions of Firmicutes and Proteobacteria. 10 For patients with AECOPD, TCM may reduce side effects and improve treatment efficacy through adjustments to intestinal flora, maintenance of intestinal microecological balance, and improvement of systemic immune function.
TCM exhibits potentially beneficial effects in treatment of AECOPD. 11 TCM has also been shown to regulate intestinal flora composition, protect intestinal mucosal barrier function, and restore intestinal flora homeostasis. 12 Based on clinical experience and traditional TCM theory, we created the Jianpi Huatan Tongfu (i.e., “spleen strengthening, phlegm removing, and bowel relaxing”) granule for disease treatment. Spleen-qi strengthening eliminates the overall source of phlegm, with temporary support by lung-qi dispersion and phlegm removal. 13 The Jianpi Huatan Tongfu granule has been used in clinical treatment of AECOPD. In our experience, compared with the traditional TCM decoction, the Jianpi Huatan Tongfu granule has a good curative effect, as its administration method and flavor facilitate patient compliance. However, its underlying mechanisms have not yet been elucidated.
In this study, considering the high incidence and economic cost of AECOPD, which greatly affect quality of life, 14 affected patients were treated with the Jianpi Huatan Tongfu granule to relieve inflammatory responses and improve intestinal flora. We investigated the mechanism by which TCM affects AECOPD. Specifically, we assessed whether the Jianpi Huatan Tongfu granule acted through a mechanism involving the lung and large intestine.
Material and methods
Study participants
The study protocol was approved by the Ethics Committee of the Affiliated Hospital of Gansu University of Traditional Chinese Medicine, and written informed consent was obtained from each participant for enrollment in the study. Patients with AECOPD, who were admitted to our hospital from January 2017 to December 2017, were included in this study. In accordance with Western medical diagnostic criteria, AECOPD was diagnosed based on the 2017 Chinese Expert Consensus on AECOPD, as clinical grade I or II. 15 For the TCM diagnosis, AECOPD was diagnosed as lung distension (i.e., “phlegm blocking in lung”), based on the Traditional Chinese Medicine Diagnostics 16 and the Traditional Chinese Medicine Diagnosis and Treatment Guidelines (TCM Syndrome Part). 17 Briefly, the main symptoms included coughing, white phlegm, wheezing, and sensation of oppressed breathing; secondary symptoms included abdominal distension, fatigue, limb edema, gastric cavity and chest-abdomen fullness, and loose stool. Furthermore, the tongue color was dark, with thin and whitish fur (or thin and dirty), and the pulse was smooth. Patients who exhibited the main symptoms, together with ≥3 secondary symptoms, combined with the tongue and pulse diagnosis results, were diagnosed with AECOPD (i.e., “spleen deficiency and phlegm dampness syndrome”).
Inclusion criteria for patients with AECOPD were as follows: (1) age 50 to 80 years; (2) fulfillment of Western medical diagnostic criteria for AECOPD; (3) fulfillment of TCM diagnostic criteria for AECOPD; and (4) agreement to receive treatment and provide written informed consent. Exclusion criteria were as follows: (1) pregnancy or lactation; (2) presence of other serious lung diseases; (3) presence of cancers; (4) presence of severe heart disease, cerebrovascular disease, or near-death status; (5) presence of mental illness or severe neurological dysfunction; (6) violation of dosage regimen; (7) presence of TCM syndromes other than spleen deficiency and phlegm dampness syndrome; (8) presence of infectious diarrhea; and/or (9) poor compliance, allergic reaction, serious adverse reactions/complications during treatment, failure to complete the trail, or loss to follow-up.
Inclusion criteria for healthy individuals were as follows: (1) age 50 to 80 years; (2) ratio of half men and half women; (3) agreement to participate in experiments and provide written informed consent. Exclusion criteria were as follows: (1) pregnancy or lactation; (2) presence of COPD and/or other serious lung diseases; (3) presence of cancer; (4) presence of severe heart disease, cerebrovascular disease, or near-death status; (5) presence of mental illness or severe neurological dysfunction; (6) presence of infectious diarrhea; and/or (7) loss to follow-up.
