
Abstract
Objective
To investigate the effect of hypothermia on the pharmacokinetics and pharmacodynamics of nimodipine in rabbits using in vivo and in vitro methods.
Methods
Five healthy New Zealand rabbits received a single dose of nimodipine (0.5 mg/kg) intravenously under normothermic and hypothermic conditions. Doppler ultrasound was used to monitor cerebral blood flow, vascular resistance, and heart rate. In vitro evaluations of protein binding, hepatocyte uptake and intrinsic clearance of liver microsomes at different temperatures were also conducted.
Results
Plasma concentrations of nimodipine were significantly higher in hypothermia than in normothermia. Nimodipine improved cerebral blood flow under both conditions, but had a longer effective duration during the hypothermic period. Low temperature decreased the intrinsic clearance of liver microsomes, with no change in protein binding or hepatocyte uptake of nimodipine.
Conclusion
Nimodipine is eliminated at a slower rate during hypothermia than during normothermia, mainly due to the decreased activity of cytochrome P450 enzymes. This results in elevated system exposure with little enhancement in pharmacological effect.
Introduction
Hypothermia is defined as a central temperature ≤36℃, and is classified into three types: mild (34–36℃), moderate (30–34℃) and severe (<30℃). Whether accidental or intentional, hypothermia can be induced by a variety of chemical or physical interventions, such as sustained low temperature, severe trauma, shock, anesthesia, and infusion of a large amount of fluid.1,2 Reduction of body temperature suppresses a broad range of pathological and physiological processes, especially those involving energy consumption. Negative effects include lowering oxygen and glucose demands, interruption of apoptotic pathways, inhibition of pro-inflammatory cytokines, and blocking of neuroexcitatory cascades. 3 As a result, hypothermia is neuroprotective and can be used to treat focal and global ischemic brain injury. 4 Indeed, intentional hypothermia, often referred to as “therapeutic hypothermia”, has been translated into clinical practice to improve neurological outcomes in many hypoxic–ischemic diseases including cardiac arrest, neonatal encephalopathy, traumatic brain injury, convulsive status epilepticus, myocardial ischemia, spinal cord injury and subarachnoid hemorrhage.5,6
Certain physiological processes that mediate drug metabolism, disposition and response also need energy, and are vulnerable to theoretically unavoidable temperature-induced changes in drug pharmacokinetics and pharmacodynamics, which may increase the occurrence of unanticipated adverse drug effects. 7 In practice, there is a large body of preclinical and clinical evidence for altered drug disposition during hypothermia. For example, the expression and activity of a variety of metabolic enzymes and transporters such as cytochrome P450 (CYP) 2C9, CYP2E1, CYP3A2, CYP3A4 and permeability glycoprotein (P-gp) may change at a low temperature. 8 Hypothermia can reduce the elimination of a number of xenobiotics and endogenous substances, such as ethanol, general anesthetics (rocuronium and atracurium), macrolide antibiotics (gentamycin), antiepileptic drugs (phenytoin), antidepressant drugs (phenobarbitone), glycine and glutamate. 9 Hypothermia also leads to changes in the pharmacodynamic profile of drugs such as phenobarbitone, pancuronium bromide and furosemide. 10
Coupled with therapeutic hypothermia, critically ill patients are often subjected to a wide variety of medications. Many of these drugs have narrow therapeutic windows and have not been thoroughly studied under hypothermic conditions. 11 As a result, the success or failure of this promising intervention depends largely on rational drug dose adjustments by clinicians based on evidence and on an intimate knowledge of drug interactions.
Nimodipine is a dihydropyridine-like calcium channel antagonist that selectively dilates cerebral arteries and increases cerebral blood flow in animals and humans. 12 Its major therapeutic indication is the prevention and treatment of delayed ischemic neurological disorders that often occur in patients with subarachnoid hemorrhages. 13 Matsumoto et al. 14 have demonstrated that nimodipine combined with therapeutic hypothermia increases the beneficial effects in neurological outcomes. However, no information is currently available regarding either the possible changes of in vivo exposure and response to nimodipine under conditions of therapeutic hypothermia, or the specific mechanisms underlying these changes. The objectives of the present study, therefore, were a) to investigate the effects of hypothermia on the pharmacokinetics and pharmacodynamics of nimodipine in rabbits; and b) to identify the mechanisms underlying alterations in systemic clearance by in vitro evaluation of the effects of hypothermia on nimodipine protein binding, hepatocyte uptake and intrinsic clearance (CLint) of rabbit liver microsomes.
