
Abstract
Objective
A randomized controlled trial to evaluate the use of fat emulsion and normal saline for bile leakage tests during hepatic resection.
Methods
Patients were randomized to undergo intraoperative bile leakage tests with saline then fat emulsion (Group A), or fat emulsion then saline (Group B). All patients received both tests.
Results
In group A (n = 64), saline revealed 53 leakage points in 27 patients, and fat emulsion revealed 42 additional points in a further nine patients. In group B (n = 64), fat emulsion revealed 87 leakage points in 37 patients, and saline revealed three additional points in three patients. There were no significant between-group differences in the number of leakage points detected by the first test, total number of leakage points or postoperative complications. Significantly more leakage points were detected by the second test in Group A (fat emulsion) than in Group B (saline).
Conclusions
Fat emulsion then saline identifies more leakage points after the first test than saline then fat emulsion. There is no difference in the total number of leakage points detected, regardless of which method is used first.
Introduction
Bile leakage is a common complication of hepatectomy, occurring in 3–33% of patients.1–7 Bile leakage is difficult to avoid, increases postoperative hospital stay and seriously affects health-related quality-of-life.1,2,8–11 In addition, the presence of bile within the surgical cavity increases the risk of bacterial infection, impairs the immune response, and may cause sepsis and liver failure. 7 The timely detection and repair of intraoperative bile leakage is extremely important, but small leakage points are often difficult to detect. 7
There are several methods for detecting and/or preventing bile leakage after hepatectomy, including bile leakage tests,1,8,12–15 which detect open bile duct stumps on the resection surface by increasing fluid pressure within the duct.1,8,12 The fluid used can be saline, which is low cost, nontoxic, has low viscosity (allowing the detection of small leakage points) and can be repeated as many times as needed. Saline is difficult to detect, however, because it is colourless,13–15 and its use may not lower the incidence of postoperative bile leakage. 13 This can be overcome by the use of a fluorescent dye, but this requires special equipment and there is a risk of allergic reaction.15,16 An alternative is methylene blue, but the dye stains the entire resection surface (preventing the repetition of the procedure), and there is also a risk of allergic reaction. 17
Bile leakage tests using fat emulsion allow for the direct and easy visualization of white droplets appearing on the resection surface.7,14,18,19 The incidence of postoperative bile leakage is significantly lower when using fat emulsion compared with saline, 18 or in control patients. 7 The fat emulsion is harmless to tissue, 20 but there are little data regarding the efficacy of this procedure. Studies performed to date have randomized patients to either saline or fat emulsion groups, but it is unknown if the use of both methods could increase the detection rate, and whether the order in which they are used is important.
The present study randomized patients to receive either fat emulsion then saline, or saline then fat emulsion bile leakage tests, to compare the efficacy and sensitivity of both methods in revealing intraoperative bile leakage points, and to assess whether the order of use had an impact on the number of leakage points detected. Our working hypothesis was that using fat emulsion first would reveal more leakage points than using saline first.
Patients and methods
Study population
This randomized, parallel, controlled trial recruited patients who underwent liver resection for any liver disease (benign or malignant tumour, liver metastases or intrahepatic bile duct stones) at the Fourth Hospital of JiLi University, ChangChun, China, between January 2005 and December 2011. Exclusion criteria were: (i) patient required duct rebuilding; (ii) history of abdominal surgery; (iii) resection of other organs in addition to liver; (iv) previous cholecystectomy; (v) emergency surgery. The study was approved by the ethics committee of the Fourth Hospital of JiLi University, ChangChun, China, and all patients provided written informed consent prior to enrolment.
Study design
Patients were randomized to group A (bile leakage test using saline first, then fat emulsion) or group B (bile leakage test using fat emulsion first, then saline) in a 1 : 1 ratio using a random-number table generated by SPSS® version 12.0 (SPSS Inc., Chicago, IL, USA) and sequential sealed envelopes. A statistician prepared the sealed envelopes, and the surgeon opened an envelope on the day of the surgery. Only the nurses in the recovery ward were blinded to intervention. All patients underwent both procedures, ensuring that all patients received optimal care. There were no changes to methods after trial commencement.