Patients who fulfilled the Western medical and TCM diagnostic criteria for AECOPD were screened and randomly divided into two groups of equal size: integrative treatment (Western medical treatment combined with Jianpi Huatan Tongfu granule) and Western medical treatment. Healthy individuals were included in the control group.
Intervention methods
In the Western medical treatment group, patients received routine Western medical treatment. In the integrative treatment group, patients received routine Western medical treatment, combined with the Jianpi Huatan Tongfu granule. Routine Western medical treatment was performed in accordance with the 2017 Chinese Expert Consensus on AECOPD. 15 Briefly, while receiving controlled oxygen therapy, patients were treated with antibiotics appropriate for the patient’s acute exacerbation symptoms and local drug resistance; bronchodilators or glucocorticoids were also used for treatment of active complications. TCM treatment comprised the Jianpi Huatan Tongfu granule, which contained 15 g Rhizoma Pinelliae Preparata, 12 g Atractylodes rhizome, 30 g Atractylodes macrocephala, 20 g Poria cocos, 9 g Semen Arecae Preparata, 15 g Semen Raphani (stir-fried), 9 g Radix et Rhizoma Rhei (stir-fried with wine), 9 g balloon flower root, 15 g Thunberg fritillary bulb, 9 g Tomentose pummelo peel, 9 g honey-fried ephedra, 6 g leech, 9 g amomum villosum, 6 g common ginger, and 6 g liquorice root. All components were boiled and stirred in 250 mL boiling water; patients were instructed to ingest the Jianpi Huatan Tongfu granule twice per day. All Jianpi Huatan Tongfu granules were delivered with the intelligent formula granule (Efong Pharmaceutical Co., Ltd., Guangzhou, China). During the treatment period, patients were not permitted to smoke or drink alcohol; other cough and phlegm-relieving medicines were also forbidden, as well as other incompatible drugs (e.g., aconite, Radix Knoxiae, and Flos Genkwa). All prescription granule and western medicine preparations used during treatment were from the Department of Pharmacy, the Affiliated Hospital of Gansu University of Traditional Chinese Medicine. Both patient groups received 10 days of treatment. Participants in the control group received no treatment.
TCM clinical symptom severity grading
In accordance with the Guidelines for Clinical Research of New Drugs in Traditional Chinese Medicine, 10 based on the disease symptoms and the treating physician’s clinical experience, the following symptoms were assessed: coughing, expectoration, wheezing and sensation of oppressed breathing, abdominal distension, fatigue, limb edema, gastric cavity and chest-abdomen fullness, and loose stool. These symptoms were used to construct a TCM clinical symptom severity scoring system (Table 1). Therapeutic efficacy criteria are shown in Table 2.
Traditional Chinese medicine-based clinical symptom severity scoring.

Therapeutic efficacy criteria.

Note: Total efficacy included clinically controlled, as well as obviously effective and effective outcomes. Formula: Efficacy = [(Scorebefore–Scoreafter)/Scorebefore] × 100%.
Dyspnea severity grading
Dyspnea severity was assessed in accordance with the modified Medical Research Council Respiratory Questionnaire in the COPD Guide (Table 3). 15 Dyspnea severity scores comprised the following four grades: 0, 1, 2, 3 and 4 points (Table 3).
Dyspnea severity scoring.
Arterial blood-gas analysis
For blood-gas detection, arterial blood samples were obtained from all patients and healthy participants in the morning, under fasting conditions. Blood-gas analysis was conducted with using an ABL800 arterial blood-gas analyzer (Radiometer, Copenhagen, Denmark). Partial pressure of oxygen (PaO2) and partial pressure of carbon dioxide (PaCO2) levels were assessed in arterial blood samples. Patients from the integrative treatment and Western medical treatment groups underwent blood-gas analysis, both at admission and after 10 days of treatment; these results were compared with those of the control group.
Lung function detection
Lung function was detected with the MasterScreen PFT system (Vyaire Medical GmbH, Höchberg, Germany) in our department. After 10 days of treatment, patients underwent assessment of lung function (percent predicted forced expiratory volume in 1 second [FEV1%pred], ratio of forced expiratory volume in 1 second to forced vital capacity [FEV1/FVC], and forced vital capacity [FVC]); results were compared with lung function in the control group.