Materials and methods
Drugs and reagents
The following drugs/reagents were used in the study: nimodipine for injection (batch no. EXG2G31; Bayer HealthCare Corporation, Beijing, China), nimodipine standard (batch no. 100270-200002; National Institute for the Control of Pharmaceutical and Biological Products, Beijing, China), aconitine (Sigma–Aldrich, St Louis, MO, USA), 1-aminobenzotriazole (Sigma–Aldrich), methanol, acetonitrile (chromatography grade; SK chemicals, Seoul, Korea); all other reagents and solvents were analytical grade.
Animal experiments
Five male New Zealand rabbits weighing 2.2–2.6 kg (age: 120 days) were purchased from Vital River Ltd. (Beijing, China). As estrogens are potent and efficacious neuroprotectants, 15 only male animals were used in this study. All rabbits were raised in an atmosphere where the temperature was 22 ± 1℃ and humidity was 60 ± 10%. The study was approved by the Ethics Committee of the Navy General Hospital and conducted in accordance with Chinese GLP standards. Rabbits were fasted for 12 h before surgery with free access to water.
In the first period of studies at normal body temperature, rabbits were placed on the operating table in the prone position. Skin preparation and sterilization were conducted in the parietal region of the skull. After anesthesia, a vertical incision of about 5 cm was made. The skin was retracted, and a rounded bone window about 0.8 cm in diameter was made in the parietal region of the skull using a hand drill. The periosteum was then carefully removed with tweezers, and the wound was waxed to stop bleeding. The cerebral dura was kept intact, while a Doppler ultrasound probe (Acuson Sequoia 512, Siemens America, Malvern, PA, USA) was placed in the rounded bone window to record the cerebral blood flow image and the quantitative pharmacodynamic data including the velocity of the cerebral arterial blood flow, vascular resistance, and heart rate. The rectal temperature of each rabbit was monitored throughout the experiment with a mercury thermometer.
Rectal temperature and heart rate of rabbits under normothermic or hypothermic conditions (mean ± SD, n = 5).

P < 0.01 vs. normothermia.
Drug administration
During each hypothermic period, a single dose (0.5 mg/kg) of nimodipine was injected intravenously into the inner ear vein 20 min after rectal temperature stabilization. A blood sample (1 mL) was collected from the contralateral ear vein before and 0.167, 0.33, 0.5, 1, 2, 4, and 6 h after drug administration. The sample was placed in a heparin tube, and centrifuged at 3500 × g for 10 min. The plasma was carefully drawn and kept at −80℃.
Nimodipine analysis
An LC–MS/MS spectrometer (Xevo TQ MS system, Waters, Milford, MA, USA) was used to measure the plasma concentration of nimodipine. Aconitine was added as an internal standard and an aliquot of 0.2 mL plasma was subjected to extraction with 1 mL extraction liquid (n-hexane: ether = 1:1) for 2 min, then centrifugation at 3500 × g for 3 min. The supernatant was collected and placed into another centrifuge tube, while the residue was extracted again using the method described above. The mixed extraction liquid was then evaporated with nitrogen at 40℃. The residue was dissolved with 200 µL mobile phase, then centrifuged at 3500 × g for 15 min. A 10 -µL volume of supernatant was injected into the LC–MS/MS system for quantitative analysis.
Chromatographic conditions were as follows: ACQUITY BEHC18 column (2.1 × 100 mm, 1.7 µm); column temperature, 35℃; sample room temperature, 10℃; mobile phase, methanol:water (65:35,v/v); flow rate, 0.3 mL/min. The main working parameters for the mass spectrum were set as follows: ion source, electrospray ionization; capillary voltage, 3.0 kV; cone hole voltage, 18 V; atomization flow rate, 800 L/h; cone hole flow rate, 30 L/h; source temperature, 400℃. Quantification was performed using the MRM method in a positive ion mode with transitions of m/z 419.2→343.1 (collision energy 24 V) for nimodipine and m/z 646.2→586.2 (collision energy 30 V) for aconitine.
