
Abstract
Objectives
To examine correlations between the uptake of 2-deoxy-2-[18F]fluoro-D-glucose (FDG) by primary tumours and axillary lymph nodes, and clinical and biological tumour prognostic parameters, in patients with newly diagnosed breast cancer.
Methods
Newly diagnosed breast cancer patients who had received a dual-phased FDG positron emission tomography/computed tomography scan for pretreatment staging were enrolled retrospectively. Maximal standardized uptake values at 1 h (SUV1), 2 h (SUV2), and retention indices (RI) of the tumours and ipsilateral axillary lymph nodes were measured. SUV and RI were compared with clinical and biological prognostic parameters.
Results
A total of 32 patients participated in the study. Tumour FDG uptake correlated with histological grade and tumour size. FDG uptake in axillary lymph nodes correlated positively with lymph node status, metastasis status and clinical stage. RI values for the tumour and lymph nodes were significantly positively correlated with human epidermal growth factor receptor-2 positivity.
Conclusions
FDG uptake in tumours and lymph nodes showed correlations with some clinical and biological parameters, and may serve as a predictive marker of tumour biological behaviour in breast cancer.
Keywords
Introduction
Breast cancer is one of the most common malignancies in women and the second leading cause of cancer death in women in the developed world. 1 The incidence of breast cancer has increased in recent decades. 2 Precise preoperative evaluation of breast cancer is important because it may affect individual treatment decisions. Furthermore, some prognostic parameters (including primary tumour size, histological tumour grade, axillary lymph node involvement. and expression status of the oestrogen receptor [ER], progesterone receptor [PR] or human epidermal growth factor receptor-2 [c-erbB-2]) in the primary tumour have been reported to be related to the disease response to chemotherapy, and to influence subsequent patient survival. 3
Positron emission tomography (PET) using 2-deoxy-2-[18F]fluoro-D-glucose (FDG) has been integrated with computed tomography (CT); this technique provides the precise evaluation of not only the structures and locations of pathological lesions, but also the level of glucose metabolism of those lesions. The standardized uptake value (SUV), which is the most popular semiquantitative parameter for objectively evaluating PET, is proportional to the rate of glucose metabolism within the normal range of serum glucose concentrations,4,5 and is used to characterize tumour metabolism in vivo. Using FDG PET/CT, whole-body evaluations of the nature of a tumour and its metastases can be achieved in the early stages of diagnosis. 6 PET/CT is increasing in popularity as a tool for the evaluation of patients with breast cancer. It has been used for initial staging, restaging of locoregional recurrence and for monitoring responses to therapy.7–9 Some studies have further demonstrated associations between prognostic impact and FDG uptake.10,11
Regarding the relationship between biological prognostic parameters and metabolic activity, various studies have shown that the FDG uptake of a tumour is associated with some biological prognostic parameters.12–15 However, these results remain controversial. Moreover, to the best of our knowledge, some studies have used dual-phased FDG PET to identify the correlation between a tumour’s metabolic activity and biological parameters,12,16,17 but only one study has used the FDG uptake of the lymph nodes as an evaluation parameter. 18
Therefore, the aims of the present study were to examine correlations between the FDG uptake by breast tumours and axillary lymph nodes, as assessed using dual-phased FDG PET/CT scans, and histopathological and immunohistochemical tumour prognostic parameters, in patients with newly diagnosed breast cancer.
