
Abstract
Objective
Recent studies demonstrated that circulating tumor cells (CTCs) contribute to the metastasis of prostate cancer. Survivin knockout could inhibit epithelial-mesenchymal transition (EMT) and suppress several metastatic tumors. In this study, we examined the potential involvement of survivin in EMT in CTCs.
Methods
CTCs were isolated from the peripheral blood of 100 patients with prostate cancer as EpCAM+/CD45− cells via FACS sorting and identified by immunofluorescence staining of prostate-specific antigen (PSA). CTCs and DU145 cells were transfected with survivin siRNA. Then, the levels of survivin, E-cadherin, and vimentin in CTCs and DU145 cells were detected via immunofluorescence staining, and the invasiveness of CTCs and DU145 cells was examined using a Transwell chamber.
Results
The results revealed the abundant expression of PSA in the cytoplasm of CTCs. Transfection of survivin siRNA significantly decreased the levels of survivin and vimentin in CTCs and DU145, whereas that of E-cadherin was significantly increased, suggesting survivin plays an important role in EMT of CTCs. In addition, survivin siRNA significantly inhibited the invasiveness of CTCs and DU145 cells.
Conclusions
Survivin plays an important role in EMT of CTCs in prostate cancer, which might mediate the metastasis and invasion of prostate cancer.
Keywords
Introduction
Prostate cancer is one of the most common malignant tumors in men, and circulating tumor cells (CTCs) play key roles in its recurrence and metastasis.1–3 In recent years, the detection of CTCs has been used to monitor the recurrence and metastasis of prostate cancer.4–6 CTCs refers to tumor cells circulating in peripheral blood because of the spontaneous shedding of the primary tumor or shedding occurring during treatment.
It is currently clear that CTCs represent the main cause of tumor metastasis. 7 Epithelial tumor cells are transformed into cells with a mesenchymal phenotype via a biological process termed epithelial-mesenchymal transition (EMT), which eliminates cell polarity and the connection with the basement membrane and grants cells migratory, invasive, and anti-apoptosis activity and the ability to degrade extracellular matrix.8,9 Prior studies indicated that EMT is associated with wound healing, fibrosis, and tumor progression.8,10 Although only a handful of CTCs entering the circulatory system survive and further develop into metastatic foci, this is a critical process for achieving tumor metastasis.11,12
Metastatic prostate cancer is the final stage of prostate cancer progression. The optimal clinical treatment of metastatic prostate cancer remains controversial. 13 Radiotherapy and chemotherapy can prolong the survival time of patients with metastatic prostate cancer, but the side effects of chemotherapy significantly reduce patients’ quality of life. Therefore, an in-depth understanding of the mechanism of prostate cancer metastasis and early screening of prostate cancer are the most important task for diagnosis and treatment.
Although CTCs were discovered more than 100 years ago, the specific role and mechanisms of these cells in the process of tumor metastasis remain unclear.14,15 CTCs may represent a specific type of cancer stem cell that shares some of the characteristics of stem cells, making them more invasive. 16 Aceto et al. researched the role of CTCs in breast and prostate cancer, finding that CTCs can increase the metastatic potential of tumor cells and play a key role in tumor metastasis. 17
Prior research indicated that the interaction between CTCs and platelets accelerates the rate of CTC metastasis. Labelle et al. 18 demonstrated that the interaction between platelet-derived TGF-β and CTCs activates CTCs TGF-β/Smad and NF-κB signaling pathways, making tumor cells more aggressive via EMT. Survivin knockout suppresses ovarian metastatic tumors. 19 Survivin is also involved in the radioresistance and castration resistance of prostate cancer.20,21 It was demonstrated that survivin levels of CTCs are associated with prostate cancer metastasis. Therefore, we examined whether survivin is involved in EMT in CTCs.