Protein binding analysis
Protein binding of nimodipine in rabbit plasma was determined using the equilibrium dialysis method. Plasma was collected from normal rabbits and stored at −80℃ until experimentation. Nimodipine was mixed with rabbit plasma to reach a final concentration of 10 µg/mL and 500 -µL aliquots were placed into the sample chambers of the rapid equilibrium dialysis system (Thermo Fisher Scientific Inc., Rockford, IL, USA) equipped with a dialysis membrane (molecular weight cut-off, ∼8000) to separate the sample chamber and the buffer chamber. The buffer chamber was filled with 750 µL phosphate-buffered saline (0.1 M pH 7.4). The samples (n = 4 per temperature group) were incubated for 18 h at 37℃, 32℃ or 28℃ using a shaking water bath. The nimodipine concentrations in both chambers were determined using the method described above. The unbound fraction ratio (
Enzyme kinetics analysis
Rabbit liver microsomes were purchased from BD Biosciences (Woburn, MA, USA). All reaction mixtures (0.1 mL) contained 400 µg/mL of microsomal protein, phosphate-buffered saline (0.1 M pH 7.4), MgCl2 (2 mM) and 1 mM reduced nicotinamide adenine dinucleotide phosphate (NADPH). Nimodipine was added at increasing final concentrations of 0.023, 0.068, 0.21, 0.62, 1.9, 5.6, 16.7, and 50 µM. These samples were incubated for 5 min at 37℃, 32℃ or 28℃ in a circulating water bath. Preliminary experiments showed that the nimodipine concentration decreased linearly for 5 min at each temperature (data not shown). The reaction was quenched by adding 200 µL acetonitrile containing internal standard. After centrifugation at 20,000 × g for 10 min at 4℃, the nimodipine concentration in the supernatants was determined by LC–MS/MS as described above. The rate of metabolism (v) of nimodipine in the incubation sample was calculated using the following equation:

The Michaelis–Menten constant (Km) and maximum velocity (Vmax) were calculated using OriginPro 9.0 (OriginLab Corp, Northampton, MA, USA) via nonlinear regression by fitting the raw data to the Michaelis–Menten equation:

Considering the nimodipine concentration in vivo is lower than 
The in vivo hepatic intrinsic clearance (
Hepatocyte uptake analysis
To investigate the effects of temperature on hepatic uptake, cryopreserved New Zealand white rabbit hepatocytes (male donor, XenoTech, Kansas City, KS, USA) were diluted with Krebs–Henseleit buffer containing 5 mM 1-aminobenzotriazole to inhibit metabolism by CYP as a “suicide substrate.” 16 After preincubation at 37, 32 or 28℃ for 30 min, nimodipine was added to the incubation systems (1 × 106 cells/ml) at increasing final concentrations of 0.08, 0.24, 0.73, 1.56, 3.13, 6.25, 12.5, 25 and 50 µM. After 1 min incubation, the samples were centrifuged immediately at 15,000 × g for 1 min at 4℃. The nimodipine concentration in the supernatant was determined, and the rate of uptake (v) of nimodipine was calculated using equation 2.
Statistical analysis
Noncompartmental analysis in WinNonlin v. 33 (Pharsight Corp, Mountain View, CA, USA) was used to calculate the pharmacokinetic parameters of nimodipine. All data are expressed as mean ± standard deviation (
Results
Effect of hypothermia on the pharmacokinetics of nimodipine
The standard curves for nimodipine in rabbit plasma were linear from 1 to 1000 ng/mL. Precision and accuracy were consistent with the requirements for quantitative analysis. The mean plasma concentration–time profiles in rabbits under normothermia and hypothermia after single intravenous administration of 0.5 mg/kg nimodipine are shown in Figure 1 and the corresponding pharmacokinetic parameters are presented in Table 2. Compared with the normothermic period, pharmacokinetics of nimodipine in the hypothermic period showed significantly greater plasma concentration, area under the curve (2239.54 vs 512.67 ng/mL h), half life (3.95 vs 2.29 h), mean residence time (4.44 vs 2.10 h), peak plasma concentration (902.34 vs 343.07 ng/mL), and a significant decrease in apparent distribution volume (0.835 vs 1.65 L) and systemic clearance (0.58 vs 2.34 L/h).
