
Abstract
Osteoid osteoma is a small benign bone tumor that is primarily localized in long bone; lumbar osteoid osteoma combined with scoliosis has rarely been reported. Here, we describe a 9-year-old boy who complained of back pain and scoliosis. He underwent nidus resection and did not experience complications or osteoid osteoma recurrence. His pain and scoliosis were relieved after the operation. The findings in this case indicate that resection of osteoid osteoma is an effective and safe method of treatment. The lumbar spine is the most common location of osteoid osteoma, which causes painful scoliosis. Nidus resection can provide relief of back pain and scoliosis.
Introduction
Osteoid osteoma is a small benign bone tumor that arises from osteoblasts, which was first described by Jaffe in 1935 1 as a smaller version of an osteoblastoma. A tumor size of <1.5 cm was regarded as an osteoid osteoma, while a tumor of >1.5 cm was regarded as an osteoblastoma. Approximately 10% of osteoid osteomas occur in the spine; the majority of spinal osteoid osteomas occur in lumbar vertebrae, commonly in the posterior elements. Osteoid osteoma commonly occurs in the second decade of life, and is more common in boys than in girls (approximate ratio of 3:1).2,3 The typical chief complaints are pain that worsens at night and is relieved by administration of aspirin. The pain is caused by vascular pressure and the production of prostaglandins in the nidus of the osteoid osteoma. 4 These aspects underlie the responses of osteoid osteomas to treatment with non-steroid anti-inflammatory drugs. Scoliosis resulting from spinal osteoid osteoma has been reported to cause painful scoliosis in 70% of adolescent patients; this painful scoliosis may be caused by paravertebral muscle spasm. 5
Computed tomography (CT) is regarded as the best diagnostic tool for nidus identification and localization; magnetic resonance imaging (MRI) is less accurate than CT. 6 Recently, interstitial laser photocoagulation and percutaneous radiofrequency coagulation have become increasingly popular for the treatment of non-spinal osteoid osteoma. 7 Wang et al. showed that CT-guided percutaneous radiofrequency ablation was safe and effective for the treatment of spinal osteoid osteoma; however, this method is not indicated for lesions that are in close proximity to neurological structures. 8 Surgery is the most common method for treatment of spinal osteoid osteoma; the prognosis for pain relief is good when en bloc resection of the tumor is performed. Here, we describe a patient who had an L5 osteoid osteoma, which was successfully treated by surgical resection.
