
Abstract
Multiple sclerosis (MS) is an autoimmune disease that affects the central nervous system, causing inflammation, demyelination, and neurodegeneration. Infection can play a role in its etiology. Herein, a review is presented of studies that have reported an association between infection and MS risk in countries of the Arabian Gulf region. Searches of the PubMed, Google Scholar, and Science Direct databases were carried out using various search terms, and relevant studies published through January 2019 on the epidemiology of MS in Gulf Cooperation Council countries identified. MS has been found to be associated with measles in Saudi Arabia and Epstein–Barr virus in Kuwait whereas no association has been identified between risk of MS and varicella-zoster virus, mumps, or human herpesvirus-6. However, few epidemiological studies on this topic have been conducted in countries of the Gulf region. Longitudinal and serological studies to establish robust evidence between infection and risk of MS are highly recommended, and a regional MS registry is needed.
Keywords
Introduction
Multiple sclerosis (MS) is an autoimmune disease that affects the central nervous system. In this pathological condition, the myelin sheath of the nerve fibers is attacked by the immune system. 1 MS is similar to other autoimmune diseases in that it disproportionately affects women, at nearly twice the frequency as men, probably owing to immunologic variations such as the stronger Th1-mediated immune responses in female mammals. 2 Moreover, the X chromosome is likely to be a contributing factor in the elevated MS susceptibility among women.3,4 MS susceptibility is broadly acknowledged to be mediated by a complex interaction between unidentified ecological and/or behavioral aspects that exist in certain regions of the world and within genetically suspect hosts.5,6 Although the complete etiology of MS remains unknown, autoimmunity has been implicated in this process. 7 MS arises from complex interactions between individual genetic susceptibility and environmental factors. Nearly 50% of the MS risk is attributed to alleles and genes mapped in the HLA-II locus. 8 Variations in HLA-II genes and allele frequencies and types have been observed among different nations and ethnic groups worldwide. 9 The genetic profile of MS is heterogeneous in the Gulf region, comprising Gulf Cooperation Council countries, where the MS profile is not unique but is unlike that observed in other regions. In Saudi Arabia, HLA-DRB1*15:01 is the most frequently observed risk allele for MS among Saudi patients. 10 This is in line with MS risk alleles observed in patients from Iran.11–14 Likewise, it is the same allele reported among patients with MS from Sweden, Australia, the Netherlands, Spain, and Italy.15–19 By contrast, in Bahrain, another Gulf region country, the HLA-DRB1*15:01 allele is not a risk allele for MS; instead, HLA-DR3, HLA-DR4 and HLA-DR16 have been reported as MS risk alleles in Bahraini patients. 20 In Kuwait, some patients with MS express HLA-DR4, similar to some Bahraini patients. In addition, Kuwaiti patients also express HLA-DQ6, HLA-DQ7, and HLA-DQ8. 21 From another viewpoint, HLA-DR6 and HLA-DQ1 are protective alleles among Kuwaiti patients 21 whereas HLA-A10 is protective among Bahraini individuals. 20 In a Saudi study, HLA-DQB1*02:02, HLA-DQB1*05:03, and HLA-DQB1*06:14 were found to be protective alleles against MS. 10 This is in contrast to protective alleles against MS like HLA-DRB1*11, which have been documented by the World Health Organization and in reports from Spain and India.22–24 Another protective allele is HLA-DRB1*1001, which has been reported in Iran. 13 Various studies have shown that infectious and noninfectious environmental factors in children and young adults are correlated with a strong risk of MS. 25 Several theories on the cause of MS have emerged, supported by varying degrees of evidence; these include infectious diseases,26,27 an autoimmune state,28,29 and vascular diseases.30,31 Presently, the most widely accepted hypothesis is that MS is an immune-mediated illness with variable stages of immune activity within individuals and sometimes among individuals within a population. Many common mechanisms of autoimmunity are suspected as playing a role in this process, such as major and minor failures of normal self-tolerance, induced by various causes such as bacterial or viral infectivity or target tissue abnormality. 32 High antibody titers against viruses have been reported in MS patients. Notably, most studies on the infectious causes of MS, which are generally based on clinical, experimental, and pathological observations in animals, have been conducted in Western countries.33,34 The six countries of the Gulf Cooperation Council (GCC) include the Arabian Gulf nations, specifically, Saudi Arabia, United Arab Emirates, Bahrain, Oman, Kuwait, and Qatar. Together, the GCC countries have a population of 50 million (Figure 1). 35 These GCC nations have many commonalities and share aspects such as borders, experiences of climate change, cultural values, lifestyles, and socioeconomic development. Over the past 20 years, oil and gas revenues have led to drastic social and cultural changes as well as an epidemiologic transformation, 36 which may be leading to increases in environmental factors that result in conditions such as vitamin D deficiency,37,38 infections,39,40 obesity,41,42 and smoking.43,44 In addition, increasing younger populations and the availability of free medical services for citizens may facilitate early diagnosis and partially explain an increase in the MS incidence. The aim of the current study was to review published studies that have reported an association between infection and the risk of MS in GCC countries.

