
Abstract
Objective
To test the hypothesis that double bundle posterior cruciate ligament (PCL) reconstruction yields better improvement in stability and functional recovery of the knee than the single bundle technique.
Methods
PubMed®, Embase®, the Cochrane Library, CNKI, Wanfang and CBM disc databases were searched for comparative trials of PCL reconstruction using the single- versus double bundle technique. Data were extracted and meta-analysis was performed for stability improvement and functional recovery.
Results
The meta-analysis included 435 patients in three randomized controlled trials (RCTs) and eight non-RCTs. Double bundle reconstruction provided significantly better 90° posterior stability than the single bundle technique (weighted mean difference 0.81, 95% confidence interval, [CI] 0.2, 1.42). Double bundle reconstruction resulted in a significantly higher likelihood of International Knee Documentation Committee (IKDC) examination grade A than the single bundle technique (odds ratio 0.41, 95% CI 0.24, 0.72).
Conclusions
The small amount of data available indicates that double bundle reconstruction is superior to the single bundle technique after isolated PCL injury. These findings should be interpreted with caution due to the low quality and limited sample size of the studies concerned.
Introduction
The posterior cruciate ligament (PCL) is twice as strong as the anterior cruciate ligament (ACL) and is one of the most important stabilizers of the knee. 1 Around 44% of knee injuries involve damage to the PCL. 2 Both the ACL and PCL comprise two bundles.1,3 Single bundle PCL reconstruction cannot always effectively replicate normal knee joint motion, 4 whereas double bundle reconstruction restores the normal PCL anatomy and may offer improved clinical and biomechanical outcomes.4–7 It has been suggested that double bundle PCL reconstruction is surgically more complex than the single bundle technique and may not be sufficiently clinically superior to render it worthwhile.7–9
A number of evidence-based systematic reviews have attempted to determine the optimal technique for PCL reconstruction, but their findings are inconclusive.10–14 The aim of the present evidence-based systematic review was to perform a meta-analysis to compare clinical and functional outcomes of PCL reconstruction using single- and double bundle techniques. Our hypothesis was that double bundle PCL reconstruction provides better restoration of normal knee motion than the single bundle technique, with consequent improvements in clinical outcome measurements.
Materials and methods
Search strategy
In accordance with guidelines from the Cochrane handbook, 15 searches of PubMed®, Embase®, the Cochrane Library, CNKI, Wanfang and CBM disc databases were performed for all peer-reviewed studies published up to April 2014 that compared double bundle with single bundle PCL reconstruction. There were no restrictions on publication language. Search terms were: “reconstructive surgical procedure”; “operation”; “surgery”; “posterior cruciate ligament”; “single bundle”; “one bundle”; “one tunnel”; “one band”; “one socket”; “double bundle”; “two bundles”; “two tunnels”; “two bands”; “two sockets”; “bi band”; “bi socket”; “bi bundle”; “bi tunnel”.
Study criteria
Studies were considered eligible for inclusion if they met the following criteria: (i) comparative studies (randomised controlled trials [RCTs] or non-RCTs); (ii) patients with PCL tear with or without other knee injuries; (iii) comparison of arthroscopic single bundle and double bundle PCL reconstruction; (iv) outcomes at ≥12-month follow-up – knee 90° posterior stability, knee 30° posterior stability, range of knee motion (ROM) and clinical functional outcomes. The main endpoints for the meta-analysis were knee posterior stability and subjective outcome (Lysholm knee function score 16 or Tegner activity scale 17 ) and the International Knee Documentation Committee (IKDC) grade examination. 18
Exclusion criteria were: open or repeat PCL reconstructive surgery; ligament or other injuries in the contralateral knee; studies with “time zero” (e.g., intrasurgical) outcome measures; technique articles; comparisons within single- or double bundle techniques; review articles.
Study selection
Article titles and abstracts were independently screened by two reviewers (X.Y.S. and Z.Z.). Subsequently, the full text of the studies that potentially met the inclusion criteria were read and reviewed to determine their suitability for inclusion or exclusion in the present analysis.
Data extraction
Data were extracted independently by two reviewers (J.X.Z. and Z.M.). Data included title, authors, year of publication, study design, sample size, population, age, sex, type of graft, fixation method, accompanying injuries, surgical procedures, duration of follow-up and outcome parameters.