Mean plasma concentration–time profile of nimodipine in rabbits under normothermic and hypothermic conditions after single intravenous administration of nimodipine 0.5 mg/kg (mean ± SD, n = 5). aP < 0.05, bP < 0.01, vs. normothermia. Main pharmacokinetic parameters of rabbits under normothermic or hypothermic conditions after single intravenous administration of nimodipine 0.5 mg/kg (mean ± SD, n = 5). t1/2: Elimination half life; Vd: apparent volume of distribution; AUC(0−t): area under the curve; CLs: systemic clearance; MRT: mean residence time; Cmax: maximum plasma concentration.

Effect of hypothermia on the pharmacodynamics of nimodipine
Doppler results showed that the cerebral blood flow in the normothermic period (Figure 2(a)) was better than that in the hypothermic period (Figure 2(c)). However, after administration of a single intravenous dose of nimodipine, the cerebral blood flow in both periods (Figure 2(b, d)) was significantly better than before administration.
Ultrasound image of cerebral blood flow in a rabbit under normothermic and hypothermic conditions. (a, c) Cerebral blood flow in normothermia (a) and hypothermia (c) before intravenous administration of nimodipine. (b, d) Cerebral blood flow in normothermia (b) and hypothermia (d) 10 min after administration of intravenous nimodipine.
