
Abstract
Objective
To determine the relationships between serum leptin and levels of lipoprotein(a) [Lp(a)], apolipoprotein A-1 (ApoA-1) and apolipoprotein B (ApoB) in patients with cholelithiasis.
Methods
Patients with ultrasound-confirmed cholelithiasis and controls frequency-matched for age, sex, body mass index, fasting blood glucose and haemoglobin A1c levels were recruited. Fasting blood samples from all study participants were assayed for glucose, haemoglobin A1c, total cholesterol, high density lipoprotein-cholesterol (HDL-C) and triglyceride. Serum Lp(a), ApoA-1 and ApoB levels were measured using nephelometric assays; serum leptin was measured using an enzyme-linked immunosorbent assay.
Results
A total of 90 patients with cholelithiasis and 50 controls were included in the study. Serum levels of leptin, Lp(a), total cholesterol, triglyceride and ApoB were significantly increased, and levels of ApoA-1 and HDL-C were significantly decreased, in patients with cholelithiasis compared with controls. Serum leptin in patients with cholelithiasis were significantly positively correlated with Lp(a) and ApoB and negatively correlated with ApoA-1.
Conclusions
Patients with cholelithiasis have higher leptin levels and an altered lipoprotein profile compared with controls, with increased leptin levels being associated with increased Lp(a) and ApoB levels, and decreased ApoA-1 levels, in those with cholelithiasis.
Introduction
Gallstone-related disease is an important and costly healthcare problem in Western societies. 1 Gallstones are common, with a prevalence as high as 10–15% in Europe and 3–11% in Asia.2,3 Cholesterol gallstone formation is a complex process that is mediated by genetic and environmental factors. Cholesterol gallstones are induced by an imbalance of cholesterol metabolism that involves changes in intestinal absorption, hepatic biosynthesis and biliary output of cholesterol and its conversion to bile acids.2,4 Gallstone risk factors include female sex, obesity, ageing, diabetes mellitus, hypertriglyceridaemia, insulin resistance, oestrogen therapy and ethnicity.2–4 The three major factors in the pathogenesis of cholelithiasis are gallbladder dysmotility, cholesterol supersaturation of the bile and cholesterol nucleation.2,3 Multiple associations between gallstones and dyslipidaemia,4–6 coronary artery disease 7 and stroke 8 have been reported. Gallbladder disease has been shown to be associated with heightened fasting serum insulin levels in women.9,10 Hyperinsulinaemia increases hepatic cholesterol excretion and biliary cholesterol supersaturation, and induces gallbladder dysmotility; insulin resistance has been shown to be associated with cholelithiasis in nondiabetic, nonobese individuals. 11
Leptin, a 16 kDa nonglycosylated polypeptide product of the ob gene, is an adipose tissue-derived hormone and is considered to be one of the major regulators of food intake and energy metabolism. 12 It is secreted from the gastrointestinal tract, with the epithelium of the stomach being a major source of leptin production. 13 Leptin is stable in the stomach despite the acidic pH; from there it passes on into the intestine. Leptin receptors have been identified from the duodenum to the colon in the basolateral membrane of enterocytes and colonocytes, suggesting a role for leptin in the gastrointestinal tract. 14 Leptin receptors have also been identified in the enteric nervous system. 15 Leptin has been shown to modulate nutrient absorption, growth, inflammation and gut motility. 16 Abnormal leptin levels and hyperinsulinaemia are important risk factors for gallbladder disease.17,18 High plasma triglyceride (TG) concentrations and low plasma high-density lipoprotein-cholesterol (HDL-C) concentrations have been associated with a greater risk of gallstone disease. 4 Cholesterol saturation of the bile is heightened when the serum TG concentration is high, whereas the serum concentration of HDL-C is inversely correlated with gallstone prevalence and cholesterol saturation of bile.4,19 The present study aimed to determine the relationships between serum leptin and levels of the lipoproteins lipoprotein(a), apolipoprotein A-1 and apolipoprotein B in patients with cholelithiasis.