Materials and methods
Patients and samples
In total, 100 patients with prostate cancer were enrolled after providing written informed consent. The study was approved by the ethics committee of Shandong Cancer Hospital (SHEC89E). All biopsy specimens from patients with prostate cancer were examined independently by two experienced pathologists. Finally, peripheral blood was collected from the patients, after which circulating tumor cells were collected as previously described.1,22 In brief, CTCs were isolated as EpCAM+/CD45− cells via FACS sorting on a MoFlo XDP high-speed cell sorter system (Beckman Coulter, Brea, CA, USA). The CTCs were identified via immunostaining of prostate-specific antigen (PSA). DU145 cells were obtained from American Type Culture Collection (Manassas, VA, USA).
Immunofluorescence staining
Cells isolated or transfected after 24 hours were quickly washed once with PBS, fixed with 2% PFA, and blocked with 2% goat serum. Cells were then stained with anti-PSA, anti-Twist, anti-E-cadherin, anti-vimentin, or anti-survivin antibody (1:100, Santa Cruz Biotechnology, Santa Cruz, CA, USA) overnight and then visualized via incubation with AF488 or AF594 secondary antibody for 1 hour at room temperature. Cells were imaged using an LSM 510 confocal microscope (Zeiss, Oberkochen, Germany) as described previously. 23
Survivin siRNA transfection
Survivin siRNA was synthesized as previously described. 24 Survivin siRNA was transfected into CTCs or DU145 cells using the Neon Transfection System (Invitrogen, Thermo Fisher Scientific, Carlsbad, CA, USA) according to the manufacturer’s manual. The non-transfected cells were eliminated using G418. Cell culture was maintained for 48 hours.