The time-averaged maximum velocity (TAMX) and resistive index (RI) in both periods increased soon after nimodipine administration. TAMX and RI during hypothermia were slightly, but not significantly, higher than during normothermia, except RI at 0.16 and 4 h (Figure 3). However, the time these values took to fall to baseline was different between the two periods (TAMX: 1 h and RI: 2 h for normothermia; TAMX: 4 h and RI: 6 h for hypothermia). No change in heart rate was observed in either period (Table 1).
TAMX (a) and RI (b) of rabbits in normothermia or hypothermia (mean ± SD, n = 5). TAMX: time-averaged maximum velocity, RI: resistive index.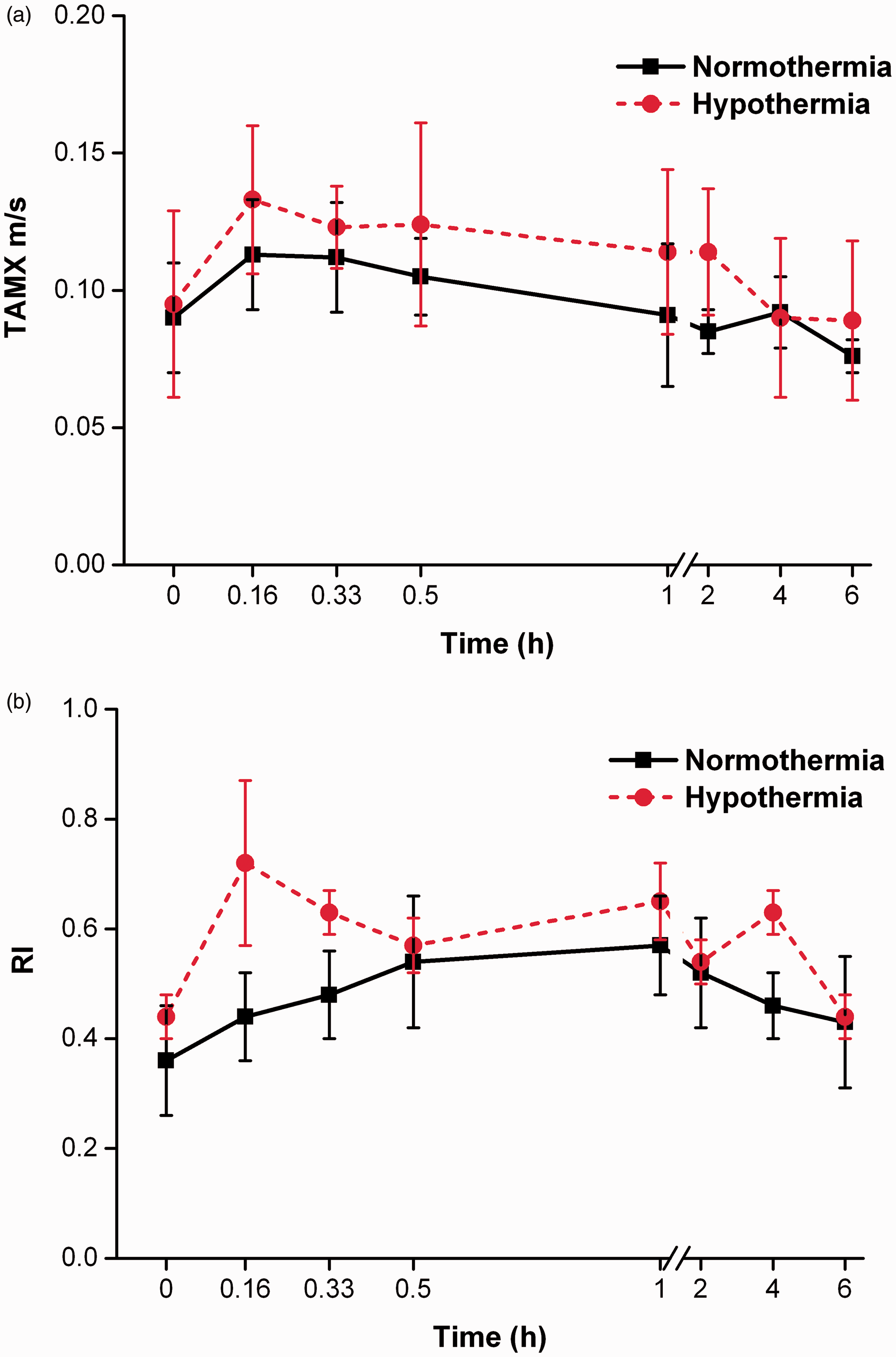
Alteration in the unbound fraction ratio of nimodipine in rabbit plasma at low temperatures
The
Effect of temperature on nimodipine metabolism in rabbit liver microsomes
Figure 4 shows the Michaelis–Menten plot for nimodipine elimination from rabbit liver microsomes. The Km and Vmax at 37, 32 or 28℃ were obtained from the Michaelis–Menten equation. No significant changes were observed in Km at 37, 32 or 28℃ (Table 3). However, the Vmax of nimodipine was ∼34% lower at 32℃ and ∼62% lower at 28℃ than that at 37℃. Correspondingly, the same differences were observed when CLint invitro was calculated using equation 4, and in vitro to in vivo extrapolation of CLint was performed using equation 5, where microsomal protein content had been estimated as 45 mg of protein/g of liver and the average weight of the liver in our rabbits was estimated as 77 g/2.5 kg of body weight.