Assessment of methodological quality
Methodological quality of RCTs and non-RCTs was appraised using the Cochrane collaboration tool for assessing the risk of bias 15 and Methodological Index for Non-Randomized Studies (MINORS) form, respectively. 19
Statistical analyses
Continuous data were expressed as weighted mean difference (WMD) with 95% confidence interval (CI). Dichotomous data were presented as odds ratio (OR) with 95% CI. Statistical analyses for continuous and dichotomous data were performed by independent sample Student-t test and Chi-square test, respectively, using Review Manager software, version 5.2 (The Nordic Cochrane Centre, The Cochrane Collaboration, Copenhagen, Denmark). P-values < 0.05 were considered statistically significant. Heterogeneity was assessed with the I2 statistic, where I2 > 50% was considered substantial heterogeneity. In the case of substantial heterogeneity, data were pooled using a random-effects model. A fixed-effects model was used in the absence of heterogeneity.
Sensitivity analyses were performed to explore the influence of preoperative conditions, tools for outcome assessment and other techniques that varied between studies.
Results
A total of 157 titles and abstracts were preliminarily reviewed,9,20–29 of which 11 studies satisfied the eligibility criteria. These studies included 3 RCTs20–22 and eight retrospective cohort studies,9,23–29 with a total of 435 patients (n = 229 single bundle; n = 206 double bundle). The studies were published between 2004 and 2014. Figure 1 shows the process of literature selection. The characteristics and demographic data of each study are given in Table 1. Follow-up duration ranged from 12–90.5 months.
Selection process for studies included in a meta-analysis of outcomes of posterior cruciate ligament reconstruction using the single- versus double-bundle technique. Demographic and clinical data for studies included in a meta-analysis comparing clinical outcomes of single- and double-bundle posterior cruciate ligament reconstruction. SB, single bundle; DB, double bundle; IKDC; International Knee Documentation Committee grade
18
; NS, not stated; STG, semitendinosus and gracilis graft; ACL, anterior cruciate ligament; MCL, medial collateral ligament; LCL, lateral collateral ligament; BPTB, bone–patellar tendon–bone graft. Kim
24
included 29 patients (n = 8 transtibial SB, n = 11 SB with tibial inlay, n = 10 DB with tibial inlay), (a) transtibial SB versus DB with tibial inlay; (b) SB with tibial inlay versus DB with tibial inlay.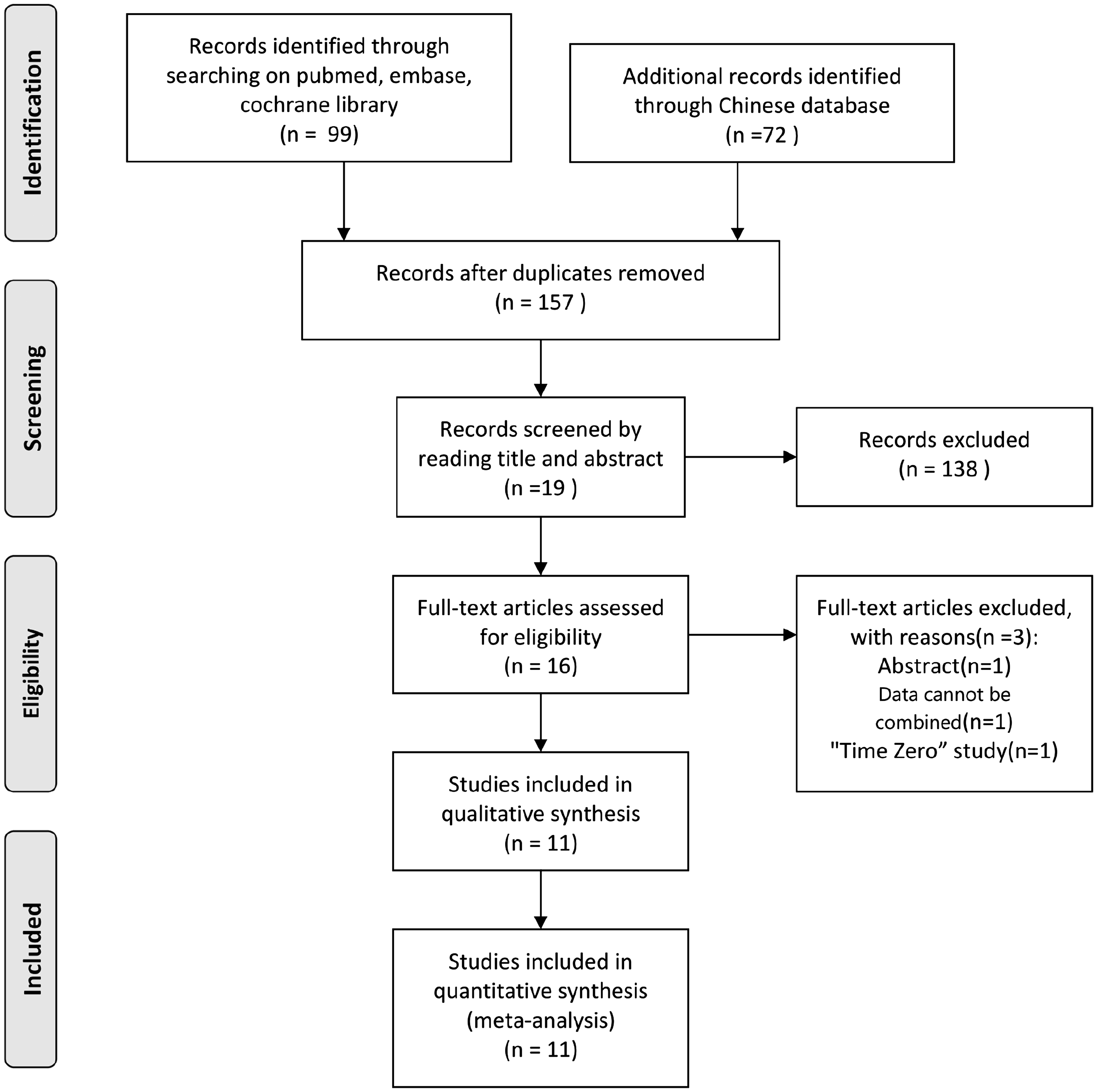

