
Abstract
Complex aortic aneurysms are difficult to treat endovascularly and so techniques have been developed to broaden the management options. We report a case of 51-year-old man with several thoracoabdominal aortic aneurysms (TAAAs) who underwent endovascular repair with “off-label” stent grafts. Three aortic stent grafts and four branched stent grafts were used in the procedure using chimney and periscope techniques. The patient was followed for three years with regular computed tomography angiography (CTA). Scans at 3 and 12 months showed that the TAAAs were repaired and all visceral arteries were patent. Although, scans at the two- and three-year follow-ups showed that the stent graft in the superior mesenteric artery was occluded, the patient did not have any complications probably as a result of coeliac artery compensation.
Introduction
Thoracoabdominal aortic aneurysms (TAAAs) arise from continuous dilatation of the descending thoracic aorta extending into the abdominal aorta. 1 Currently, surgical treatment of TAAAs includes open surgery, hybrid procedures and total endovascular repair. 2 Conventional open surgery for TAAAs is challenging; it requires a highly invasive thoracoabdominal incision and is associated with high rates of perioperative mortality and severe complications.3,4 In recent years, a hybrid procedure has been used to treat thoracoabdominal aortic disease. This approach does not require a thoracoabdominal incision or aortic arch interruption and avoids thoracotomy and cardiopulmonary bypass. Additionally, the duration of spinal cord and visceral ischemia is short, and the incidence of severe complications is significantly reduced. Although the mid- to long-term outcomes of the hybrid procedure are good, the operation is still invasive. Endovascular abdominal aortic aneurysm repair (EVAR) which involves the placement of a stent-graft into the aneurysm is minimally invasive and is associated with lower complication and mortality rates than those of traditional open surgery. Advances in endovascular techniques, including the development of fenestrated, branched and chimney endografts has broadened the management options for extensive aneurysms.5,6
We report here on a three-year follow-up of a male patient with Crawford Type III TAAAs who underwent endovascular repair of aortic aneurysms with composite stent grafts in our department in June 2015.
Case report
This study was approved by the institutional review board of Nanjing Drum Tower Hospital and the patient provided written informed consent.
A 51-year-old male was admitted to hospital with a three-day history of pain in his waist and back which had intensified over the previous eight hours. Physical examination showed the patient to be in good general health with no heart or lung abnormalities and a blood pressure of 140/81mmHg. His abdomen was soft, and no palpable pulsating masses were present. Computed tomography angiography (CTA) of the aorta showed two TAAAs with a maximum diameter of 6.6 cm (Figure 1). Automatic three-dimensional sizing software (EndoSize; Therenva, Rennes, France) was used to evaluate the diameter and relative relationship of the aorta and its branches. The patient was characterised as having Type III TAAAs (i.e., aneurysms involve the distal thoracic aorta to the aortoiliac bifurcation).
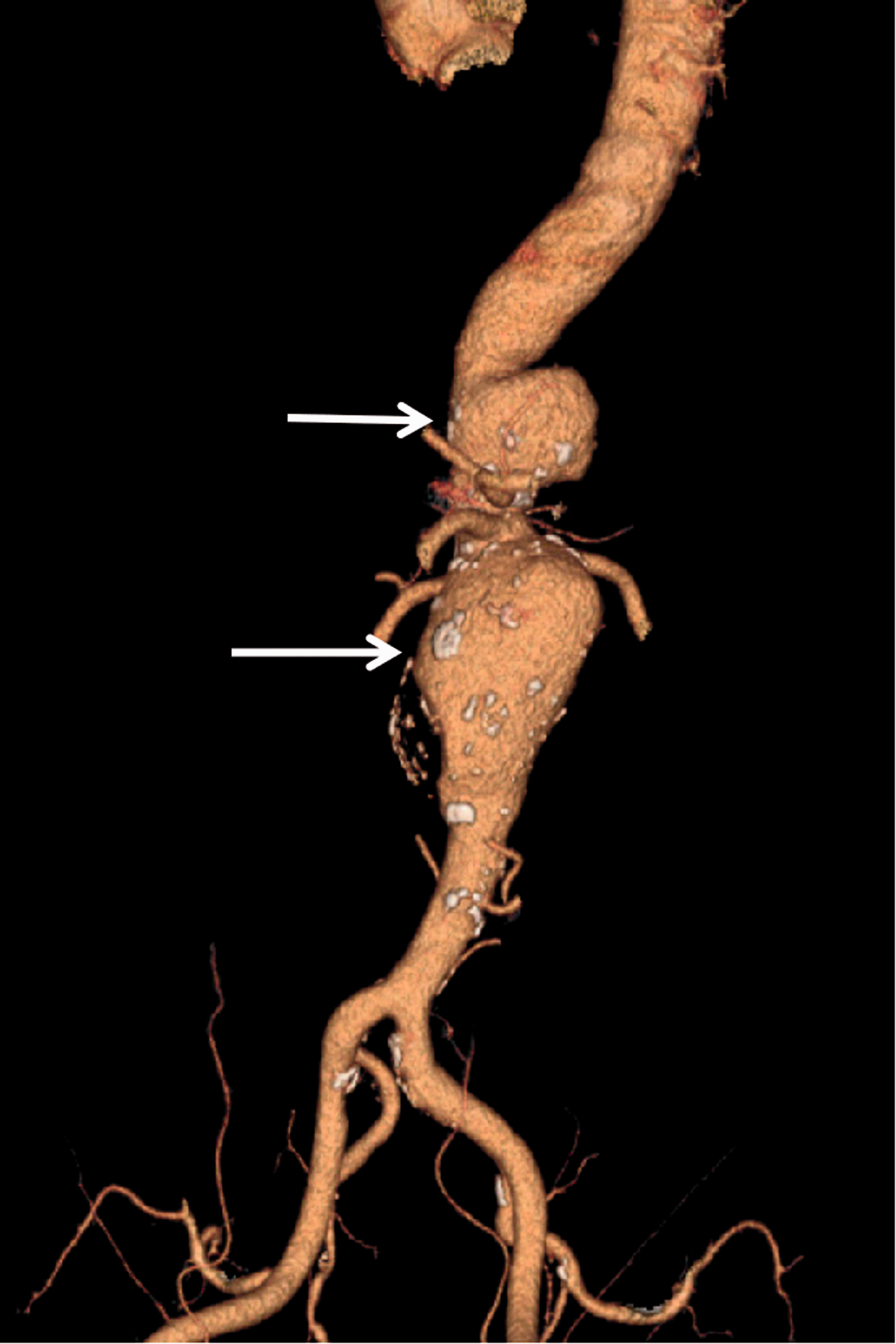
Computed tomography angiography (CTA) three-dimensional (3D) reconstruction showing two thoracoabdominal aortic aneurysms (TAAAs) as indicated by arrows.
Under general anaesthesia, bilateral inguinal and left brachial arterial incisions were made and a long 10-F sheath catheter was passed from the left brachial artery to the descending aorta. Following confirmatory CTA, a 9 × 150 mm covered stent graft (VIABAHN, Gore, Inc., USA) was passed into the truncus coeliacus under the protection of the long catheter. Subsequently, a 34 × 100 mm covered stent graft (Tag, Gore, Inc., USA) was introduced from the right femoral artery. The two stent grafts were released successively. Imaging showed there were no endoleaks and the truncus coeliacus was patent. Two covered stent grafts (24 × 80 mm and 28 × 80 mm; Endurant, Medtronic, Inc., USA) were placed from the femoral artery to the distal abdominal aorta. In addition, two long 8-F control catheters (FuStar, Lifetech, Inc., China) were placed from the left femoral artery, a long 9-F control catheter was deployed in the left brachial artery, and under the protection of three long catheters, a 9 × 100 mm covered stent graft (VIABAHN, Gore, Inc., USA) was placed in the superior mesenteric artery, a 7 × 100 mm covered stent graft (VIABAHN, Gore, Inc., USA) was placed in the left renal artery, and an 8 × 100 mm covered stent graft (VIABAHN, Gore, Inc., USA) was placed in the right renal artery (Figure 2).