17
Michaelis–Menten plot for the metabolism rate of nimodipine in rabbit liver microsomes at 28, 32 and 37℃. Each value is the mean ± SD of three experiments. Solid lines represent best fit: 28℃ (□), 32℃ (▴) and 37℃ (○). Kinetic parameters of nimodipine metabolism in rabbit liver microsomes and uptake in rabbit hepatocytes at 28, 32 and 37℃. Vmax: maximum velocity; Km: Michaelis–Menten constant; CLint invitro: in vitro intrinsic clearance; CLint invivo: in vivo intrinsic clearance; K: slope of curve. Each value is the mean ± SD of three experiments. P < 0.01 vs. 37℃. P < 0.01 vs. 32℃.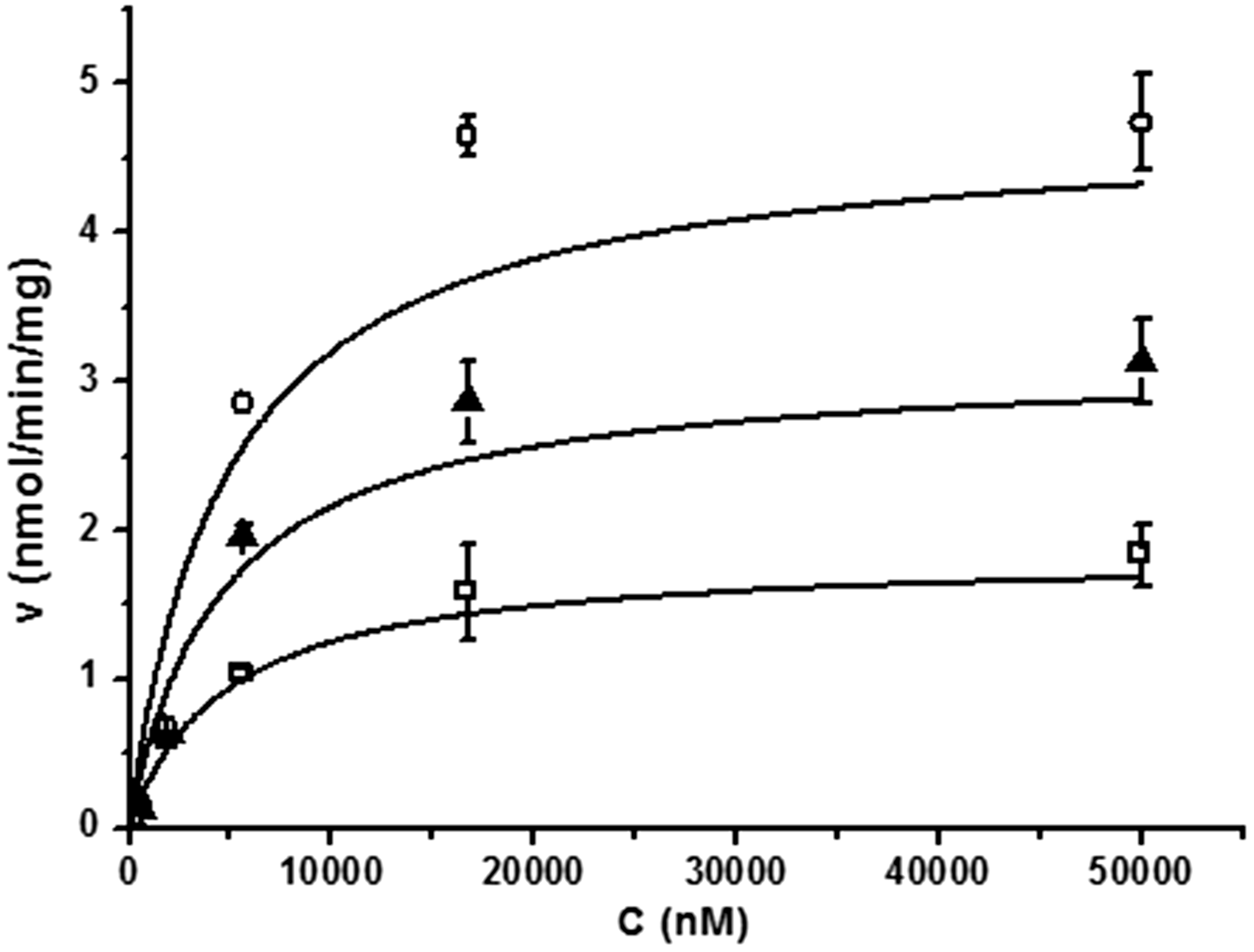

Effect of temperature on nimodipine uptake in rabbit hepatocytes
To determine the effects of temperature on nimodipine uptake in rabbit hepatocytes, the nimodipine concentration in supernatants was determined at different temperatures in the presence of a CYP inhibitor. The rate of nimodipine uptake in rabbit hepatocytes increased linearly at concentrations below 50 µM (Figure 5) and neither the uptake rate at different concentrations nor the slope of the curve (k) (Table 3) differed significantly between the two temperature groups.