Patients and methods
Patients
Patients with gallstones attending the Department of General Surgery and the Department of Clinical Biochemistry, Faculty of Medicine, Dicle University, Diyarbakir, Turkey, between November 2008 and December 2010, were recruited to the study. Patients with acute cholecystitis, biliary colic, acute infection of the biliary tract, haemolytic disease, acute pancreatitis, viral or alcoholic hepatitis, drug-induced liver disease, endocrine, renal, lung or coronary heart disease and those following restrictive diets were excluded from the study. Patients who had previously undergone cholecystectomy due to gallstone disease at the same institution were also recruited to the study group. Prolidase levels were measured and planned to be reported elsewhere (not submitted yet).
As increasing age, female sex, obesity and prediabetes are risk factors for gallstones and have a major influence on lipid levels, and obesity is also a determinant of leptin levels, a matching procedure was employed to avoid confounding. Patients with gallstone disease were matched with controls according to age, sex, body mass index (BMI, calculated as body weight in kg divided by height in m), fasting blood glucose and haemoglobin A1c (HbA1c) levels using the frequency matching method.
The study protocol was approved by the Ethics Committee of Dicle University Faculty of Medicine and all study procedures were in accordance with the ethical standards for human experimentation established by the Declaration of Helsinki. All study participants provided written informed consent.
Patient assessment
A medical history was obtained from all study participants and physical examination, biochemical evaluation and upper abdominal ultrasonography were performed. The presence of intraluminal echogenicity with posterior acoustic shadowing was considered to indicate gallstones. All ultrasonographic studies were evaluated by the same radiologist (A.B.).
Biochemical assessment
Blood samples (10 ml) were taken from all study participants at 09.00 h after a 12-h overnight fast and were immediately centrifuged for 10 min at 3000
Serum levels of apolipoprotein A-1 (ApoA-1) and apolipoprotein B (ApoB) were measured by nephelometric assays using antiserum specific for ApoA-1 and ApoB (Dade Behring, Newark, DE, USA), respectively. The serum leptin level was measured using an enzyme-linked immunosorbent assay kit (Leptin ELISA, DRG International, Springfield, NJ, USA); the limit of detection was 0.2 ng/ml. Lipoprotein-a (Lp[a]) was measured using a nephelometric agglutination assay (N Latex Lp[a] Reagent, Dade Behring). The intra- and interassay coefficients of variations were 1.5–3.0% (n = 20) and 1.7–3.2% (n = 10), respectively; the lower detection limit was 30 mg/l.
Statistical analyses
Results were expressed as the mean ± SD. The unpaired Student’s t-test was used to compare the cholelithiasis and control groups. Pearson’s correlation coefficient was used to estimate the linear relationships between the variables studied. A P-value <0.05 was considered to be statistically significant. All statistical analyses were performed using SPSS® software, version 17.0 (SPSS Inc., Chicago, IL, USA).
Results
A total of 140 participants (92 women and 48 men) were included in the study. Of these, 50 were healthy controls (32 women and 18 men; mean age ± SD, 47.2 ± 8.23 years), and 90 were patients with cholelithiasis (60 women and 30 men; mean age ± SD, 48.1 ± 9.7 years). Because of the matching criteria, there were no statistically significant differences between the groups in terms of age, sex, BMI, fasting blood glucose or HbA1c levels.
Demographic and fasting biochemical parameters in patients with cholelithiasis and healthy controls.