Patients and methods
Patients
This study retrospectively analysed the medical records of patients with breast cancer who were treated in the Department of Surgery, Kaohsiung Medical University Hospital, which is a tertiary medical centre in southern Taiwan. The dates for inclusion in this study were between August 2005 and November 2012. Patients were included if they met the following inclusion criteria: (i) newly diagnosed with breast cancer but not receiving therapy; (ii) received a whole-body dual-phased FDG PET/CT scan for pretreatment staging; (iii) received the surgical treatments of mastectomy and ipsilateral axillary lymph node dissection; (iv) tumour samples from the operation were evaluated using immunohistochemical staining to examine the presence of ER, PR, c-erbB-2 and p53 proteins. Patients were excluded according to the following criteria: (i) age < 20 years; (ii) previous diagnosis of malignancy. The study design and review process was approved by the Institutional Review Board (KMUH-IRB-20140163) of Kaohsiung Medical University Hospital. Patient consent was not required because all of the clinical data were retrospectively collected via medical chart review. Patients were staged according to the 7th edition of the breast cancer staging system of the American Joint Committee on Cancer. 19
FDG PET/CT imaging
Every patient had fasted for ≥6 h prior to the examination. Blood glucose levels were measured using standard techniques, and needed to be <150 mg/dl prior to injection of the tracer. Each patient was asked to lie comfortably to reduce muscular uptake after the intravenous injection of 370 MBq 18 F FDG (Positron Technology, Kaohsiung, Taiwan). At 50 min after the administration of FDG, each patient underwent whole-body imaging with a dedicated, dual-modality PET/CT system (Discovery ST 16; GE Medical Systems, Waukesha, WI, USA). Spiral low-dose CT (with 80 mA, 140 kV, 3.75 mm section thickness, 1.0 s per CT rotation, and 59.0 mm/s table speed) was performed with a craniocaudal direction that covered the area from the vertex to the middle thigh, for the purpose of attenuation correction and precise anatomical localization. Thereafter, emission acquisition was conducted in a reverse direction. The emission scan time per bed position was 4 min. Seven to eight bed positions per patient were acquired, depending on the patient’s height. All images were taken in the supine position. No intravenous contrast medium was administered. An additional delayed-phase scan (covering the area from the neck to the lower chest) was performed 2 h after FDG injection. After decay correction, PET data were iteratively reconstructed (via the ordered-subset expectation maximization method) with attenuation correction, and reoriented in three orthogonal slices. Whole-body maximum-pixel-intensity projections were also used for visual evaluation. A workstation (Xeleris Functional Imaging Workstation; GE Medical Systems) was used for image display, visualization and data analysis.
