
Abstract
Objective
Neuropsychiatric systemic lupus erythematosus (NPSLE) is a manifestation of systemic lupus erythematosus (SLE). Central nervous system (CNS) infection is a consequence of intensive immunosuppressive therapy that patients with SLE might undergo. This study aimed to compare the differences between NPSLE and CNS infections in patients with SLE.
Methods
Patients with SLE and NPSLE or CNS infections were retrospectively reviewed. Clinical manifestations, laboratory test results, and prognoses were recorded. The independent sample t-test or chi-square test was used to compare data.
Results
Patients with CNS infections (n = 20) had more serious headache, high fever (>39.0°C), and vomiting compared with patients with NPSLE (n = 48). Patients with CNS infections also had a larger prednisone dose at the time of symptom onset, larger cumulative dosages over the preceding year, lower SLE Disease Activity Index (SLEDAI) scores, higher rate of nephritis, lower albumin levels, higher C-reactive protein (CRP) levels, higher 24-h-urine protein levels, higher cerebrospinal fluid (CSF) white blood cell levels, and lower protein and glucose levels than those with NPSLE.
Conclusions
For patients with SLE presenting with CNS symptoms, serious headache, high fever, a high dose of corticosteroids, low SLEDAI scores, and abnormal CSF are more important indicators for CNS infections than NPSLE.
Keywords
Introduction
Patients with systemic lupus erythematosus (SLE) have an increased susceptibility to infections, either from disease-related immunological dysfunction or the effects of immunosuppressive therapies on the immune system. These infections include viral, bacterial, fungal, and parasitic infections involving multiple organs. 1 Central nervous system (CNS) infections in patients with SLE are rare, affecting only 1.4% of patients, 2 but a death rate of higher than 40% has been reported in these patients.3,4 Neuropsychiatric systemic lupus erythematosus (NPSLE) is a generic definition referring to a series of neurological and psychiatric symptoms that are directly related to SLE. Because of a lack of a gold standard, NPSLE represents a clinical challenge that obligates the strict exclusion of any other potential cause. In some cases, the manifestations of CNS infection and NPSLE are similar, which may delay diagnosis and treatment. This retrospective study evaluated the clinical profiles and outcomes of 68 patients with SLE who were hospitalized with CNS infections or NPSLE. This study aimed to identify some factors for discrimination of CNS infection and NPSLE.
Patients and methods
We retrospectively reviewed inpatient medical records of patients with SLE who were admitted to the Fifth and Six Affiliated Hospitals of Wenzhou Medical University from January 2007 to January 2016. All cases fulfilled the requirement of the 1997 revised American College of Rheumatology (ACR) classification criteria for SLE. 5 CNS infection was diagnosed according to the patient’s clinical manifestations, cerebrospinal fluid (CSF) examination results, pathogen tests, and responses to anti-infective treatment. NPSLE was defined as patients with SLE who had neuropsychiatric (NP) manifestations according to Systemic Lupus International Collaborating Clinics classification for NP lupus syndromes, with the exclusion of other diseases by a rheumatologist, neurologist, and psychiatrist.6,7 Patients in whom making a definite diagnosis was difficult were excluded. The study protocol was approved by Lishui ethics review committee. The patients provided verbal consent to participate.
The severity of headaches was classified as mild, moderate, and severe according to the International Headache Society criteria. 8 SLE disease activity was calculated according to the SLE Disease Activity Index (SLEDAI). 9 Laboratory data, such as white blood cells (WBCs), serum creatinine (Scr), the erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), albumin, anti-phospholipid antibodies (aPLs), complement 3 (C3), and immunoglobulin G (IgG) were collected. CSF and magnetic resonance imaging (MRI) examinations were performed.
Variables are described as mean and standard deviation or proportion. We used the independent sample t-test or chi-square test to compare demographic features and laboratory data between the two groups. A P value of <0.05 was considered statistically significant. All statistical analysis was performed using SPSS 17 (IBM, Cary, NC, USA).
Results
From January 2007 to January 2016, 48 patients with NPSLE (44 females) and 20 patients with SLE complicated by CNS infection (20 females) among 1700 patients with SLE were included. The causative microorganisms in the 20 patients with SLE and CNS infection are shown in Table 1. Among the 20 patients with CNS infections, Cryptococcus neoformans was the most common in 12 patients, Mycobacterium tuberculosis (TB) was found in four patients, Listeria monocytogenes in two patients, and Klebsiella pneumoniae in two patients. One patient with TB meningitis also had pulmonary TB.