Gulf Cooperation Council (GCC) countries.
Methods
To identify relevant studies on the epidemiology of MS in the GCC countries, a number of search terms were used to search the PubMed, Google Scholar, and Science Direct databases. All studies included in this review were published during or before January 2019. The three databases were searched using keywords or phrases that included MS (multiple sclerosis) and the name of each GCC nation, as follows: [“multiple sclerosis”] AND [“Saudi Arabia” OR “Kuwait” OR “United Arab Emirates” OR “Oman” OR “Qatar” OR “Bahrain”]. Thereafter, the identified articles on MS were reviewed using their abstracts, titles, tables, and references (Figure 2). The original search was broad, to help achieve the main objective of the current study. Ethical approval and informed consent were not required owing to the nature of the study.
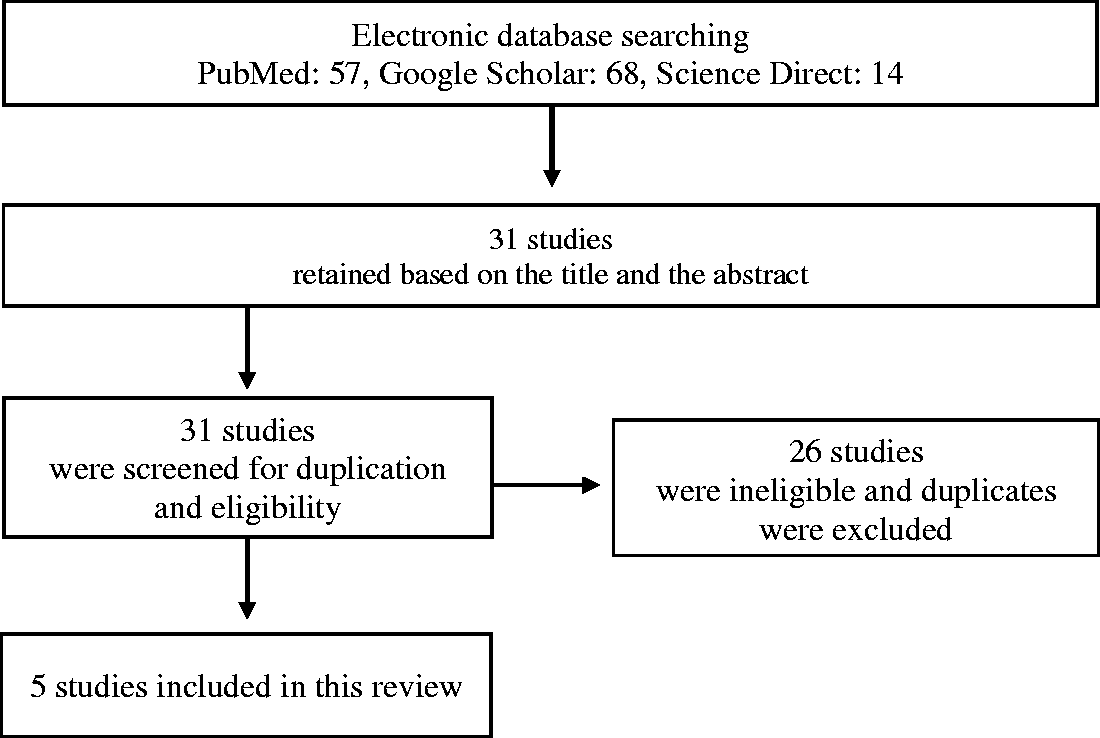
Flow chart of strategy used for article selection.
Results
Five studies were conducted on MS in GCC countries and fulfilled the criteria for inclusion in this review. Among these five articles reporting an association between MS and infection, only two GCC countries were represented, Saudi Arabia and Kuwait.45–49 The relevant details of these studies are listed in Table 1.
Studies in Gulf Cooperation Council countries of multiple sclerosis and reporting infection.