ROI measurements
Accumulation of the 18 F FDG was analysed semiquantitatively by calculating the SUV of lesion sites. SUV values were calculated as the ratios of radiopharmaceutical activity to tissue volume and administered radiopharmaceutical activity to body weight, as follows:

Using CT images from FDG PET/CT procedures, the maximal SUV (SUVmax) was measured by placing the region of interest (ROI) on the hypermetabolic lesions, which included tumours in the breasts, axillary lymph nodes and distant metastases (if presented), as demonstrated in Figure 1. In cases of low FDG uptake in the axillary region (SUVmax < 2), the ROI was carefully drawn over the corresponding axillary lymph nodes, as depicted on the CT images. SUVmax of lesions at 1 h (SUV1) and 2 h (SUV2) were recorded. Retention indices (RI, %) of these lesions were calculated as follows:
Selected regions of interest on a dual-phased 2-deoxy-2-[18F]fluoro-D-glucose (FDG) positron emission tomography/computed tomography (PET/CT) image from a 51-year-old woman with grade 2 invasive ductal carcinoma of the left breast (clinically at stage III). (A) On the maximum-pixel-intensity projection, FDG-avid lesions were confined to the left chest (arrow) and the ipsilateral axillary regions (arrowhead). Fused PET/CT images helped to localize hypermetabolic lesions to the left axillary lymph nodes (B) and left breast tissue (C). Dual-phased maximal standardized uptake values and retention indices of the primary tumour and metastatic axillary lymph nodes were recorded. The colour version of this figure is available at: http://imr.sagepub.com.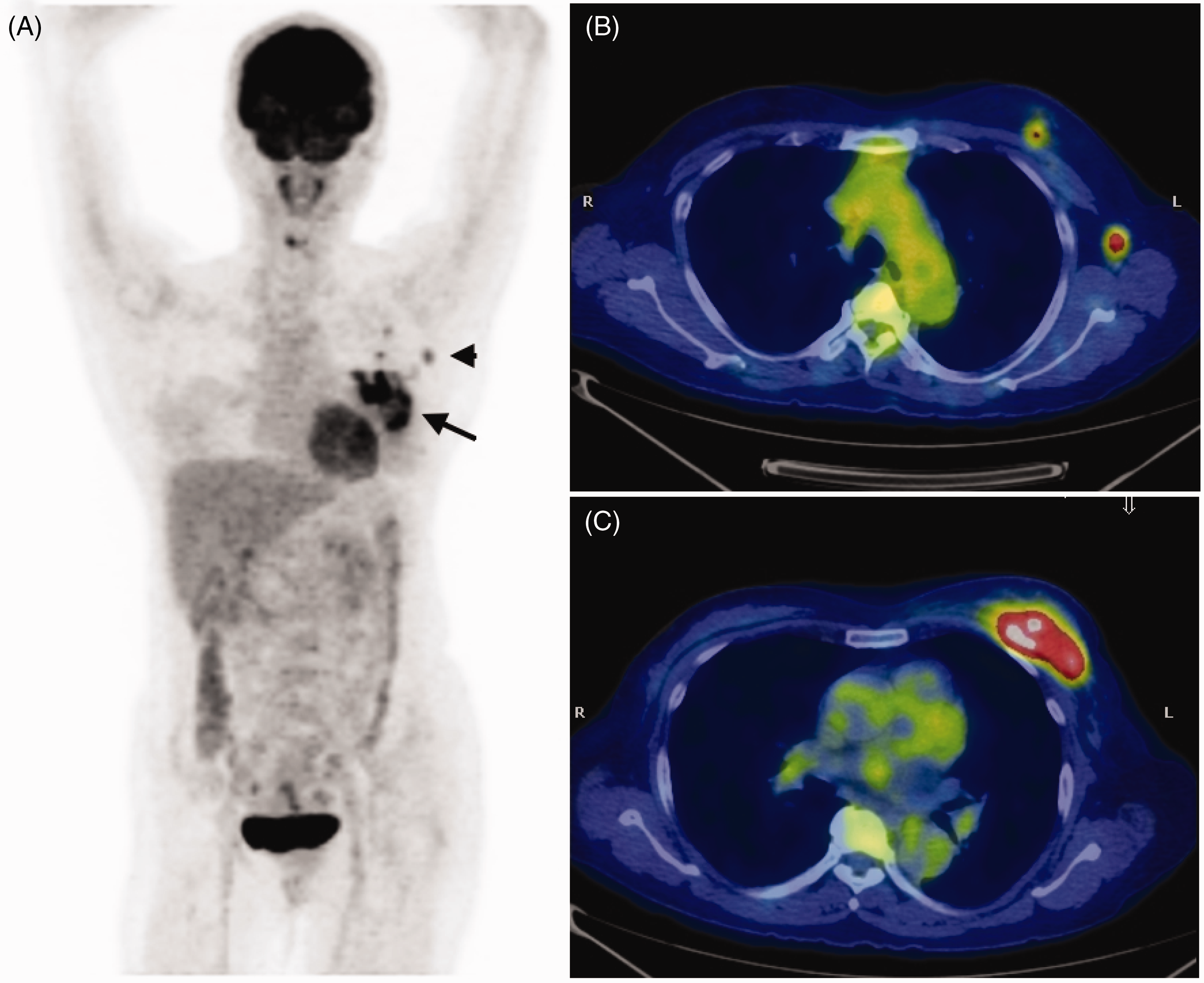

Immunohistochemical staining
Representative sections from surgical tumour samples were formalin-fixed and embedded in paraffin wax prior to standard histopathological and immunohistochemical examination. Primary monoclonal antibodies against ER (clone 6F11; Leica Biosystems, Singapore), PR (clone 16; Leica Biosystems), c-erbB-2 (clone CB11; BioGenex, Fremont, CA, USA) and p53 (clone DO-7; DAKO, Glostrup, Denmark) proteins were applied. A Leica BOND-MAX™ (Leica Microsystems, Milton Keynes, UK) automated system was used for immunohistochemical staining, according to the manufacturers’ instructions. Receptor staining status was defined as positive or negative, based on cut-offs of 10% nuclear staining for ER and PR. C-erbB-2 positivity was defined by tumours that exhibited immunohistochemical staining scores of 3 + (i.e. > 30% of tumour cells exhibited complete staining) and 2 + (i.e. ≤ 30% of tumour cells exhibited complete staining and further analysis of in situ hybridization with fluorescence revealed ERBB2 gene amplification [encoding the c-erbB-2/Her-2 protein]). Triple-negative tumours were defined as those with negative staining results for ER, PR and c-erbB-2. P53 nuclear staining was scored as positive or negative. Slides were reviewed by experienced pathologists who were blinded to the FDG PET/CT results and the patients’ clinical presentations.