Invasion assay
CTC invasion was performed using a Transwell chamber (Millipore, Billerica, MA, USA). After mixing with Matrigel, cells were seeded into 24-well plates and cultured at 37°C in Dulbecco’s modified Eagle’s medium (Invitrogen) containing 2% serum, and 600 μl of medium containing 10% FBS was added into the lower chamber. After 48 hours, cells were fixed with methanol for 30 minutes and stained with crystal violet for 20 minutes. Non-invaded cells were removed using cotton swabs. Cell images were obtained using a microscope (Olympus, Tokyo, Japan).
Statistical analysis
All data were expressed as the mean ± SD. Student’s t-test or one-way analysis of variance with the least significant difference test was performed using SPSS 10.0 (SPSS Inc., Chicago, IL, USA). The statistical significance level was defined as p < 0.05.
Results
CTCs express PSA
To identify the isolated CTCs, we detected PSA levels via immunofluorescence staining (Figure 1). The results revealed that PSA was abundantly expressed in the cytoplasm of CTCs, confirming that the isolated CTCs were prostate cancer cells.
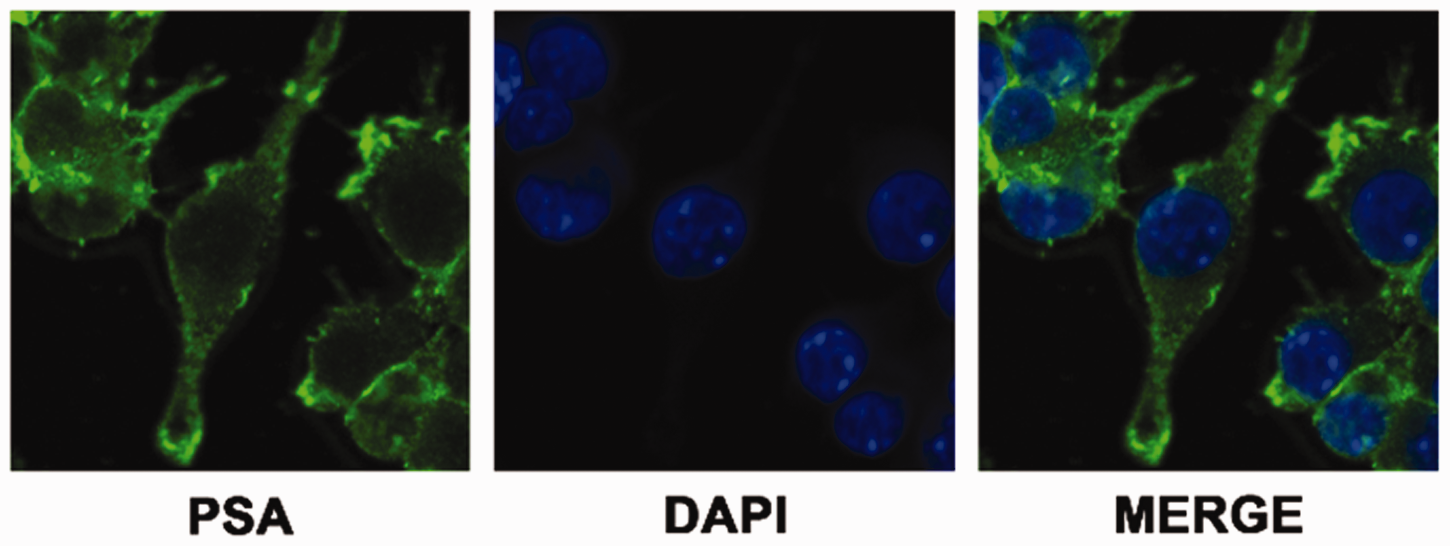
Immunostaining of prostate-specific antigen (PSA) in circulating tumor cells (CTCs). CTCs were isolated as EpCAM+/CD45− cells via FACS sorting on a MoFlo XDP high-speed cell sorter system and then identified via immunostaining of PSA.
Silencing of survivin in CTCs
To further detect the EMT capacity of CTCs and the related role of survivin, siRNA against survivin (siSurvivin) was transfected into CTCs and DU145 cells (Figure 2). The efficiency of siRNA transfection was approximately 60%. The efficiency was confirmed via qRT-PCR (data not shown). An immunofluorescence assay illustrated that survivin expression was significantly inhibited by siSurvivin (P < 0.05). Then, the cells were used for the subsequent experiments.