A diagram of the operative approach. [CA, carotid artery; SMA, superior mesenteric artery; RRA, right renal artery; LRA, left renal artery]
Following their positioning, all small stent grafts were deployed and balloon dilatation performed. Repeat CTA showed that all stent grafts were in position, the primary aneurysm had disappeared, and the visceral arteries showed no evidence of endoleaks. Approximately 500 ml of blood was lost during the procedure and haemoglobin levels changed from 12.8 to 11.5 g/dl. The total operation time was 300 minutes and the patient returned to a general ward post-surgery.
Low-molecular-weight heparin was used post-operatively for three days and electrocardiographic monitoring was stopped one day after the operation. The patient was encouraged to get out of bed and walk around as soon as possible and was discharged from hospital one week after the procedure. Long-term oral treatment with rivaroxaban tablets (5 mg/day) and clopidogrel (75 mg/day) was prescribed.
CTA of the aorta 30 days after surgery showed that the stent grafts were in good condition, there were no endoleaks and the truncus coeliacus, superior mesenteric artery and bilateral renal arteries were unobstructed. CTA of the aorta 3- and 12-months (Figure 3) post-operation showed that the stent grafts were viable and all visceral arteries were unobstructed. After 12 months, clopidogrel was stopped and the patient received aspirin for antiplatelet treatment. CTA of the aorta two years post-operation showed that the truncus coeliacus and renal arteries were unobstructed. However, the stent graft in the superior mesenteric artery was occluded with a thrombus (Figures 4–6).