All RCTs were single-centre studies. Of these, two21,22 were judged as having moderate risk of selection bias (no details of random sequence generation;21,22 no details of blinding method for participants, personnel or outcome assessors 21 ). A further study was judged to have a high risk of performance bias and detection bias (all procedures and outcome assessments were performed by the same author). 20 In two studies, over 5% of patients were lost to follow-up.20,22 A single study reported adequately generated allocation concealment. 22
MINORS 16 appraisal scores for non-randomized controlled trials included in a meta-analysis comparing clinical outcomes of single- and double-bundle posterior cruciate ligament reconstruction.

MINORS criteria include the following items: (1) a clearly stated aim; (2) inclusion of consecutive patients; (3) prospective data collection; (4) endpoints appropriate to the aim of the study; (5) unbiased assessment of the study endpoint; (6) a follow-up period appropriate to the aims of the study; (7) <5% loss to follow-up; (8) prospective calculation of the sample size; (9) an adequate control group; (10) contemporary groups; (11) baseline equivalence of groups; (12) adequate statistical analyses. Items are scored as follows: 0 (not reported); 1 (reported but inadequate); or 2 (reported and adequate). The ideal global score for comparative studies is 24.
Ten studies (n = 431) reported knee posterior stability at 90° flexion.9,20–28 Double bundle reconstruction provided significantly more posterior stability than the single bundle technique (WMD 0.81; 95% CI 0.20, 1.42 Figure 2), but heterogeneity was high (I2 74%). There was no significant between-group difference in posterior stability when RCTs alone were analysed (n = 134).20–22 Sensitivity analyses Table 3 indicated that the double bundle technique was significantly superior in patients with PCL isolated injuries (n = 244; P = 0.001 for all studies; P < 0.001 for RCTs; Table 3).9,20,22–24,29 There were no significant between-group differences in knee stability at 30° (n = 138)9,21,26,27 or ROM (Table 4) (n = 88).20,21
Sensitivity analyses using various exclusion criteria for 90° posterior stability of the knee after single- or double-bundle posterior cruciate ligament (PCL) reconstruction. SB, single bundle; DB, double bundle; WMD (95% CI), weighted mean difference (95% confidence intervals); RCT, randomized controlled trial; ACL, anterior cruciate ligament. Independent-samples Student’s t-test. Results of meta-analysis for clinical outcome of single- or double-bundle posterior cruciate ligament (PCL) reconstruction. SB, single bundle; DB, double bundle; WMD (95% CI), weighted mean difference (95% confidence intervals); NS, not statistically significant (P ≥ 0.05); IKDC, International Knee Documentation Committee grade.
18
Independent-samples Student’s t-test for knee stability and range of motion; Chi-square test for IKDC grade.