Aetiology of CNS infection in patients with SLE

SLE: systemic lupus erythematosus; CNS: central nervous system.
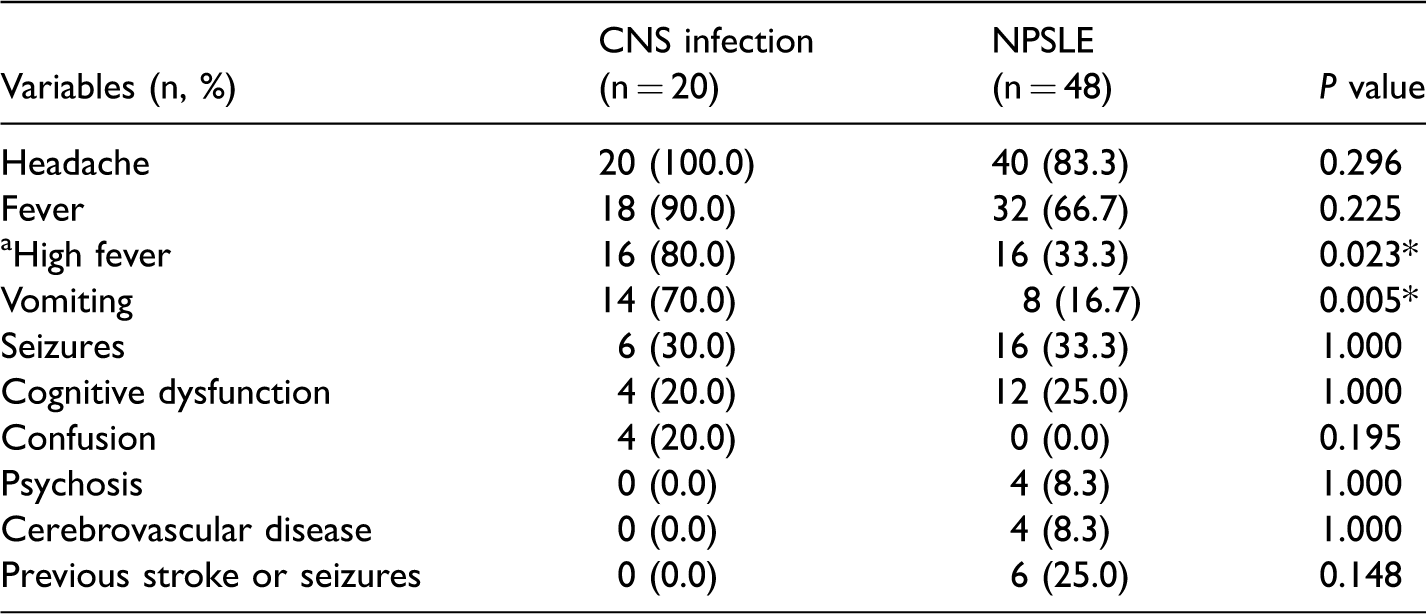
Clinical features at presentation for the patients with SLE and CNS infections and those with NPSLE are shown in Table 2. Headache was the most common symptom in the CNS infection and NPSLE groups. Patients with CNS infections had moderate to severe headaches (80%), while patients with NPSLE had mild to moderate headaches (70%). The duration of headaches in patients with NPSLE was usually less than 1 week. In patients with CNS infections, with the exception of four who died, headaches were usually relieved after 2 weeks.
Clinical features in patients with SLE and CNS infection and those with NPSLE
SLE: systemic lupus erythematosus; CNS: central nervous system; NPSLE: neuropsychiatric systemic lupus erythematosus.
Temperature >39.0°C.
P < 0.05.
Fever was the second most common presenting clinical feature in the CNS and NPSLE groups. A significantly greater percentage of patients with CNS infections had high fever (> 39.0°C) and vomiting than did patients with NPSLE (P = 0.023 and P = 0.005, respectively). There were no significant differences in the rates of seizures, cognitive dysfunction, confusion, psychosis, cerebrovascular disease, and previous stroke or seizures between the two groups.
There were no differences in sex, age, duration of lupus disease, rate of methylprednisolone pulse therapy, or rate of immunosuppressive therapy (cyclophosphamide and mycophenolate mofetil) over the preceding year between patients with SLE and CNS infections and those with NPSLE (Table 3). Patients with CNS infections had a longer interval between symptom onset and establishment of diagnosis, a larger prednisone dose at the time of symptom onset, a larger cumulative prednisone dose over the preceding year, lower SLEDAI scores, and a higher rate of nephritis compared with patients with NPSLE. The incidence of death was 20% (4 died) in the CNS infection group and 0% (0 died) in the NPSLE group (P = 0.006).