Uptake rate of nimodipine in rabbit hepatocytes at 28, 32 and 37℃. Values are the mean ± SD of three experiments: 28℃ (□), 32℃ (▴) and 37℃ (○).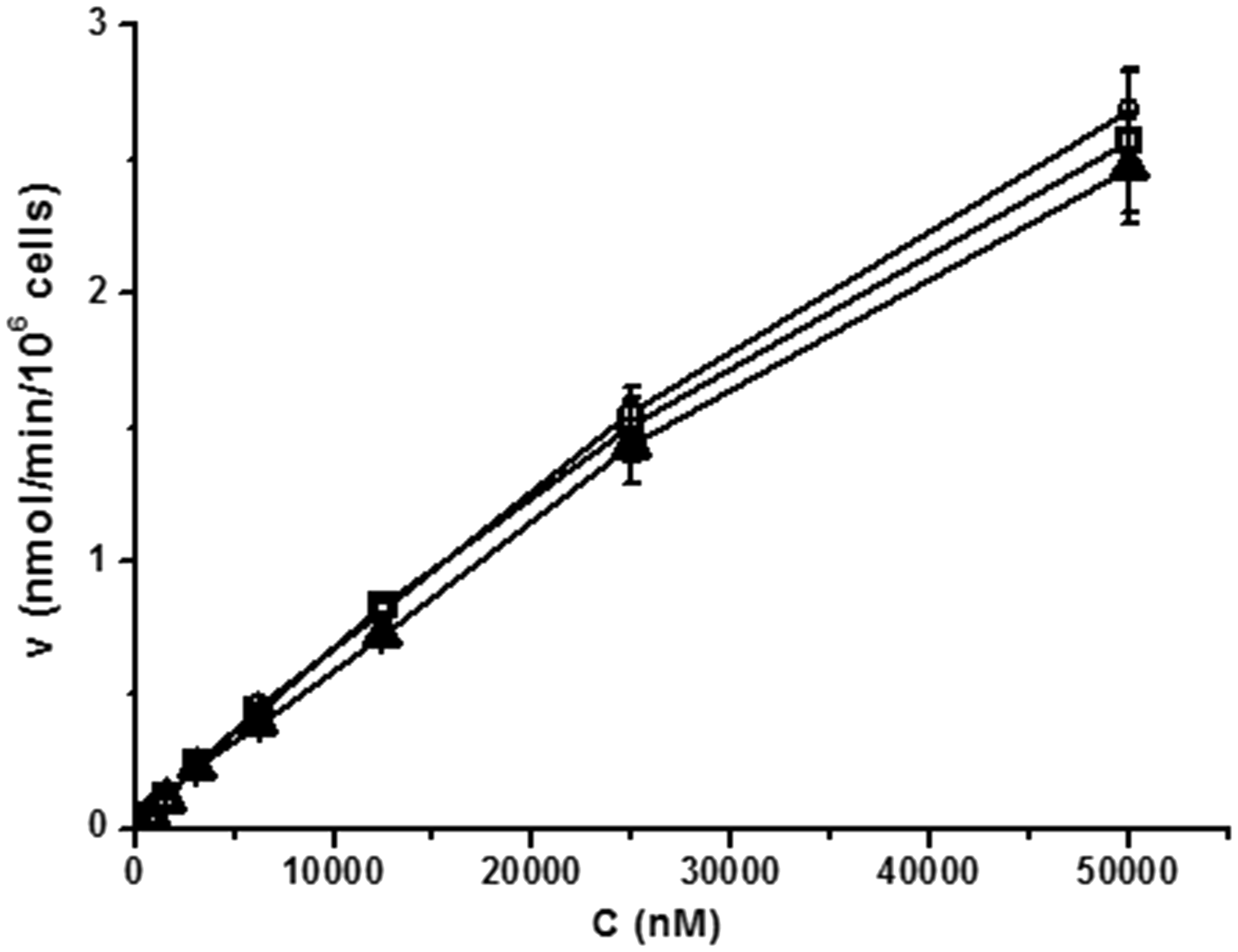
Discussion
Nimodipine is mainly eliminated by the liver. After administration, it is widely distributed throughout the body and undergoes extensive hepatic metabolism. Most of the metabolic steps involve phase 1 reactions catalyzed by CYP enzymes, mainly CYP3A4. 18 Orally administered nimodipine is subject to extensive first-pass metabolism from the portal circulation, resulting in low systemic bioavailability. 13 Therefore, in the present study, the intravenous route was selected to exclude the bioavailability factor.