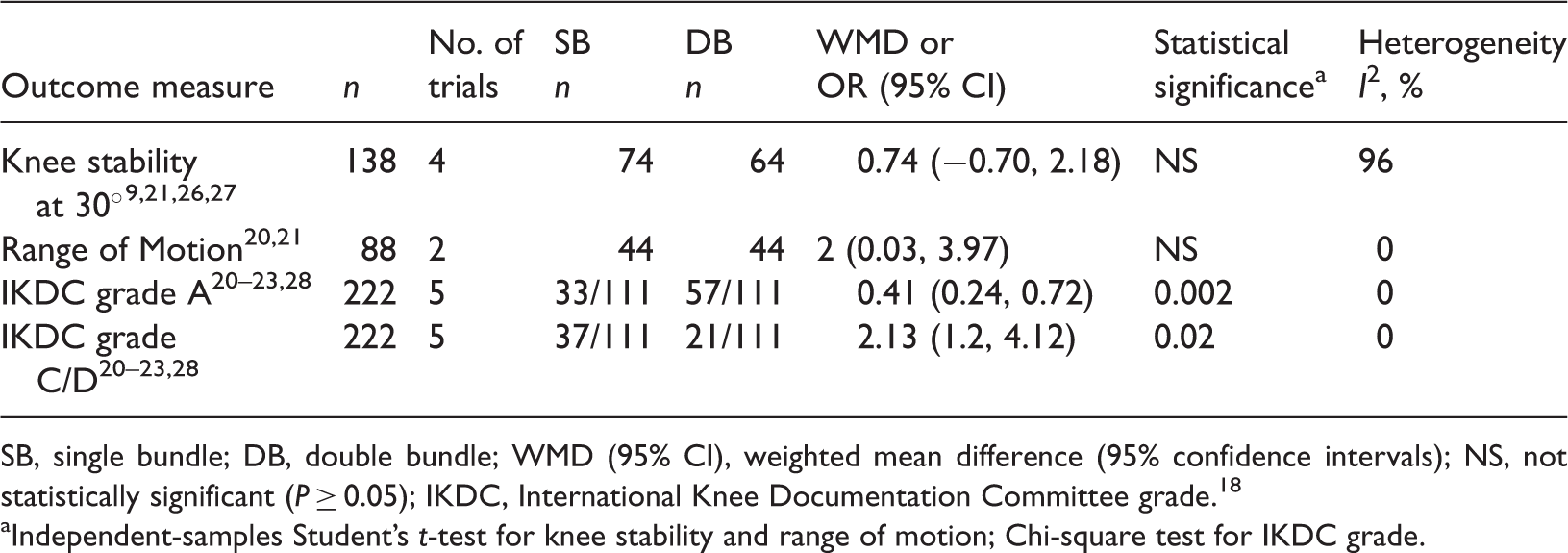
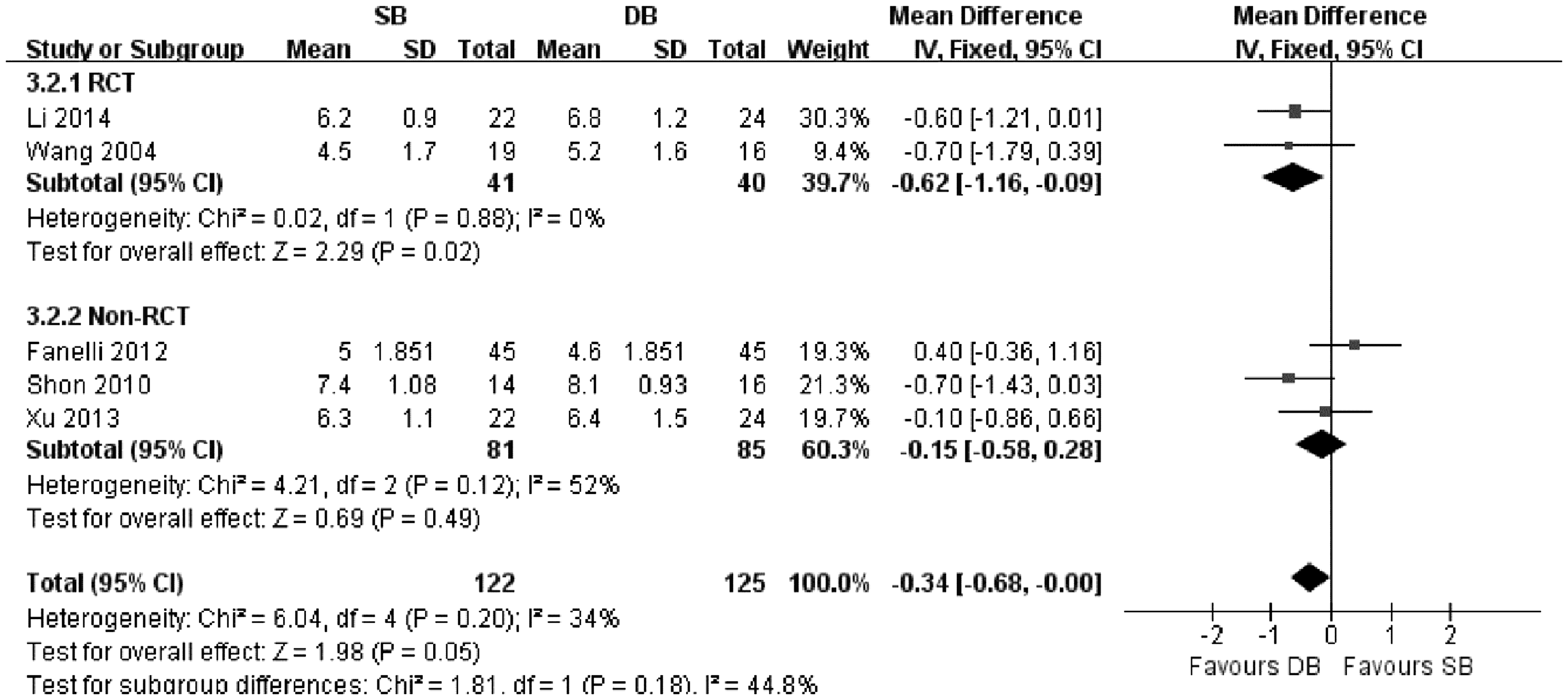
Studies using the Lysholm test found no significant between-group difference in outcome (n = 372; Figure 3).9,21–24,26–29 Those reporting the Tegner activity scale indicated significantly better outcomes after double- rather than single bundle reconstruction (n = 247; OR −0.34, 95% CI −0.68, 0.00; Figure 4).9,21–23,26 The IKDC examination was reported in five studies (n = 222)20–23,28 with outcomes categorized as grade A or grades C/D (Table 4). There were significantly more patients with grade A outcomes in the double bundle group than in the single bundle group (P = 0.002).

Discussion
The optimal technique for PCL reconstruction remains unclear. The present meta-analysis comparing single- and double bundle techniques found that double bundle reconstruction resulted in superior 90° posterior knee stability in patients with PCL isolated injuries. In addition, IKDC grade and Tegner activity scale scores were both better following double bundle than single bundle reconstruction. There was high heterogeneity between the included studies, mainly due to study design and preoperative conditions.
The main source of bias in the current meta-analysis was blinding performance in both RCTs and non-RCTs. additional sources of bias included preoperative conditions, outcome examination tools and other technique details. Retrospective studies were subject to reporting bias. The majority of studies included in the present analysis had high methodological assessment risks, which could have influenced the pooled results.
The objective physical parameter of 90° posterior knee stability was chosen as the primary outcome measure in our meta-analysis. Double bundle reconstruction was significantly superior to the single bundle technique, although heterogeneity was high. Since there was a lack of uniformity regarding injury type as well as assessment tool used, we used sensitivity analyses to determine the influence of these factors on the pooled results. Due to the limited data available, it was not possible to determine which measurement tool was more accurate and reliable. Future studies are required to test and verify the accuracy and sensitivity of different examination tools, and allow the standardization of the method used to assess knee stability.