Case report
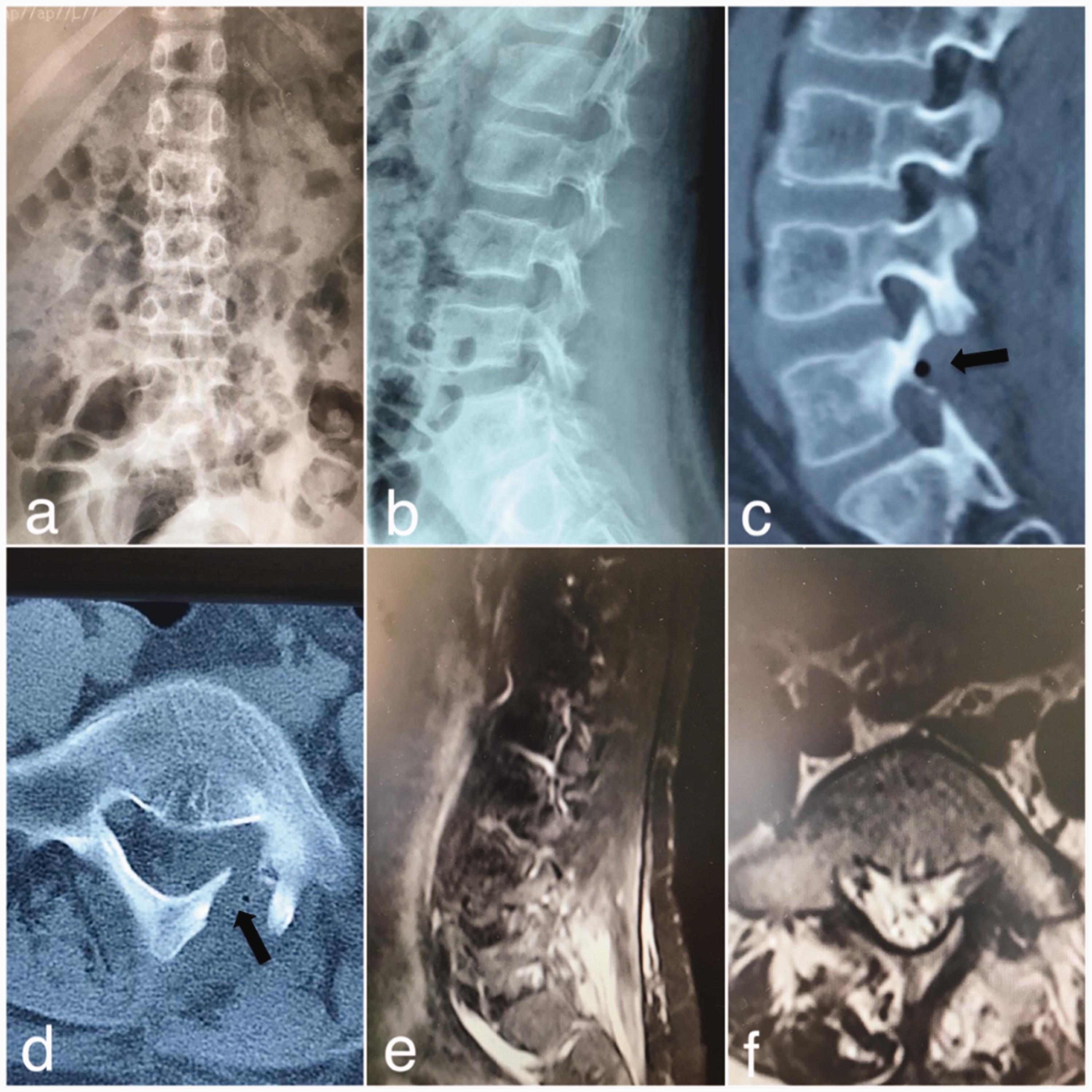
A 9-year-old boy presented with the complaint of lower back pain that had been present for 3 months and became aggravated at night. Physical examination revealed lumbar percussion pain and tenderness, combined with lumbar scoliosis. Neurologic examinations and laboratory analysis revealed no abnormalities. CT findings revealed a nidus in the left lamina of the L5 vertebrae. The nidus size was 4 mm. MRI showed inflammatory changes in the entire left pedicle, as well as the left lamina and vertebral body (Figure 1). However, the tumor did not compress the nerve root. Therefore, the patient was diagnosed with osteoid osteoma.

(a, b) Anteroposterior and lateral views of the lumbar spine revealed scoliosis, with absence of thoracic vertebrae rotation and minimal lumbar vertebrae rotation to the concave side. (c, d) Computed tomography scans revealed the nidus of the osteoid osteoma (black arrows). (e, f) Magnetic resonance imaging showed edema and inflammatory changes of the lamina and paravertebral soft tissue (red arrows).
We performed surgery using a traditional posterior approach, with the patient under general anesthesia. When the L5 level was identified under fluoroscopic control, partial laminectomy was performed as necessary. Total nidus resection was completed by using an osteotome. Histology and pathology findings confirmed the diagnosis of osteoid osteoma. The patient reported absence of pain and scoliosis after surgery. Postoperative anteroposterior imaging revealed that the scoliosis had disappeared. Postoperative CT revealed that the nidus had been completely resected, while postoperative MRI demonstrated resolution of edema in the lamina and paravertebral soft tissue (Figure 2). Routine follow-up was performed at 1 week, 6 weeks, and 6 months postoperatively. During 18 months of follow-up, the patient remained asymptomatic without recurrence of osteoid osteoma. The patient and his family consented to the publication of this case report.