Silencing of survivin in circulating tumor cells (CTCs) and DU145 cells. After transfection with survivin siRNA, survivin expression in CTCs and DU145 cells was examined using immunofluorescence staining. DU145 cells were used as the positive control.
siSurvivin increased the expression of E-cadherin
To identify the role of survivin in EMT of CTCs, the expression of e-cadherin in CTCs was detected (Figure 3). E-cadherin expression in DU145 cells served as the positive control. After transfection of siSurvivin, E-cadherin expression was significantly increased in CTCs. E-cadherin expression was also increased in DU145 cells transfected with siSurvivin. Thus, silencing of survivin inhibited the epithelial cell phenotype.
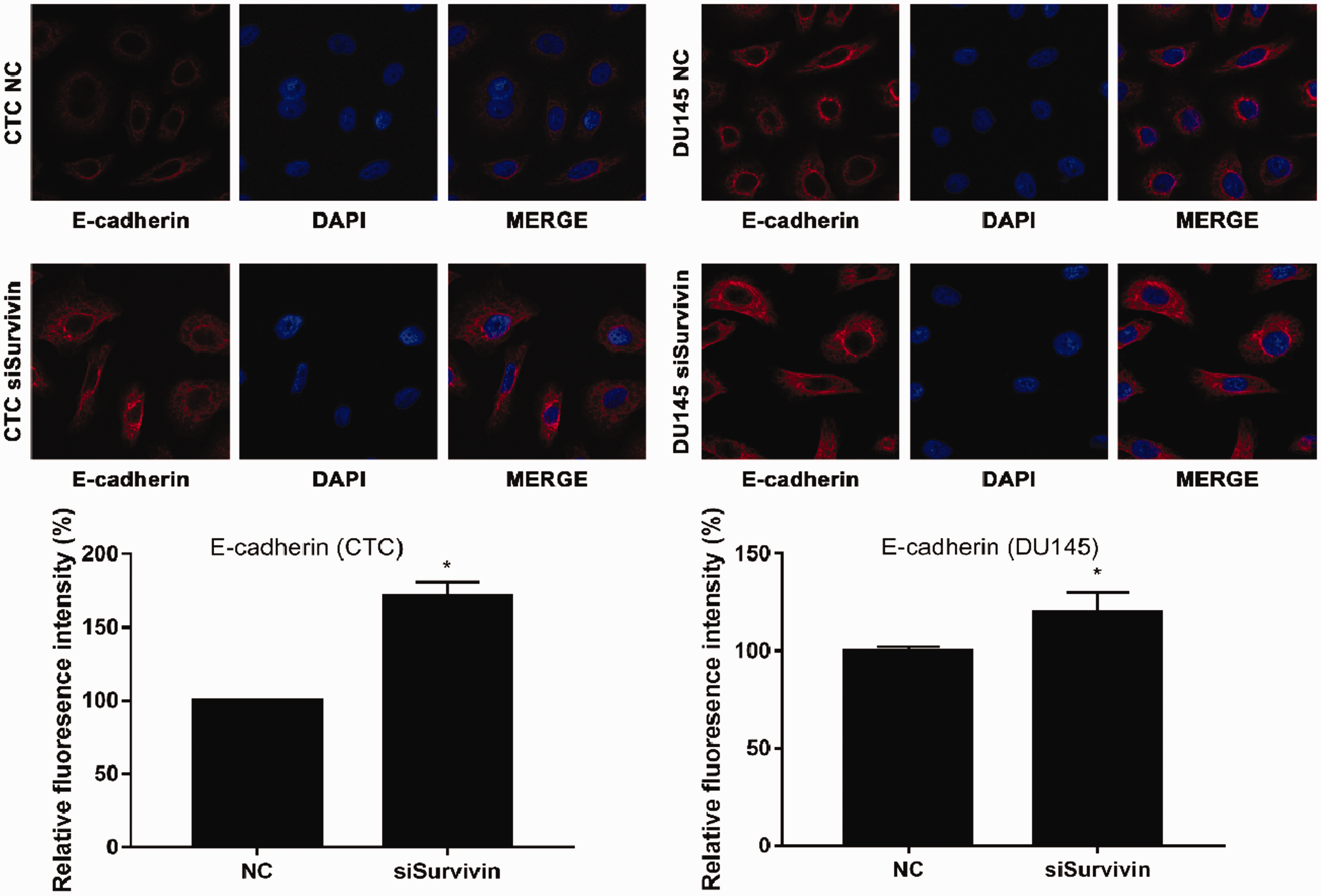
Expression of E-cadherin in circulating tumor cells (CTCs) and DU145 cells. After transfection with survivin siRNA, the expression of E-cadherin in CTCs and DU145 cells was examined using immunofluorescence staining. DU145 cells were used as the positive control.
siSurvivin inhibited the expression of vimentin
To identify the role of survivin in EMT of CTCs, the expression of the mesenchymal marker vimentin in CTCs was also detected (Figure 4). Vimentin expression in DU145 cells was set as a positive control. After silencing of survivin, vimentin expression was significantly decreased in CTCs. Similarly, vimentin expression was also increased in DU145 cells transfected with siSurvivin. Thus, silencing of survivin increased the mesenchymal cell phenotype.