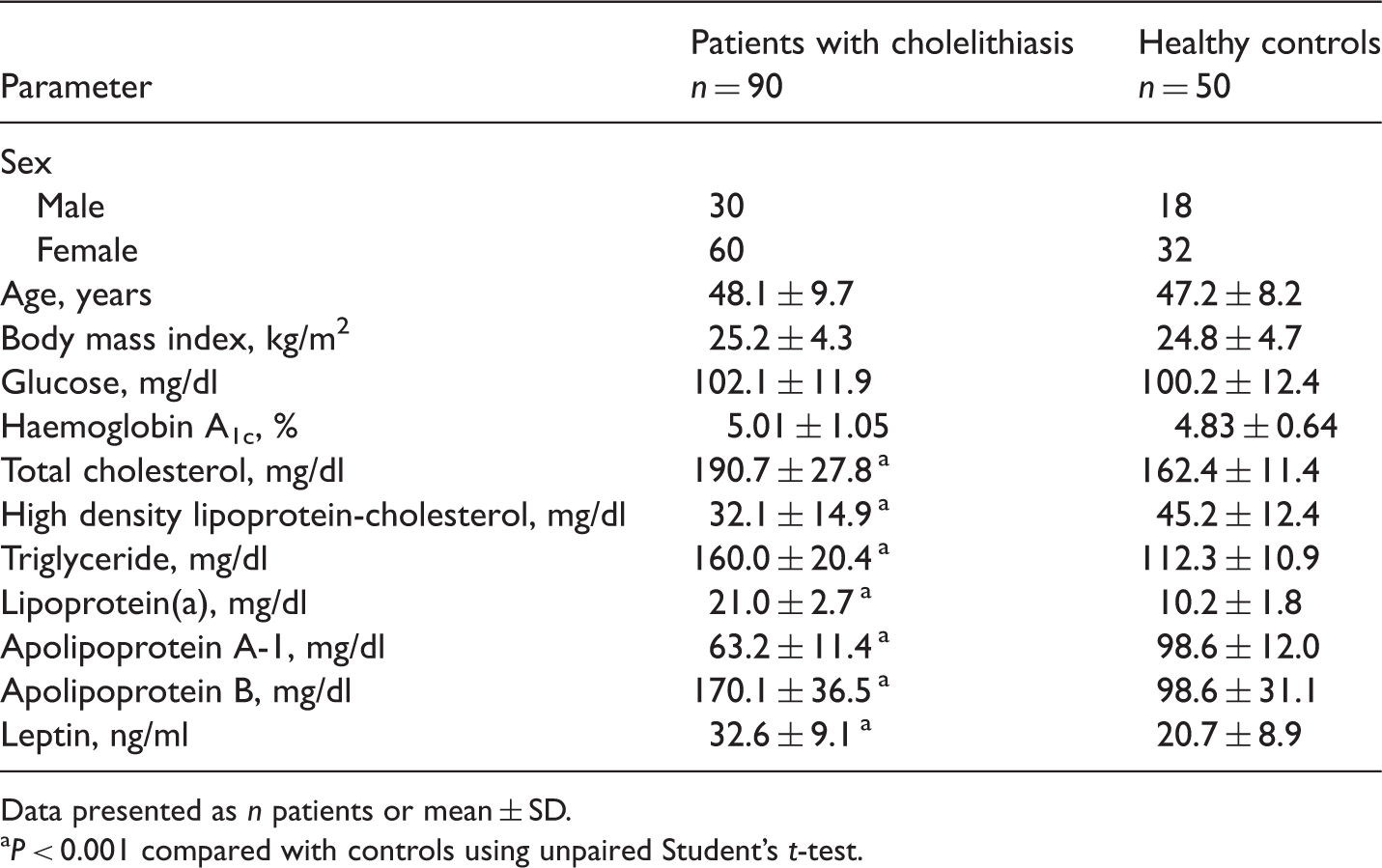
Data presented as n patients or mean ± SD.
P < 0.001 compared with controls using unpaired Student’s t-test.