Detection of CRP, IL-6, IL-8, TNF-α, and procalcitonin levels
Venous blood (4–5 mL) was collected after patients had fasted overnight. Serum was isolated from blood by centrifugation. The serum levels of C-reactive protein (CRP), interleukin (IL)-6, IL-8, and tumor necrosis factor (TNF)-α were detected with enzyme-linked immunosorbent assay kits (Kemei Dongya Biotech, Beijing, China) using a Cobase automatic electrochemical luminometer (Roche, Basel, Switzerland). The procalcitonin level was assessed with a Procalcitonin Kit (Roche). Assessments were conducted, both at admission and after 10 days of treatment, for patients in the integrative treatment and Western medical treatment groups; the findings were compared with the results from the control group.
Routine blood analysis
Venous blood was obtained, both at admission and after 10 days of treatment, from patients in the integrative treatment and Western medical treatment groups. This blood was subjected to routine blood analysis (including red blood cell, white blood cell, lymphocyte, and platelet counts) with the XE-2100 automatic blood analyzer (Sysmex, Shanghai, China); the findings were compared with the results from the control group.
16S rDNA intestinal flora detection
Fecal specimens were obtained from patients in the integrative treatment and Western medical treatment groups, both at admission and after 10 days of treatment; they were also obtained from the control group. Specimens were kept in collection tubes and stored at −80°C. The processing of fecal samples, DNA isolation, and 16S rDNA intestinal flora sequencing detection were performed by Hegu Health (Hangzhou, China); in the sequencing protocol, the V4 region of 16S rDNA was amplified with the Illumina HiSeq, using primers for 515F and 806R. Sequencing data were analyzed using QIIME software, version 1.7.0.
Statistical analysis
SPSS Statistics, version 20.0 (IBM Corp., Armonk, NY, USA) was used for statistical analysis. The measurement data exhibited a normal distribution. One-way ANOVA was used for comparison among groups, followed by the least significant difference test. χ2 and t-tests were performed to compare counting and grading data, respectively. Differences with P < 0.05 were considered statistically significant.
Results
Clinical characteristics of study participants
Sixty patients with AECOPD were included in this study (n = 30 patients per group). Thirty healthy individuals were included in the control group. The study design was performed as shown in Figure 1. In the Western medical treatment group, two patients withdrew from the trial due to personal preference; therefore, 28 patients completed the study. Moreover, the patients in the Western medical treatment group ranged in age from 51 to 76 years (mean age, 62.03 ± 5.90 years); patients in the integrative treatment group ranged in age from 51 to 75 years (mean age, 64.27 ± 6.30 years); and patients in the control group ranged in age from 53 to 72 years (mean age, 64.11 ± 5.29 years). There were no significant differences in sex, age, or disease severity grading among the three groups (Tables 4 and 5). Moreover, no significant adverse reactions were reported in any patient during treatment.

Study flow diagram.
Clinical characteristics of study participants.
Note: Data are shown as n (%). Control and Integrative treatment groups, n = 30 participants each; Western medical treatment group, n = 28 participants.
Disease grades of study participants.

Note: Data are shown as n (%). Integrative treatment group, n = 30 participants; Western medical treatment group, n = 28 participants.
Integrative treatment exhibited superior therapeutic efficacy
Therapeutic efficacies were compared between treatment groups. The therapeutic efficacy of the integrative treatment was superior to the efficacy of the Western medical treatment (P < 0.05) (Table 6). The symptom severity scores improved over time for both treatment groups (P < 0.05) (Figure 2a). Moreover, improvement of respiratory difficulties was significantly greater in the integrative treatment group than in the Western medical treatment group (P < 0.05) (Figure 2b).
Therapeutic efficacies of integrative treatment and Western medical treatment.

Note: Data are shown as n (%). Integrative treatment group, n = 30 participants; Western medical treatment group, n = 28 participants.