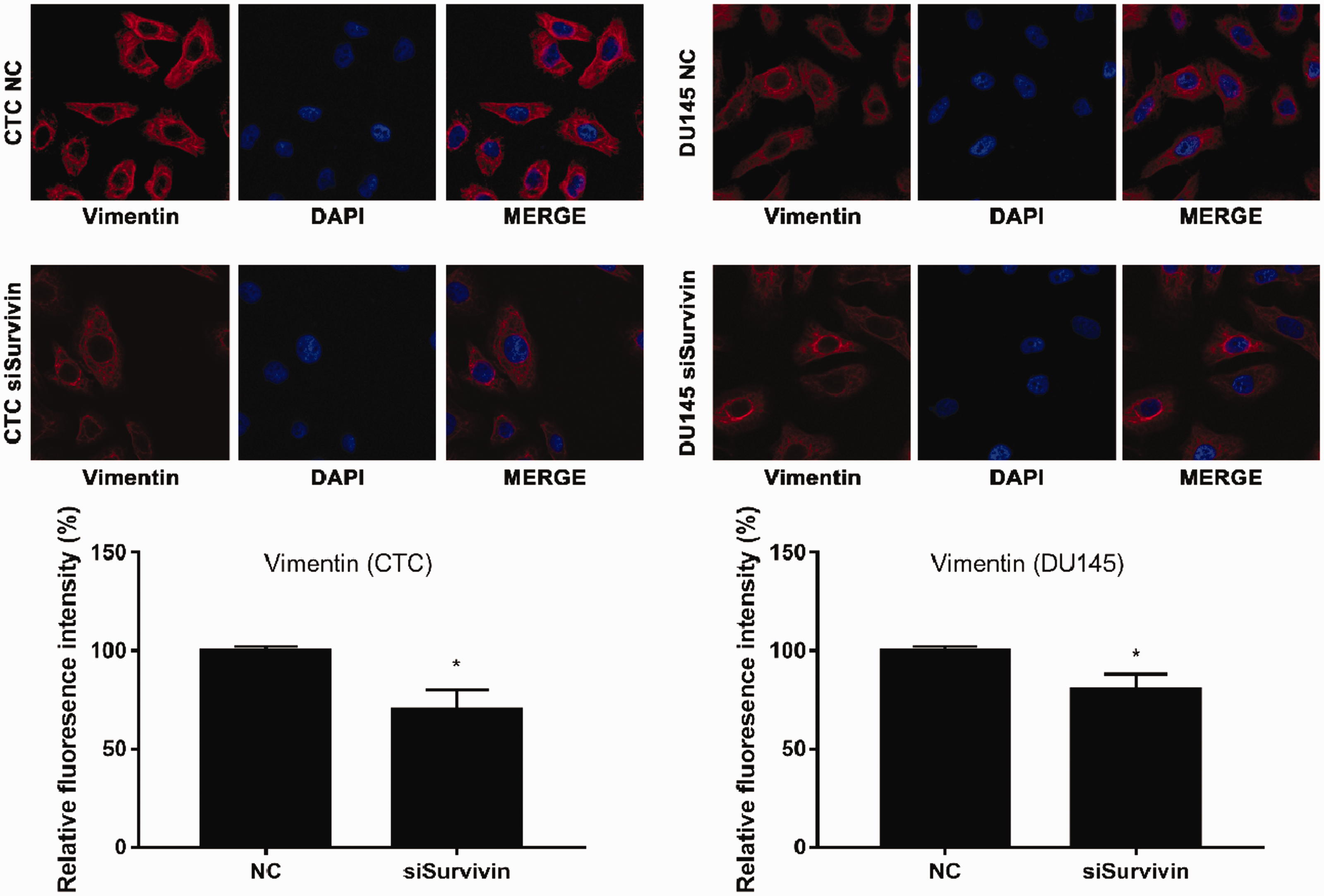
Expression of vimentin in circulating tumor cells (CTCs) and DU145 cells. After transfection with survivin siRNA, the expression of vimentin in CTCs and DU145 cells was examined using immunofluorescence staining. DU145 cells were used as the positive control.
siSurvivin inhibited cell invasion
The role of survivin in the invasiveness of CTCs and DU145 cells was also examined (Figure 5). The invasiveness of both sell types was significantly reduced by silencing of survivin. Taken together, survivin is involved in EMT of CTCs.