(a, b) Anteroposterior and lateral views of the lumbar spine showed disappearance of lumbar scoliosis. (c, d) Computed tomography scan showed en bloc resection of the nidus (black arrows). (e, f) Magnetic resonance imaging showed relief of edema and inflammatory changes in the lamina and paravertebral soft tissue.
Discussion
Patients with osteoid osteomas generally complain of pain that increases in severity during the night. This pain can be relieved by administration of non-steroid anti-inflammatory drugs. Some affected patients may present with painful scoliosis. Uehara et al. described a patient with osteoid osteoma who had presented with thoracic scoliosis; the patient complained of scoliosis without back pain or other problems. 9 In the patient described by Uehara et al., the pain-related scoliosis resolved upon relief of the pain, similar to our patient; however, true scoliosis does not resolve. Moreover, patients with true scoliosis may exhibit deformities of the vertebral body, such as hemivertebrae or butterfly vertebrae, which are visible in X-ray images or CT scans. 10 In patients with osteoid osteoma, pain generally arises from spasms of the paravertebral muscle, which cause pain-related scoliosis. Consistent with the findings in prior case reports, our patient complained of night pain and scoliosis.
Osteoid osteoma tumors can be detected by CT scans and bone scans; CT is more commonly used. Classically, CT scans of patients with osteoid osteoma have revealed a nidus with central mineralization and varying degrees of perennial sclerosis. 11 However, CT findings in the spine depend on the position of the nidus; if its location is subchondral, sclerosis may be absent. In addition, if incisions are made at an inappropriate level or are excessively wide, the nidus of the tumor may be missed. Bone scanning represents a more sensitive method for localization of the tumor. In particular, the technetium bone scan method provides accurate localization of the lesion. 12 For detection of changes in soft tissue and bone marrow around the nidus, MRI is a more sensitive modality than CT. However, MRI findings can be misleading in patients with osteoid osteoma. 13 Therefore, it is necessary to rule out low-grade infection, as well as tuberculosis and Brodie abscesses, when using MRI findings for diagnosis of patients with osteoid osteoma. CT should be used when evaluating benign tumors with known inflammatory responses on MRI. The majority of spinal osteoid osteomas are located in lumbar vertebrae and the posterior elements; indeed, in our patient, the nidus was found in the left lamina of the L5 vertebrae. Osteoblastoma histology resembles that of osteoid osteoma; these tumors can be differentiated by size. The differential diagnosis should also include osteochondroma, aneurysmal bone cyst, and giant cell tumor. Furthermore, pain-related scoliosis can be caused by conditions such as lumbar disc herniation, muscular spasm, and discogenic pain; these should also be ruled out. 14
Treatment varies based on the condition of the affected patient. Some patients can be treated successfully by a conservative approach. However, most patients cannot tolerate long-term conservative treatment. If medication therapy fails or if the lesion increases in size, patients are selected for surgery with the aim of en bloc resection of the tumor. After resection of an osteoid osteoma, pain and scoliosis are relieved. Radiofrequency ablation is an attractive method because it involves minimal bone destruction and is minimally invasive, with adequate safety and efficacy.15,16 Radiofrequency ablation can be combined with guided bone biopsy. However, radiofrequency ablation is more widely used for non-spinal osteoid osteomas 3 owing to the risk of damage to neural structures. We considered radiofrequency ablation to be inappropriate for our patient because his osteoid osteoma was adjacent (1.45 mm) to the dura. Moreover, minimally invasive surgeries, such as those involving video endoscopy, microscopy, and imaging-guided or navigation-guided techniques also achieve satisfactory outcomes. 17 However, these methods have steep learning curves, as well as requirements for additional education and equipment.18,19
In this report, we have described a patient with a rare L5 osteoid osteoma, who complained of lumbar pain and scoliosis. The patient underwent nidus resection without any complications; his pain and scoliosis were relieved after the surgery. Our findings demonstrate that, if the osteoid osteoma nidus exhibits close proximity to the neural canal, resection of the osteoid osteoma is an effective and safe treatment method. The lumbar spine is the most common location of osteoid osteoma, which causes painful scoliosis. Nidus resection can provide relief of back pain and scoliosis in affected patients.