Therapeutic efficacy of integrative treatment is superior to Western medical treatment for patients with AECOPD. (a) Statistical analysis of TCM-based clinical symptom severity scores for integrative treatment, Western medical treatment, and control groups, before and after treatment. (b) Statistical analysis of respiratory difficulty severity for integrative treatment, Western medical treatment, and control groups, before and after treatment. *P < 0.05, **P < 0.01, and ***P < 0.001. Abbreviations: AECOPD, acute exacerbation of chronic obstructive pulmonary disease; TCM, traditional Chinese medicine.
Integrative treatment improved blood-gas parameters and lung function
Before treatment, no significant differences were observed in PaO2 or PaCO2 between the integrative treatment and Western medical treatment groups. After treatment, the PaO2 level was significantly higher in the integrative treatment group than in the Western medical treatment group, while the PaCO2 level was significantly lower in the integrative treatment group than in the Western medical treatment group (P < 0.01) (Figure 3a and 3b). However, no significant within-group or between-groups differences were observed in pH values (Figure 3c).

Analysis of blood-gas parameters and lung function in patients with AECOPD. (a–c) Statistical analysis of PaO2 (a), PaCO2 (b), and pH (c) in the integrative treatment, Western medical treatment, and control groups, before and after treatment. (d–f) Statistical analysis of FEV1%pred (d), FEV1/FVC (%) (e), and FVC (f) in the integrative treatment (integrative; integrative +10D), Western medical treatment (Western; Western +10D), and control groups (Health), before and after treatment. *P < 0.05, **P < 0.01, and ***P < 0.001. Abbreviations: AECOPD, acute exacerbation of chronic obstructive pulmonary disease; PaO2, partial pressure of oxygen; PaCO2, partial pressure of carbon dioxide; FEV1%pred, percent predicted forced expiratory volume in 1 second; FEV1/FVC, ratio of forced expiratory volume in 1 second to forced vital capacity; FVC, forced vital capacity.
Lung function assessment revealed no significant difference in FEV1%pred between the integrative treatment and Western medical treatment groups after treatment (Figure 3d). However, FVC and FEV1/FVC were significantly higher in the integrative treatment group than in the Western medical treatment group (P < 0.05) (Figure 3f and 3e).
Integrative treatment significantly improved inflammatory responses in AECOPD
Pre-treatment assessment of inflammatory indexes for patients in the integrative treatment and Western medical treatment groups (Figure 4) showed no significant differences between the two treatment groups in terms of CRP, IL-6, IL-8, or TNF-α. After treatment, significantly greater improvements were observed in CRP (P < 0.05), IL-6 (P < 0.01), IL-8 (P < 0.01), TNF-α (P < 0.01), and procalcitonin (P < 0.05) in the integrative treatment group, compared with the Western medical treatment group (Figure 4a–e). Moreover, significant differences were observed in the percentages of neutrophils within groups (before and after treatment) and between groups after treatment (P < 0.05); greater improvement was observed in the integrative treatment group (Figure 4f). However, no significant within-group or between-groups were observed in routine blood test results (i.e., red blood cell, white blood cell, lymphocyte, and platelet counts) (Table 7).

Integrative treatment more significantly improves inflammatory responses in patients with AECOPD. (a–f) Statistical analysis of CRP (a), IL-6 (b), IL-8 (c), TNF-α (d), procalcitonin (e), and percentage of neutrophils (f) for the integrative treatment (integrative; integrative +10D), Western medical treatment (Western; Western +10D), and control groups (Health), before and after treatment. *P < 0.05, **P < 0.01, and ***P < 0.001. Abbreviations: AECOPD, acute exacerbation of chronic obstructive pulmonary disease; CRP, C-reactive protein; IL, interleukin; TNF, tumor necrosis factor.
Routine blood test data.

Control and Integrative treatment groups, n=30 participants each; Western medical treatment group, n=28 participants.