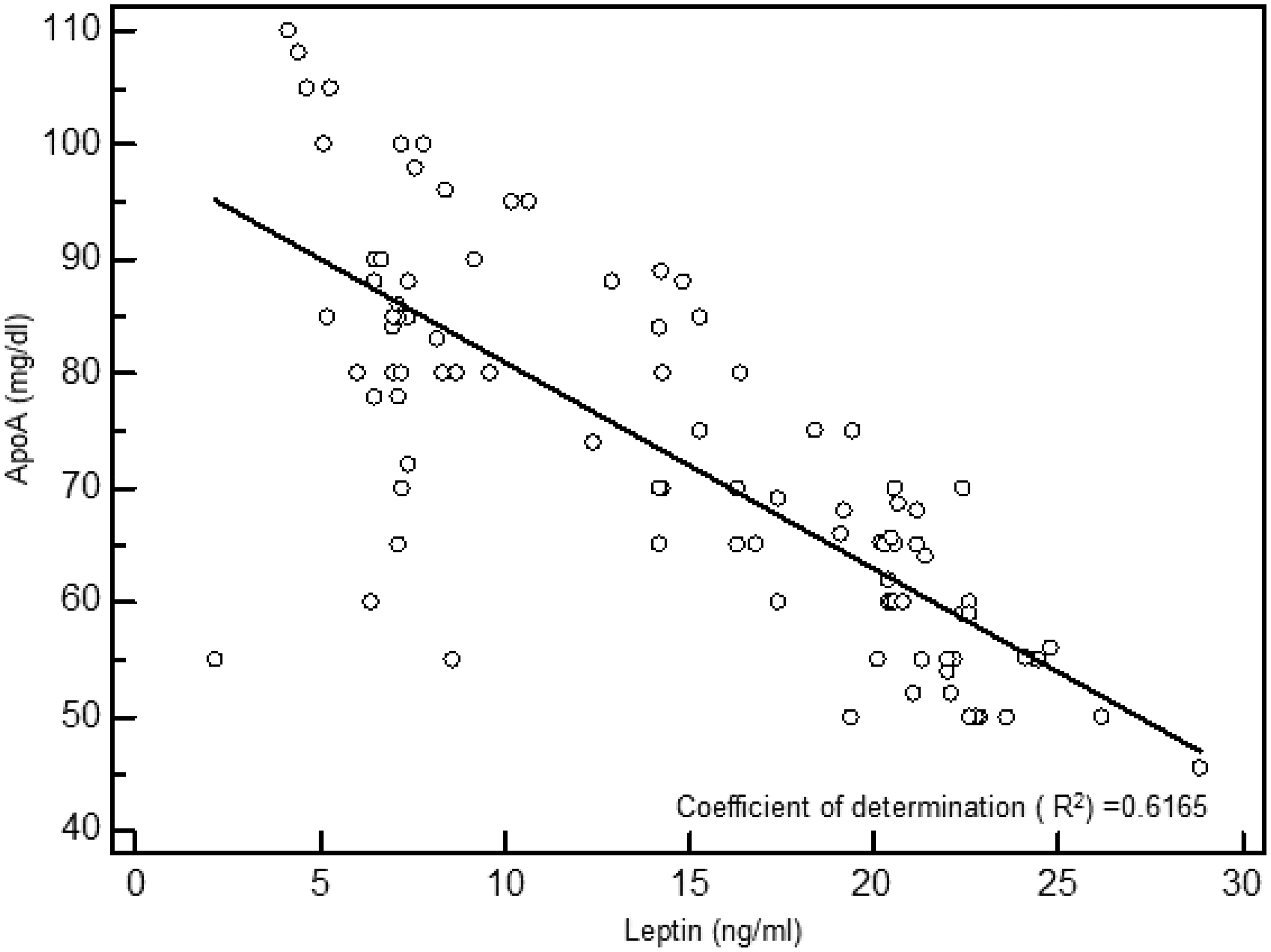
In patients with cholelithiasis, serum leptin levels were positively correlated with serum levels of Lp(a) (r = 0.952, P < 0.001; data not shown) and ApoB (r = 0.918, P < 0.001, Figure 1), and negatively correlated with serum levels of ApoA-1 (r = −0.785, P < 0.001, Figure 2).