Outcomes
The primary outcome was the total number of bile leakage points on the transected liver surface. The secondary outcome was postoperative complications of liver resection. There were no changes to trial outcomes after trial commencement.
Bile leakage test
The same methods and instruments were used for resection in both groups.After liver resection, bleeding on the transected liver surface was stopped and visible bile leakage points were completely sutured. A 1-cm length of cystic duct was retained after cholecystectomy. Saline or 10% fat emulsion (Sino-Swed Pharmaceutical Corp. Ltd., Jiangsu, China) was injected (20–30 ml, at a pressure of 25–30 cmH2O) into the cystic duct and the common bile duct was pressed and blocked. When the common bile duct was filled, the bile duct was released and two physicians evaluated fluid leakage on the transected liver surface. In the case of leakage, the number of leakage points was recorded and the points were marked. A small amount of fluid was injected to check for new leakage points. If new leakage points appeared, fluid injection was repeated. The total number of leakage points was recorded until no new leakage points were found.
The remaining fluid in the common bile duct was extracted and fat emulsion or saline (20–30 ml) was injected into the cystic duct. The same procedure as before was followed for the second test.
All leakage points were sutured in a figure-of-eight shape, using 3–0 or 0–0 absorbable sutures. After rinsing the transected surface with saline, a small amount of fat emulsion was then injected to detect whether there were new leakage points. Rinsing and injection were repeated until no leakage was observed.
After the test, saline was injected at low pressure into the cystic duct to rinse the fat emulsion from the biliary tract. Finally, the transected liver surface was sealed with fibrin glue and two silicone drainage tubes were placed in the abdomen. Diagnostic criteria for postoperative bile leakage were: (i) bile in abdominal drainage or postoperative abdominocentesis; (ii) postoperative cholangiography revealed bile leakage; (iii) intraperitoneal bile found in repeat surgery.7,21
Statistical analyses
Sample size was calculated with an expected difference of 2.0 between the mean number of bile leakage points detected by group A and group B, with an estimated SD of 3.0. Using a significance level of 0.05 (two-sided), a power of 0.95 and β = 0.05, ≥ 48 patients were required in each group. SPSS® version 12.0 (SPSS Inc.) was used for data processing and analysis. Categorical data were expressed as proportion or rate, and analysed using χ2-test or Fisher’s exact test, as appropriate. Continuous variables were expressed as mean ± SD, and analysed using Student’s t-test. P-values < 0.05 were considered statistically significant.
Results
The study included 128 patients (75 male/53 female; mean age 53.0 ± 1.2 years; age range 32–78 years). A flowchart of patient recruitment and randomization is shown in Figure 1. Demographic and clinical characteristics of the patient group are shown in Table 1. Intraoperative blood loss was significantly smaller in group B than group A (P < 0.05). There were no significant between-group differences in any other demographic or clinical characteristics.
Flowchart of patient recruitment and randomization in a controlled trial to evaluate the use of fat emulsion and normal saline for bile leakage tests during hepatic resection. Demographic and clinical characteristics of patients undergoing liver resection included in a study evaluating the efficacy of bile leakage tests using saline then fat emulsion (Group A) or fat emulsion then saline (Group B). Data presented as n (%) or mean ± SD. Defined as <35 g/l. P < 0.05; Student’s t-test.

Intraoperative bile leakage points detected in patients undergoing liver resection with bile leakage tests using saline then fat emulsion (Group A) or fat emulsion then saline (Group B).