Integrative treatment altered 16S rDNA intestinal flora
Shannon curve (Figure 5a) and dilution curve (Figure 5b) analyses showed that assessments of intestinal flora in patients with AECOPD could comprehensively analyze the majority of microbial species in the test specimens. Alpha diversity box plot analyses (Figure 5c) showed that, compared with the control group, the numbers of operational taxonomic units (OTUs) were higher in both the integrative treatment and Western medical treatment groups; after treatment, significant differences were observed in numbers of OTUs between these two groups (P < 0.05). Compared with the Western medical treatment group, the numbers of OTUs in the integrative treatment group were more similar to those in the control group. These results suggested that both treatments could improve intestinal flora in patients with AECOPD, and that integrative treatment provided greater improvement. Non metric multidimensional scaling (NMDS) plot of beta diversity (Figure 5d) showed that, after treatment, differences in community composition were smaller between the integrative treatment and control groups, compared with differences between the Western medical treatment and control groups. This analysis also showed that, after treatment, community composition in the integrative treatment group was more similar to the composition in the control group. Venn diagram analysis (Figure 5e) showed that, before treatment, 583 OTUs were shared between the integrative treatment and control groups, whereas 603 OTUs were shared between the Western medical treatment and control groups. After treatment, 643 OTUs were shared between the integrative treatment and control groups, whereas 603 OTUs were shared between the Western medical treatment and control groups.

Detection of 16S rDNA intestinal flora in patients with AECOPD. (a) Shannon curve. (b) Dilution curve. (c) Alpha diversity box plot. (d) NMDS difference analysis plot of beta diversity. (e) Venn diagram for OTU analysis. Abbreviations: AECOPD, acute exacerbation of chronic obstructive pulmonary disease; NMDS, non-metric multidimensional scaling; OTU, operational taxonomic unit.
Integrative treatment altered gate-level constitution histogram findings
Gate-level constitution histogram analysis showed that Firmicutes and Bacteroidetes phyla had the highest abundances in all groups. Firmicutes abundance was significantly higher in healthy participants, whereas Bacteroidetes abundance was significantly higher in patients with AECOPD (Figure 6). After treatment, Verrucomicrobia abundance was significantly reduced in both treatment groups.
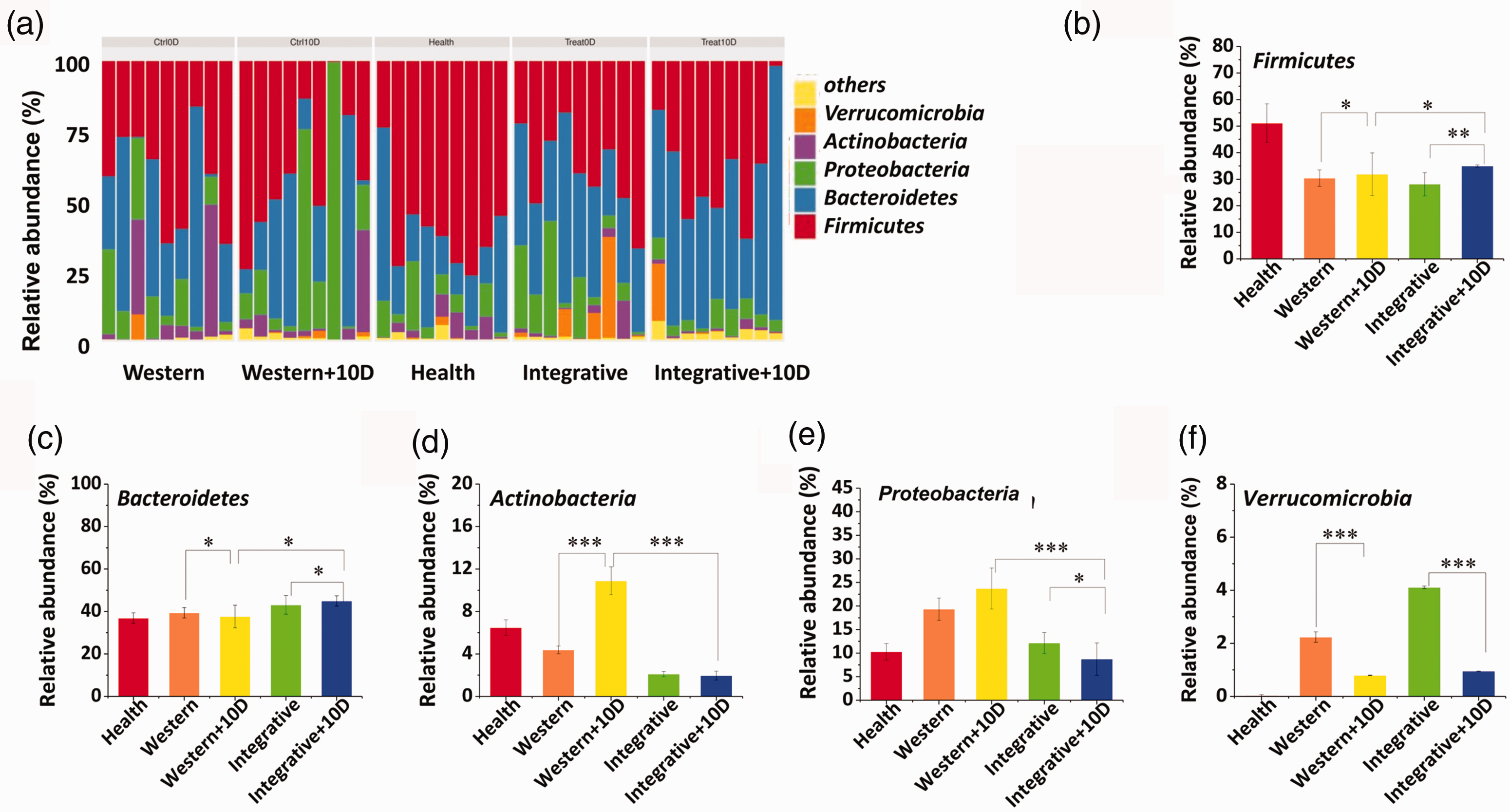