Statistical analyses
Statistical analyses were performed using SAS® version 9.3 statistical software (SAS Institute Inc., Cary, NC, USA). Differences in the SUV of the lesions between the categories of tumour behaviour (i.e. tumour grade and ER, PR, c-erbB-2 status) were tested using nonparametric Wilcoxon’s rank sum test (when two categories were compared) or Kruskal–Wallis test (when more than two categories were compared). Spearman’s rank correlation coefficient was used to test the relationship between tumour SUV and tumour size. Statistical significance was defined as a P-value < 0.05.
Results
Demographic and clinical characteristics at diagnosis of patients (n = 32) with newly diagnosed breast cancer who provided data for a retrospective study to investigate the relationship between 2-deoxy-2-[18F]fluoro-D-glucose uptake by primary tumours and axillary lymph nodes, and clinical and biological tumour prognostic parameters.

Data presented as mean ± SD or n (%) of patients.
IDC, invasive ductal carcinoma; ILC, invasive lobular carcinoma.
All breast tumours could be visualized on FDG PET/CT images. The mean ± SD SUV1 and SUV2 of the tumours were 4.42 ± 3.00 and 5.34 ± 4.30, respectively. The mean ± SD SUV1 and SUV2 of the ipsilateral axillary lymph nodes were 4.36 ± 4.40 and 5.42 ± 5.90, respectively.
Regarding the tumour behaviour of dual-phased SUV measurement, 21 (65.6%) lesions exhibited increases in metabolic activity; the remaining 11 (34.4%) lesions exhibited decreases. The mean RI value of the tumours was 10.1%. Regarding the FDG uptake in lymph nodes, 20 (62.5%) patients exhibited increases in metabolic activity in the axillary lymph nodes; 12 (37.5%) patients exhibited decreases. The mean RI value in the lymph nodes was 8.3%.
Correlations between maximal standardized uptake values (SUV) at 1 h (SUV1) and 2 h (SUV2), and retention indices (RI) of primary breast cancer tumours, and clinical and biological prognostic parameters.

Data presented as mean±SD.
Statistically significant between-group difference; nonparametric Wilcoxon’s rank sum test (when two categories were compared) or Kruskal–Wallis test (when more than two categories were compared).
ER, oestrogen receptor; PR, progesterone receptor; C-erbB-2, human epidermal growth factor receptor-2; NS, no statistically significant between-group differences (P ≥ 0.05).
Correlations between maximal standardized uptake values (SUV) and retention indices (RI) of primary breast cancer tumours and tumour size.

Correlations between maximal standardized uptake values (SUV) and retention indices (RI) of axillary lymph nodes, and clinical and biological prognostic parameters.