Correlation between leptin levels and apolipoprotein B (ApoB) levels in patients with cholelithiasis. Correlation between leptin levels and apolipoprotein A-1 (ApoA) levels in patients with cholelithiasis.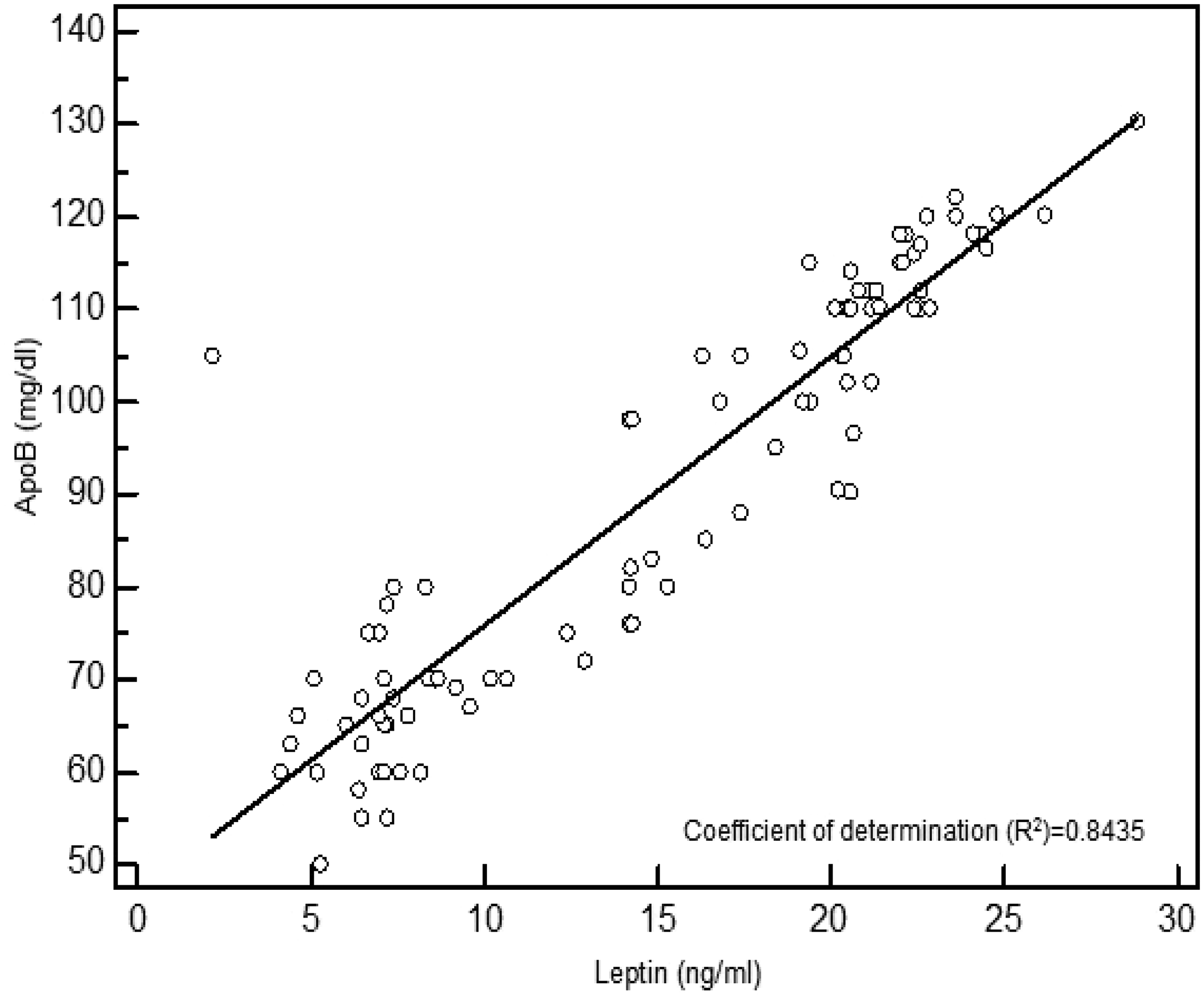
Discussion
Leptin, a hormone produced by adipocytes, is known to have central effects on neuropeptide Y and cholecystokinin, but its influence on the biliary effects of these hormones is unknown. 20 Obese, leptin-deficient mice have large gallbladder volumes with decreased contraction in vitro, and are predisposed to cholesterol crystal formation. 20 Administrating leptin to these mice caused weight loss, restored gallbladder function, upregulated cholecystokinin A receptors, acetylcholine β2 receptors and Ca2+/calmodulin-dependent protein kinase, and downregulated 3-hydroxy 3-methylglutaryl coenzyme A reductase and low-density lipoprotein receptors. 21 A previous study showed that leptin-deficient obese mice had decreased excitatory gallbladder muscle contractile responses to acetylcholine, neuropeptide Y and cholecystokinin. 20 Leptin seems to potentiate the effect of cholecystokinin. Leptin signalling in vagal afferent neurons is required for appropriate cholecystokinin signalling and satiation. 22 De Lartigue and coworkers 23 showed that leptin resistance reduced the sensitivity of vagal afferent neurons to cholecystokinin, thus reducing the satiating effects of cholecystokinin. In addition to regulating vagal afferent nerve discharge, cholecystokinin controls the expression of receptors and peptide neurotransmitters by these neurons; these regulatory actions are potentiated by leptin and inhibited by ghrelin. 24 Florian and coworkers 16 showed that leptin modulated the activity of enteric inhibitory and excitatory neurons in the proximal colon. As leptin seems to have a regulatory function in gastrointestinal motility, the present study evaluated leptin levels in patients with cholelithiasis and found that leptin levels were increased in cholelithiasis compared with controls. There were significant positive correlations between serum leptin and ApoB and Lp(a) and a significant negative correlation between serum leptin and ApoA-1 in patients with cholelithiasis. These findings could be useful in understanding the pathophysiology of cholelithiasis. The results of the present study are consistent with those of previous studies showing elevated leptin levels17,25 and an abnormal lipid profile,5,17,19,26 with higher total cholesterol, TG, ApoB and Lp(a) and lower HDL-C and ApoA-1 levels in patients with cholelithiasis compared with healthy controls. In contrast, some studies have reported no difference in leptin 18 and lipoprotein levels18,25,27,28 in patients with cholelithiasis compared with controls.