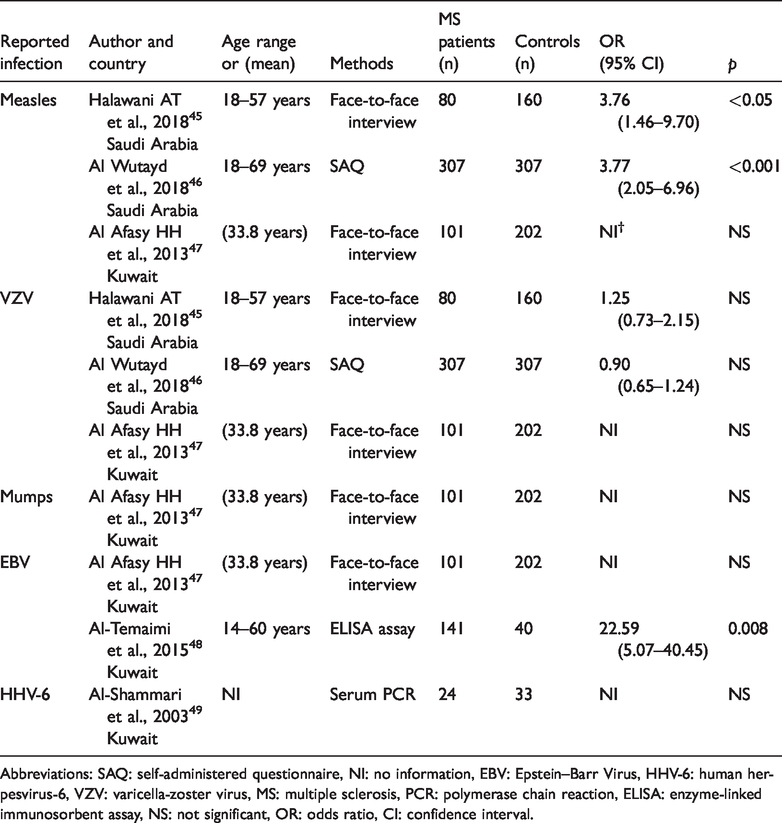
Abbreviations: SAQ: self-administered questionnaire, NI: no information, EBV: Epstein–Barr Virus, HHV-6: human herpesvirus-6, VZV: varicella-zoster virus, MS: multiple sclerosis, PCR: polymerase chain reaction, ELISA: enzyme-linked immunosorbent assay, NS: not significant, OR: odds ratio, CI: confidence interval.
Measles
Measles is a highly contagious virus belonging to the paramyxovirus family. The virus is transmitted through airborne droplets or VIA direct contact and infects the respiratory tract, with subsequent spread to the rest of the body. 50 Three case-control studies were conducted in GCC countries to assess the association between measles and MS. Two of these studies were conducted in Saudi Arabia, and both reported that measles infection increased the MS risk by approximately 4-fold. The first study reported an odds ratio (OR) of 3.76 and confidence interval (CI) of 1.46 to 9.70; 45 the second study reported an OR of 3.77 and 95% CI of 2.05 to 6.96. 46 In contrast, a study on measles and MS conducted in Kuwait found that measles posed a statistically insignificant risk for MS. 47
Varicella-zoster virus (VZV)
Chickenpox is a contagious infection, usually occurring in children, which is caused by primary infection with VZV. 51 Three case-control studies on VZV and MS that were conducted in GCC countries were identified, two in Saudi Arabia45,46 and one in Kuwait. 47 All three studies reported that VZV was associated with a statistically insignificant risk for MS.
Mumps
Mumps is a common and highly contagious childhood disease caused by the mumps virus. 52 Only one study was found on mumps and MS, conducted in Kuwait. 47 The study findings showed no association between mumps and MS risk.
Epstein–Barr virus (EBV)
EBV is considered one of the most prevalent human viruses worldwide. EBV belongs to the herpesvirus family. The virus is spread primarily through saliva and causes infectious mononucleosis. 53 Only two studies on EBV and MS were conducted in a GCC country (both in Kuwait), and these reported conflicting results. An epidemiological study showed no association between EBV and MS, 47 whereas a serological study showed a strong association between EBV and MS. 48
Human herpesvirus-6 (HHV-6)
Primary infection with HHV-6 is commonly acquired in childhood and is spread via saliva between children, caregivers, and siblings. HHV-6 viral particles enter through the nasopharynx and olfactory system. 54 Only one study on HHV-6 and MS conducted in a GCC country (Kuwait) was identified. 49 That study reported no association between HHV-6 and MS risk.