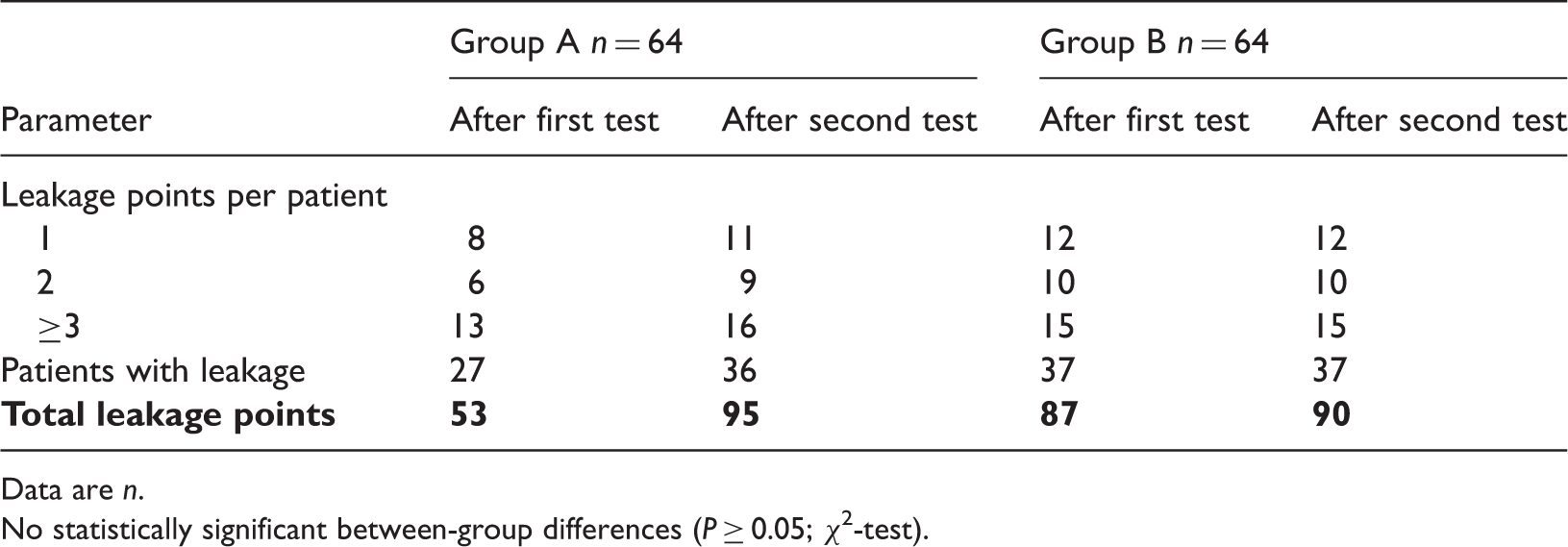
Data are n.
No statistically significant between-group differences (P ≥ 0.05; χ2-test).
Postoperative complications in patients undergoing liver resection with bile leakage tests using saline then fat emulsion (Group A) or fat emulsion then saline (Group B).

Data are n.
No statistically significant between-group differences (P ≥ 0.05; χ2-test).
Discussion
Our findings indicate that bile leakage tests performed with fat emulsion and then saline identify more leakage points after the first test than those performed with saline then fat emulsion. However, this difference was not statistically significant and there was no significant difference in the total number of leakage points detected. While fat emulsion is more effective for detection of bile leakage points when used before saline, the order in which these methods is implemented is unimportant.
Fat emulsion and saline each have their advantages. The white colour of the fat emulsion allows for easier detection, but saline can identify smaller leaker points due to its low viscosity.13–15 Fat emulsion has been successfully used to identify bile leakage points,14,18 and can decrease the incidence of postoperative bile leakage. 7 Despite the use of two detection methods, there were some cases of postoperative bile leakage in the present study (n = 7, 5.4%), although this is within the range reported by others (3.7–6.7%).7,14,18,19
The use of fat emulsion in bile leakage tests does not require special equipment, contaminate the wound, cause allergic reaction or damage the bile duct and surrounding tissues. It can easily be repeated the number of times necessary to detect and close all leakage points, can pinpoint even small leaks and is inexpensive. This technique is easier to perform than fluorescent imaging, and is more sensitive and reliable compared with saline bile leakage test used alone.18,19
The present study has some limitations. The number of patients included (although larger than in many other studies of this type) was too low to allow our conclusions to inform clinical practice. In addition, using a combination of both techniques allowed us to ensure that almost all bile leakage points were found, resulting in the best outcomes for the patient but preventing any comparison of postoperative differences between the two methods. Finally, the present study was powered to be a superiority study, rather than a noninferiority study. Future studies should be designed to take this into consideration and to include greater numbers of patients.
In conclusion, intraoperative bile leakage tests performed with fat emulsion and then saline identify more leakage points after the first test than those performed with saline then fat emulsion, although this difference was not statistically significant. There is no difference in the total number of leakage points detected, regardless of which method is used first. Further large-scale studies are necessary to confirm our results.
Footnotes
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.