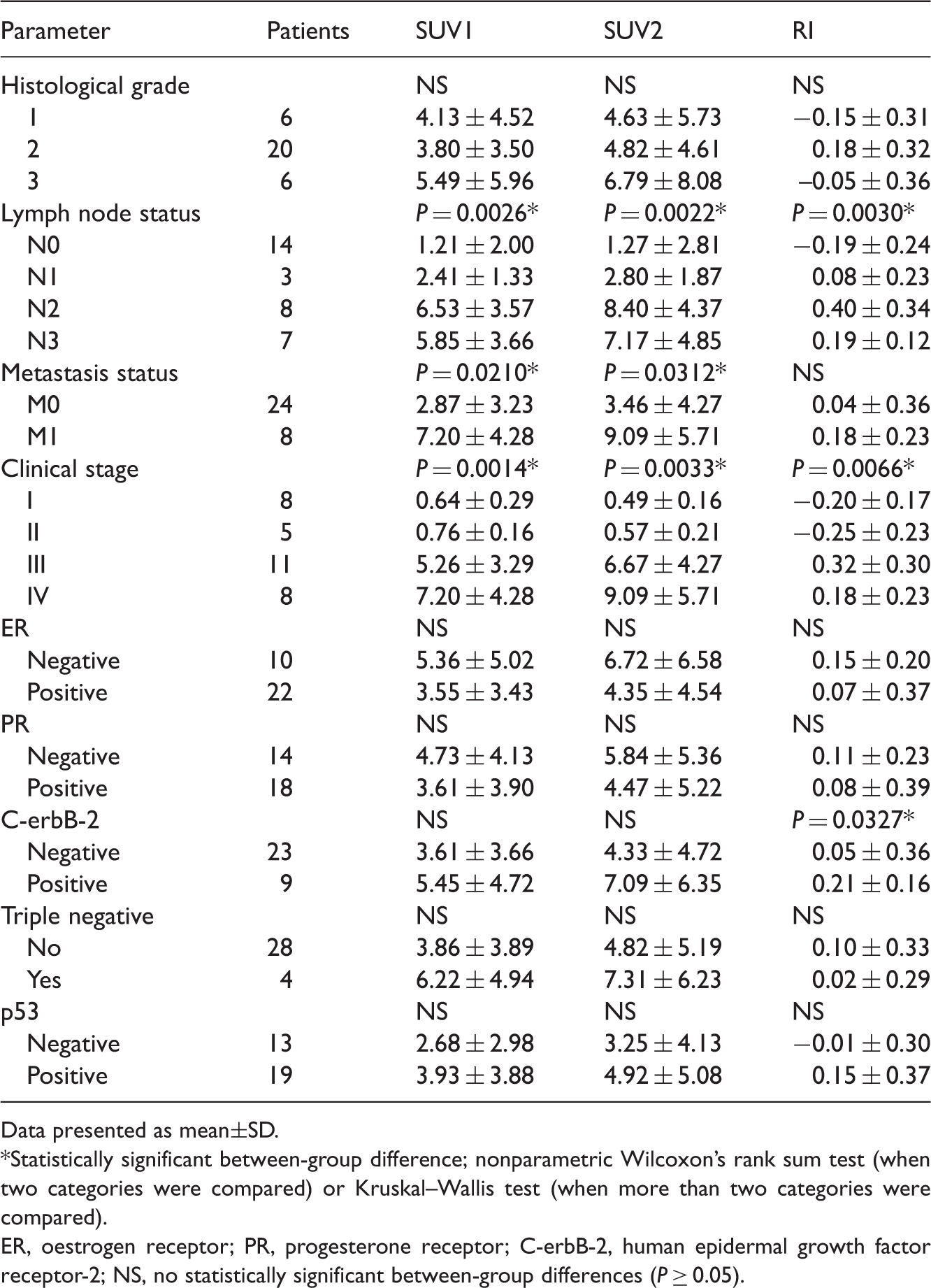
Data presented as mean±SD.
Statistically significant between-group difference; nonparametric Wilcoxon’s rank sum test (when two categories were compared) or Kruskal–Wallis test (when more than two categories were compared).
ER, oestrogen receptor; PR, progesterone receptor; C-erbB-2, human epidermal growth factor receptor-2; NS, no statistically significant between-group differences (P ≥ 0.05).
Positive ER and positive PR receptor protein statuses were detected in 22 (68.8%) and 18 (56.3%) patients, respectively. For all patients, SUV1, SUV2 and RI in ER- or PR-negative breast tumours were higher than those in ER- or PR-positive breast tumours, but the differences were not significant.