Biomechanical studies have indicated that single bundle reconstruction did not prevent posterior laxity at a flexion angle <30°, and the double bundle technique resulted in significantly less internal rotational laxity at flexion angles >90°. 30 The present analysis included four studies that assessed posterior laxity at 30° flexion.9,21,26,27 Heterogeneity was high among these studies (I2 98%), but sensitivity analyses were unable to identify the source of bias. Evaluation of knee rotational instability was not performed in all studies in the present analysis, and would be a useful primary endpoint in future studies in order to elucidate the reasons for the biomechanical superiority of the double bundle technique.
Functional clinical outcomes, determined via the objective IKDC grade and subjective Tegner activity scale, were significantly better after double bundle than single bundle reconstruction, but there was no significant between-group difference in Lysholm score. This may be due to the limited sample size of the present analysis.
The present meta-analysis has several limitations. First, it included only three RCTs, and these were of low quality. In addition, knee posterior stability was assessed using three different tools, and rotational instability was not evaluated in all studies. Finally, complication rates (including repeat surgery, revision or graft rupture rate) were not reported. Further clinical studies are needed to analyse these points.
In conclusion, the small amount of data available indicates that double bundle reconstruction is superior to the single bundle technique after isolated PCL injury. These findings should be interpreted with caution, however, due to the low quality and limited sample size of the studies concerned. Further high quality clinical studies are required to assess the relative merit of double- and single bundle PCL reconstruction.
Footnotes
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.