Clinical characteristics in patients with SLE and CNS infection and those with NPSLE

SLE: systemic lupus erythematosus; CNS: central nervous system; NPSLE: neuropsychiatric systemic lupus erythematosus; F: female; M: male; SLEDAI: SLE Disease Activity Index.
Data shown are mean ± SD (standard deviation) or n (%).
P < 0.05
Laboratory and radiological findings are shown in Table 4. Patients with CNS infections had significantly lower albumin levels, and higher CRP levels and 24-h urine protein levels compared with patients with NPSLE. Patients with CNS infections had a significantly higher CSF opening pressure, CSF WBC count, and protein levels, and lower glucose levels compared with patients with NPSLE. There were no differences in the WBC count, levels of Scr, C3, IgG, aPLs, anti-ribosomal P, and CSF chloride, ESR, and MRI abnormalities between the two groups. MRI abnormalities were aspecific in both groups.
Laboratory and radiological findings in patients with SLE and CNS infection and those with NPSLE

SLE: systemic lupus erythematosus; CNS: central nervous system; NPSLE: neuropsychiatric systemic lupus erythematosus; WBC: white blood cell; Scr: serum creatinine; ESR: erythrocyte sedimentation rate; CRP: C-reactive protein; C3: complement 3; IgG: immunoglobulin G; aPLs: anti-phospholipid antibodies, including lupus anticoagulant, anticardiolipin, and anti-β2-glycoprotein I; CSF: cerebrospinal fluid; MRI: magnetic resonance imaging.
Data shown are mean ± SD (standard deviation) or n (%).
P < 0.05.
Discussion
NPSLE can be a severe and troubling manifestation of a disease that greatly affects the patient’s health and disease outcome. 10 Patients with SLE are vulnerable to infections, and CNS infections are considered to have a poor prognosis.3,11,12 However, the clinical presentation does not allow discernment between primary CNS involvement of SLE and CNS infection because the signs and symptoms, and laboratory and MRI findings are non-specific.13–16 Therefore, neuropsychiatric involvement makes differential diagnosis especially difficult.
In this study, we compared the clinical features of patients with SLE and CNS infection and those with NPSLE. Among the 20 patients with CNS infections, C. neoformans and M. tuberculosis accounted for 80% of infections, which is consistent with previous studies.4,6,11 However, there were no viral infections, possibly because of the small number of samples. We found that patients with CNS infections had more serious headache and the duration of headache was longer compared with patients with NPSLE. Lupus headache is defined as a severe, persistent headache that may be migrainous and nonresponsive to narcotic analgesia. 17 However, most patients with NPSLE in this study could tolerate a migrainous headache, possibly because of the normal intracranial pressure. Additionally, this headache appeared to disappear soon after glucocorticoid use.
In our study, patients with SLE and CNS infections had lower SLEDAI scores than did those with NPSLE. Patients with SLE and CNS infections often had higher dosages of corticosteroids before infections, suggesting that a large dose corticosteroid therapy was a vital predictor for CNS infection in patients with SLE. Among patients with CNS infections, 80% had nephritis and 24-h urine protein levels were significantly higher than those in patients with NPSLE. Previous studies also showed a higher incidence of nephritis in patients with CNS infections, 18 but there may be no direct association between them. Patients with nephritis usually require a higher dose and longer duration of corticosteroid therapy than those without nephritis, which may be the major cause of infection.
Patients with CNS infections had a longer time to diagnosis compared with patients with NPSLE. This finding indicates that the presentation of CNS infection in patients with SLE is more complicated and atypical than in those with NPSLE. 3 Although more effective treatments have been developed in the past 10 years, patients with CNS infections had a higher mortality rate than those with NPSLE.
Patients with SLE and CNS infections had a significant elevation in CSF leukocyte numbers and protein levels compared with those with NPSLE. However, in patients with NPSLE, changes in CSF were mild; CRP levels were much higher in patients with SLE and CNS infection, and the ESR appeared to be higher in patients with NPSLE, but this was not significant. These findings are consistent with previous research.19–21
The present study shows that, generally, serious headache, high fever, high intake of corticosteroids, lower SLEDAI scores, and abnormal CSF findings could help distinguish CNS infections from NPSLE. However, comprehensive evaluation, including clinical manifestations, laboratory tests, and radiological findings, are required.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.