Invasiveness of circulating tumor cells (CTCs) and DU145 cells. After transfection with survivin siRNA, the invasiveness in CTCs and DU145 cells was examined using Transwell assays. DU145 cells were used as the positive control. (a) Invasion. (b) Cell count. *p < 0.01 vs. NC.
Discussion
Prostate cancer is one of the most common malignant tumors in elderly men, and more than 95% of the patients are diagnosed at an age of 45 to 89 years (mean age, 72 years). 25 In recent years, the important roles of CTCs in the diagnosis and prognosis of prostate cancer as well as evaluation of the curative effect of treatment. Goldkorn et al.26,27 found that in patients with metastatic castration-resistant prostate cancer and a CTC count <5/7.5 mL, the overall survival was 26 months, compared with 13 months in patients with a CTC count ≥5/7.5 mL. These data indicate that higher CTC counts are associated with worse overall survival. Therefore, the CTC count can be used as a marker for clinical prognosis and treatment. In another study, the telomerase activity of CTCs could independently predict the overall survival of patients with CTC counts ≥5/mL (hazard ratio = 1.14, P = 0.001). Although this conclusion needs to be further confirmed, the data emphasize that the molecular characteristics of CTCs have important clinical value in personalized cancer diagnosis and treatment. In addition, Aceto et al. 17 found that the average survival time was 115.8 days in patients with CTC, which was significantly lower than the average survival time of 930.1 days in patients with lower CTC counts. In this work, we collected CTCs from 100 patients, but the number of cells was not sufficient to permit western blotting to detect survivin, E-cadherin, and vimentin expression. We will collect more CTCs to measure the expression of these proteins in the future. In addition, the Gleason score and clinical stage of the patients were not analyzed. Additionally, some patients had castration-resistant prostate cancer.
A multicenter prospective study conducted by de Bono et al. 28 revealed that the CTC count at different time points after treatment was the best independent predictor of overall survival, and the CTC count was more accurate than the PSA concentration for predicting prostate cancer survival. They also demonstrated that that the CTC count at intermediate monitoring points can be used to evaluate the efficacy of treatment. Scher et al. 29 found that the CTC count was one of the most predictive markers for survival in patients with prostate cancer, and the predictive value of CTC counts was higher than that of PSA concentrations in a study of 276 patients. Thus, CTCs are expected to represent another indicator of the efficacy and prognosis of prostate cancer that can better guide the development of clinical treatment programs.
EMT is a complex pathological process that increases the ability of epithelial cells to metastasize and migrate accompanied by the disappearance of epithelial-like features and the acquisition of interstitial characteristics. 30 EMT plays an important role in the process of CTC shedding from the primary lesion into the blood vessels and formation of prostate cancer micrometastases. In view of the role of the EMT marker vimentin in promoting the metastasis and invasion of prostate cancer, it is of great clinical significance to detect vimentin levels in CTCs and explore its utility for predicting the diagnosis and metastasis of prostate cancer. At the same time, it is important to detect the expression of EMT markers in prostate CTCs and investigate whether the inhibition of survivin expression is associated with changes in the cell phenotype and invasive potential of prostate CTCs.
We examined the involvement of survivin in EMT of CTCs. CTCs were isolated from patients with prostate cancer and identified via immunofluorescence staining of PSA. CTCs and DU145 cells were transfected with survivin siRNA. Then, the levels of survivin, E-cadherin, and vimentin were detected via immunofluorescent staining, and the invasiveness of cells was detected. The results illustrated the abundant expression of PSA in the cytoplasm of CTCs. Transfection of survivin siRNA increased the expression of E-cadherin and decreased that of vimentin in CTCs, in addition to increasing cell invasion. Taken together, survivin plays an important role in EMT of CTCs in prostate cancer. To further clarify the mechanism, the factors involved in survivin-mediated cell metastasis and invasion, such as VEGF and GRP78, should be analyzed in the future.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were conducted after obtaining approval from the Shandong Cancer Hospital Ethics Committee and performed in accordance with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Informed consent
Informed consent was obtained from all individual participants included in the study.