Clearance is the most useful parameter for evaluating the efficiency and mechanism of drug elimination, defined as the hypothetical volume of biological fluids irreversibly cleared of the drug per unit time. The systemic clearance of a drug is the sum of the clearance values from all the organs, mainly the kidney and liver. For nimodipine, only the parent compound is active and the hepatic clearance approximates the systemic clearance, 19 therefore hepatic clearance, which is the focus of the present study, may play the most important role in plasma exposure and response. According to the equation CLh = QhċE = Qhċ[FuċCLint invivo/(Qh +FuċCLint invivo)], derived from the classic well-stirred model, 20 factors that affect the hepatic clearance (CLh) of a drug include: 1) blood flow to the liver (Qh), 2) fraction of unbound drug in rabbit plasma (Fu), and 3) in vivo intrinsic hepatic clearance (CLint invivo), which is defined as the clearance in the absence of restriction of blood flow and plasma protein binding. The average hepatic blood flow (Qh) was estimated at 70.8 ml/min/kg. 21 The results of the hepatocyte assay showed the uptake rate of nimodipine in rabbit hepatocytes was high, increased linearly with concentration, and remained unchanged by temperature, indicating that uptake clearance was not a limited process of hepatic elimination and no active uptake was involved. The extrapolated CLint invivo obtained from our studies was therefore applied to the function. The results of the calculated hepatic clearance values for nimodipine in rabbits were 2.31 ± 0.01, 1.85 ± 0.04 and 1.09 ± 0.19 L/h at 37℃, 32℃ and 28℃ respectively. Compared with in vivo observed systemic clearance values (2.34 ± 0.24 L/h at 38℃; 0.58 ± 0.11 L/h at 31℃), the calculated hepatic clearance values were comparable during normothermia, but overestimated during hypothermia. The reason for this overestimation might have been due to reductions in hepatic blood flow during hypothermia being ignored in the course of calculating.
The results from the animal studies showed that systemic clearance of nimodipine during hypothermia was reduced by 75.2% compared with normothermia. According to the function CLs = Ke × Vd, changes in systemic clearance (CLs) are contributed to equally by the reduction in the volume of distribution (Vd) and the elimination rate constant (Ke), resulting in higher plasma concentration and t1/2. The lower Vd during hypothermia might have resulted from reduced systemic blood flow, including in the brain. However, nimodipine significantly improved cerebral blood flow at low temperatures, consistent with previous reports. 22 We also found that the magnitude of the improvement of cerebral blood flow was not significant in either period with administration of the same dose of nimodipine, although the system exposure was significantly higher in hypothermia than that in normothermia. This phenomenon might have arisen from the saturation of the drug effect with higher exposure or the reduced activity of the nimodipine receptor during hypothermia.
The time it took TAMX and RI to return to baseline levels in rabbits with hypothermia was significantly longer than that under normothermia (TAMX: 4 h vs. 1 h; RI: 6 h vs. 2 h respectively). As the parent compound alone was active, the prolonged effective duration of nimodipine could be attributed to the lower rate of elimination in hypothermia.
In summary, it is possible that hypothermia can decrease hepatic CLint for nimodipine, contributing to a reduction in systemic clearance. As a result, a routine dose of nimodipine results in an elevated system exposure with little enhancement in pharmacological effect. The higher risk of adverse reactions with greater exposure makes it necessary to optimize pharmacotherapeutic regimens when nimodipine is clinically used during therapeutic hypothermia; this can be achieved by decreasing the routine dose by 25%. Follow-up studies that focus on hepatic blood flow and the exposure–response relationship of nimodipine at different body temperatures are needed to fully elucidate the mechanism underlying the changes in pharmacokinetics and pharmacodynamics.
Footnotes
Abbreviation list
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This work was supported by the National Natural Science Foundation of China (grant No. 81273598 and 81373472).