Méndez-Sánchez et al. 17 reported that insulin resistance and the development of gallstone disease were associated with serum leptin levels in overweight subjects (BMI < 30 kg/m2), but not in obese subjects (BMI ≥ 30 kg/m2) with similar metabolic profiles. Insulin resistance could have a major role in the pathogenesis of gallstones, favouring the production of cholesterol-supersaturated bile and altering gallbladder function. In another study, Méndez-Sánchez et al. 19 found a negative correlation between leptin and HDL-C levels. Duggirala et al. 29 reported that leptin levels correlated significantly with the incidence of gallstones in a low-income Mexican–American population, especially in women. However, Ruhl and Everhart 30 found that the serum leptin level was not a better predictor of gallstone disease than anthropometry. A significant and positive correlation between leptin levels and biliary cholesterol saturation in obese subjects has been reported.19 Méndez-Sánchez et al. 17 found a strong relationship between gallstone disease and the metabolic syndrome, which has the cardinal feature of hyperinsulinaemia. They also demonstrated the existence of relationships between serum HDL-C, the biliary cholesterol saturation index and serum leptin levels in obese subjects. 19 In the present study, lower HDL-C and ApoA-1 levels but higher Lp(a) and ApoB levels were observed in patients with cholelithiasis compared with controls. Previous studies have suggested that leptin promotes the elimination of serum cholesterol by increasing cholesterol secretion, decreasing cholesterol biosynthesis and increasing conversion of cholesterol to bile salts, whereas obesity and the chronic effect of leptin resistance impair the function of biliary cholesterol secretion.18,19 Graewin et al. 21 reported that leptin modulated obesity and regulated gallbladder genes related to cholesterol gallstone pathogenesis. Tran et al. 31 reported that hyperglycaemia, insulin resistance, hyperlipidaemia and body weight in obese mice with leptin dysfunction were associated with poor gallbladder contractility, which in turn may contribute to the association between obesity and gallstone formation. They also found an inverse correlation between gallbladder contractility and serum glucose, insulin, cholesterol, TG and body weight. 31 Nakeeb et al. 32 suggested that insulin resistance alone might be responsible for gallbladder dysmotility, resulting in gallstone formation. Gallbladder motility has been shown to be impaired in subjects with hypertriglyceridaemia, compared with BMI-matched controls. 17
In summary, the results of the present study revealed significant relationships between serum leptin and Lp(a), ApoB and ApoA-1 levels in patients with cholelithiasis. These findings support the hypothesis of altered biliary cholesterol metabolism, characterized by lower ApoA-1 and higher ApoB serum concentrations in cholelithiasis. Patients with cholelithiasis have higher leptin levels and an altered lipoprotein profile compared with controls, with increased leptin levels being associated with increased Lp(a) and ApoB levels and decreased ApoA-1 levels in those with cholelithiasis.
Footnotes
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.