Computed tomography angiography (CTA) three-dimensional (3D) reconstruction one year after the operation showing that the visceral arteries were unobstructed. [CA, carotid artery; SMA, superior mesenteric artery; RRA, right renal artery; LRA, left renal artery]

Computed tomography angiography (CTA) three-dimensional (3D) reconstruction two years after the operation showing that the stent graft in the superior mesenteric artery was occluded with a thrombus (arrow).

Computed tomography (CT) scans showing the stent graft in the superior mesenteric artery was occluded with a thrombus (arrows).

Computed tomography (CT) scans showing the stent graft in the superior mesenteric artery was occluded with a thrombus (arrows).
The patient had no symptoms and refused to undergo any further surgical treatment. It was thought that the blood supply of the superior mesenteric artery was compensated by the truncus coeliacus. CTA of the aorta three years post-operation was similar to the two-year observations and follow-up is continuing.
Discussion
Although endovascular options provide a less invasive approach and more favourable outcomes than open surgery in the management of TAAAs, more than 30% of patients are not suitable for conventional endovascular repair because of anatomic constraints around the proximal neck. 7 However, a number of endovascular techniques and devices have been developed to bypass these challenges. These include, branched, fenestrated and chimney stent graft techniques. 7
The first successful use of a branched stent-graft to preserve the visceral artery and perform complete endovascular treatment of a TAAA was reported by Chuter et al. 8 in 2001. The method avoided aortic interruption and the duration of spinal cord and visceral ischemia was short. First reported in 1999, fenestrated endografts were developed to treat patients with aneurysms with short proximal necks. 9 The chimney graft which was first reported in 2003 by Greenberg and colleagues, describes the placement of a covered stent into a branch vessel with the proximal part of the stent extending above the proximal edge of the main aortic stent graft. 6 In 2008, Ohranlander et al. 10 successfully used the chimney technique with commercially available covered stents to retain the visceral arteries in the treatment of 10 cases of complicated TAAAs. There were no endoleaks eight months after the operation.
Complex aortic aneurysms are difficult to treat endovascularly and so creative solutions such as the octopus and multi-chimney techniques have been devised. These techniques use ‘off the shelf’ stents and so there is no need to customize or modify the stent during the procedure. 11 In a two-year follow-up of 77 patients that had undergone endovascular treatment for complex aneurysms, Lachat et al. 12 reported that of the 169 target vessels that were revascularized, only four stents were blocked and only three endoleaks occurred.
This was one of the earliest cases of TAAA repair undertaken in our department. Considering the technical challenges facing us in 2015, we decided to use a phased composite stent-graft technique. The operation was performed in a hybrid operating room. Initially, a single-chimney technique was used to reconstruct the coeliac artery. A single-chimney technique was also used to reconstruct the superior mesenteric artery but a double-periscope technique was used to reconstruct the bilateral renal arteries. If any technical difficulties, such as branch failure or stent graft release failure, occurred, the procedure could have been quickly converted to open surgery to reconstruct the remaining visceral artery as long as the chimney stent graft was preserved. The most important post-operative complication of the chimney technique is Type I endoleaks, 13 and the placement of several large chimney stent grafts is thought to increase the possibility of endoleaks. However, we used a phased composite stent-graft technique and so reduced the likelihood of Type I endoleakage. At the same time, only three surgical approaches were required which simplified the procedure and reduced the possibility of surgical trauma.
The short-term outcome in this patient was good, but over the mid- to long-term post-operative period the stent in the superior mesenteric artery became occluded by the large stent graft. Fortunately, no serious complications occurred which was probably due to coeliac artery compensation. The results of this case history suggest that in the endovascular repair of TAAAs, all visceral arteries should be reconstructed as much as possible and that branch stent grafts should not be too long. Moreover, when using covered branched stent grafts, bare stent grafts should be placed simultaneously because the stent graft material is soft and the combination of stents will ensure long-term stent graft support.
Although managing TAAAs by endovascular repair was a novel technique in our department in 2015, we achieved a satisfactory clinical effect and determined that the method was suitable for treating various aortic diseases involving the visceral arteries. In theory, the chimney technique (including the octopus and periscope techniques) and our modified composite stent-graft technique can be applied to all types of TAAAs as long as guidewire access can be established. This present report is based on one case study. Further controlled, prospective studies are required and different stent graft approaches for complex TAAA repair should be compared.
Footnotes
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.