Discussion
Two studies conducted in Saudi Arabia found an association between MS and measles,45,46 which is consistent with a case-control study conducted in 2017 in Iran that identified an association between a history of measles and MS.55,56 This is also consistent with a report that a history of measles during childhood increases the MS risk. 57 The association between MS and measles infection has been studied for many years, and this association has been postulated as a host response to viral infection, which may cause the demyelinating and inflammatory lesions in MS. 58 A serological study in Kuwait found that EBV increased the MS risk and the authors identified a strong association between EBV and MS. 48 The findings of that study are consistent with a meta-analysis reporting that a history of infectious mononucleosis more than doubles the risk of MS. 59 It is currently unclear whether EBV is independently associated with MS or whether some other factors predispose an individual to both EBV infection and MS. EBV affects people of all ages, and, after causing an asymptomatic primary infection early in childhood, the virus exists in a latent form in B cells, from which it can later progress to infectious mononucleosis. 60 A strong association between EBV and MS has been demonstrated in various epidemiological 61 and serological studies conducted in Western countries.62,63 The autoimmune reactions in MS may be induced by viral infection, which leads to inflammatory disease in the central nervous system via mimicry or bystander activation. These two mechanisms are not mutually exclusive because, for successful molecular mimicry, viral antigens may have structures that are sequential or similar to self-antigens, and bystander activation is not specific to autoreactive cells because of the inflammatory events that result from infection. 64 Inconsistently, a study in Kuwait found no association between the risk of MS and measles, EBV, or mumps. 47 Moreover, two studies conducted in Saudi Arabia and one study conducted in Kuwait found no association between VZV and MS.45–47 VZV has long been considered a potential etiologic agent of MS, but previous comprehensive reviews analyzing 40 studies did not identify any causal associations. 65 Similarly, a population-based case-control study in Iran (547 cases and 1057 controls) found no association between VZV and MS. 66 A study in Kuwait reported no association between the risk of MS and mumps, consistent with a large-scale case-control study (14,362 cases and 7671 controls). 67 Another study in Kuwait found no association between HHV-6 and MS, which was inconsistent with a recent meta-analysis of 34 molecular studies and seven serological studies showing increased MS risk. 68 Viral infections have long been considered potential risk factors for MS. However, some studies have reported that viral infections such as CMV, HIV, and HCV are negatively associated with MS risk.69–71 There is a disproportionately high migrant worker population in GCC countries, and although this large anomaly could skew all epidemiological research emerging from the region, the relevant studies were conducted almost exclusively among GCC citizens.
We identified and evaluated five published articles on MS and infection conducted in Saudi Arabia and Kuwait. There were no relevant published reports of research conducted in the remaining four GCC countries. The first relevant paper from a GCC country was from Kuwait, published in 2003. 49 Two additional articles were from Kuwait, published in 2013 and 2015;47,48 the two most recent articles included in this review were published in Saudi Arabia in 2018.45,46 The number of published studies of infection and MS risk is relatively low in this region, as compared with that in Western and Middle Eastern countries. Moreover, there is a gap in the literature between 2003 and 2013. This may be because MS was previously considered to be an uncommon disease in GCC countries, although the most recently published papers show that MS is more common than previously realized.72,73 The prevalence of MS in Kuwait is 85 cases per 100,000 individuals, the highest of any GCC country. 74 MS prevalence in the United Arab Emirates is 64.44 cases per 100,000, 75 and that in Qatar is 64.56 cases per 100,000. 76 Global MS prevalence has increased from 30 cases per 100,000 in 2008 to 33 cases per 100,000 in 2013, with significant variation between countries. 77 The highest MS prevalence in the world is in high-income areas: North America with 164.6 cases per 100,000 and in Western Europe with 127 cases per 100,000 individuals. The lowest MS prevalence is found in eastern Sub-Saharan Africa with 2.8 cases per 100,000 and Oceania with 2 cases per 100,000. 78 Countries neighboring the Gulf region, such as Iran and Turkey, have an MS prevalence of 74.28 and 101.4 cases per 100,000 individuals, respectively. 79 Retrospective epidemiological studies were the most commonly published article type, followed by serological studies; thus, there is a need for additional prospective and serological studies on this topic. The present findings also emphasize the need for a regional MS registry in Gulf countries. 80 Importantly, future work on this topic should also investigate the age of infection, as contracting an infection in early life may be a protective factor for MS whereas contracting the same disease at a later age may be a risk factor of MS, 26 given that the development of a normal immune system requires challenges via exposure to infections early in life, which is the basic concept behind the hygiene hypothesis.81–83
Study limitations
The lack of an adequate number of relevant studies from the Arabian Gulf region prevented us from conducting a meta-analysis or even a systematic review. Most published papers included in this review were hospital-based and had limitations such as a small sample size and recall bias. Thus, additional studies regarding the association between infection and MS, using serological tests rather than questionnaires or interviews, are needed to provide more robust evidence.
Conclusion
An association between MS and measles has been reported in Saudi Arabia, and an association of MS with EBV was reported in Kuwait. However, only a few studies on the associations of MS with infectious diseases have been conducted in GCC countries, most of which were epidemiological studies with a small sample size. MS research in the GCC countries is currently far surpassed by that in Western countries. Further longitudinal and serological studies to investigate the relationship between infection and MS are highly recommended, as is creation of an MS regional registry in the GCC countries.
Footnotes
Acknowledgements
The author would like to thank the authors of the studies included in this review as well as Katie Oakley, PhD, from Edanz Group for editing a draft of this manuscript.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.