Gate-level constitution histogram analysis in patients with AECOPD (nine samples per group met the quality requirements for 16S rDNA intestinal flora analysis). (a) Gate-level constitution histograms. (b) Relative abundances of Firmicutes. (c) Relative abundances of Bacteroidetes. (d) Relative abundances of Actinobacteria. (e) Relative abundances of Proteobacteria. (f) Relative abundances of Verrucomicrobia. *P < 0.05, **P < 0.01, and ***P < 0.001. Abbreviation: AECOPD, acute exacerbation of chronic obstructive pulmonary disease.
Discussion
COPD is a common respiratory disease encountered in clinical practice. AECOPD worsens lung ventilation function and causes progressive damage, 18 resulting in heavy economic burden to patients and families. 19 Western medical treatments for AECOPD are mainly based on symptomatic routine treatment. However, patients are likely to experience relapse after relief of symptoms; drug resistance, side effects, and other complications have been reported during hospitalization. 20 Jianpi Huatan Tongfu granule is a clinical prescription for the treatment of AECOPD. It has been used in TCM for many years, especially in the context of combined clinical treatment using Chinese and Western medicines, where it effectively alleviates the side effects of Western medicines. However, to the best of our knowledge, there have been no relevant scientific studies in a controlled setting. In the present study, our results showed that the Western medicine combined with Jianpi Huatan Tongfu granule could effectively improve symptoms of dyspnea, avoid adverse reactions (e.g., cough, wheezing, and oppressed breathing), and improve clinical treatment efficacy.
This study investigated the efficacy of TCM using scores based on TCM and Western medicine, as well as laboratory tests and 16S rDNA assessment of intestinal flora detection. Our results showed that, before treatment, patients with AECOPD exhibited infection, hypoxia, and hypercapnia. Moreover, the PaO2 index of patients with AECOPD (i.e., “spleen deficiency and dampness syndrome”) was elevated after treatment, whereas the PaCO2 index was reduced; inflammation indexes were also reduced after treatment. Therefore, the degree of infection was closely related to the degrees of hypoxemia and hypercapnia, which reflected disease severity. Integrative treatment effectively relieved symptoms in patients with AECOPD. AECOPD is induced by bacterial or viral infections, which lead to long-term inflammatory responses (i.e., overexpression of inflammatory cytokines) and immune responses, further worsening disease progression during the acute exacerbation period. It is important to achieve timely and correct prediction of prognosis in patients with AECOPD.21–24 Our results showed that, before treatment, there were no significant differences in CRP, IL-6, IL-8, and TNF-α, between the two treatment groups. After treatment, significantly greater improvements were observed in CRP, IL-6, IL-8, and TNF-α in the integrative treatment group, compared with the Western medical treatment group.
According to TCM theory, the lung and large intestine are both exterior and interior. Beneficial intestinal flora may mediate immunity in these organs, thereby reducing the severity of respiratory pathological changes. 25 The interaction between intestinal flora and respiratory microecology may be consistent with the TCM theory that the lung and large intestine are interior-exteriorly related. 26 In the present study, patients with AECOPD had significant changes in intestinal flora, compared with the control group; in particular, alpha diversity was higher, and the numbers of OTUs and NMDS plot of beta diversity were altered in patients with AECOPD. The proportions of Firmicutes and Actinobacteria phyla were reduced, while the proportions of Proteobacteria and Verrucomicrobia phyla were elevated. These findings were consistent with the TCM theory. Moreover, the reduction of Verrucomicrobia abundance in both treatment groups was consistent with previous findings.27,28
In patients with AECOPD, the intestinal flora is altered; TCM could regulate the composition of intestinal flora, thereby protecting the intestinal mucosal barrier and restoring the intestinal microecological status. The Jianpi Huatan Tongfu granule effectively improved the intestinal flora in patients with AECOPD; it also caused the flora composition to become similar to that of the control group. Compared with the Western medical treatment group, alpha diversity was lower; the numbers of OTUs and NMDS plot of beta diversity were more comparable between the integrative treatment and control groups. These results suggested that both treatments could improve intestinal flora in patients with AECOPD, although the improvement was greater in the integrative treatment group. Therefore, we speculate that the Jianpi Huatan Tongfu granule acts on the lung and large intestine, and regulates the intestinal flora, thereby alleviating symptoms and achieving better therapeutic effects.
Our results showed that improvements in inflammation may be related to the regulation of intestinal flora; the underlying mechanism may be associated with the reduced inflammatory response induced by changes in proinflammatory cytokine secretion and neutrophil infiltration. 29 Changes in intestinal flora and microecology may inhibit inflammatory responses. 30 Our results showed that the Jianpi Huatan Tongfu granule significantly alleviated inflammatory responses in patients with AECOPD, which may have been related to TCM-induced changes in intestinal flora and microecology. The microbial composition and host immunity influence each other. 31 After the immune system is established in the host, development of immunity may lead to autoimmune reactions. Previous studies have shown that Firmicutes bacteria are closely associated with autoimmunity. 10 Our results revealed that, in patients with AECOPD, treatment with the Jianpi Huatan Tongfu granule could change the number of Firmicutes bacteria, which indicated that the regulation of intestinal flora by TCM may also be related to immunity. In addition, assessment of safety in the present study revealed no adverse reactions in either treatment group. These findings demonstrate the efficacy and safety of the Jianpi Huatan Tongfu granule for treatment of AECOPD.
In conclusion, our study showed that the Jianpi Huatan Tongfu granule could significantly alleviate inflammatory responses and improve the clinical therapeutic efficacy in treatment of AECOPD. The therapeutic efficacy was positively correlated with changes in the intestinal flora. After integrative treatment, the intestinal flora were comparable to those of the control group. These findings may provide evidence to support the use of the Jianpi Huatan Tongfu granule in the treatment of AECOPD, which may aid in improving disease prognosis.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This study was supported by the National Natural Science Foundation of China (Grant Nos. 81660730 and 81473457), the Open Fund of Key Laboratory of Molecular Medicine and Traditional Chinese Medicine Prevention and Treatment for Major Diseases for Colleges and Universities in Gansu Province (Grant Nos. FZYX14-2 and FZYX14-7), and the Major Science and Technology Project of Gansu Province (Grant No. 18YF1FA044).