Immunohistochemical staining for c-erbB-2 oncoprotein was positive in nine (28.1%) patients. Higher tumour FDG uptakes were associated with tumour c-erbB-2 positivity, particularly for the RI value, which met statistical significance (P = 0.0437) (Table 2). Furthermore, there was a tendency towards a higher FDG uptake in axillary lymph nodes in cases in which the tumours were positive for c-erbB-2 protein; the RI of the lymph nodes met statistical significance (P = 0.0327) (Table 4).
Only four of 32 patients (12.5%) had tumours with triple-negative immunohistochemical staining. There was no significant relationship between FDG uptake and presence of triple negativity.
Regarding the immunostaining for p53, 19 (59.4%) patients exhibited nuclear positivity. Although higher FDG uptake was noted in p53-positive tumour cells, the relationship between the FDG uptake and p53 expression was not statistically significant.
Discussion
In the clinical management of breast cancer, some important prognostic parameters (including primary tumour size, histological tumour grade, axillary lymph node involvement, and expression status of ER, PR and c-erbB-2 proteins in the primary tumour), are thought to influence clinical judgement and prognostic outcome. 3 PET/CT scanning can provide combined anatomical and metabolic images of pathological lesions in patients with newly diagnosed breast cancer. Tumour cells in the vast majority of breast cancers have significantly increased glycolysis and therefore utilize the administered FDG to a greater extent than the normal cells. 20 However, the intensity of FDG accumulation in breast cancer cells may vary with the extent of the disease, tumour differentiation, histological subtypes, and different biological prognostic parameters. 21 Several studies have produced controversial results regarding the correlations between FDG uptake and clinical, pathological and biological prognostic parameters in breast cancer.12–15 The present study, using dual-phased FDG PET/CT, attempted to determine possible relationships between metabolic activities of tumours and axillary lymph nodes, and clinical and biological prognostic parameters in breast cancer. Although further confirmation with larger patient populations may be needed, the present study may advance the concept that the noninvasive measurement, FDG PET/CT, might predict the biological behaviour of tumours and further correlate the behaviour with the prognoses of patients with breast cancer.
Uptake of FDG in tumour cells has been observed to increase for several hours following its injection. 22 This phenomenon may be related to the graded concentration of FDG in tumour cells, low glucose-6-phosphatase activity, and increases in glucose uptake through the glucose transporter in these cells.23–26 In contrast, incremental FDG uptake is rare in inflammatory cells or normal tissues. Due to these differences in the time course of FDG uptake between malignant and inflammatory cells, delayed PET scans should produce higher lesion-to-background ratios: these would allow for the more precise differentiation of inflammatory cells from malignant cells and thus improve diagnostic accuracy, particularly for tumours with low FDG uptake. Dual-phased FDG PET/CT has been reported to result in higher sensitivity and specificity in diagnoses of pulmonary nodules,27,28 uterine cervical cancer 29 and hepatic lesions. 30 Additionally, dual-phased FDG PET/CT can provide diagnostic value, especially in the evaluation of lymph node metastases in oesophageal cancer, 31 cervical cancer 32 and nonsmall-cell lung cancer. 33 Regarding breast cancer, dual-phased FDG PET/CT imaging improves the accuracy in the evaluation of breast cancer with low FDG uptake, 34 improves the discrimination between noninvasive and invasive cancers, and provides superior sensitivity in the detection of small cancers and cancers in dense breast tissue.35,36 In the present study, 21 (65.6%) lesions exhibited increased metabolic activity in delayed-phase PET images. The mean tumour RI value across all patients was 10.1%, which is similar to that reported by García Vicente et al. 17
Pretreatment evaluation of lymph node involvement of tumour cells is important. Previously, an accurate lymph node status could only be obtained after surgery, which is frequently associated with high rates of morbidity. 37 Based on depictions of tumour glucose metabolism, the quantitative FDG uptake of axillary lymph nodes may provide valuable adjunctive information to that provided by conventional preoperative clinical assessments. Inoue et al. 38 reported that a combination of the SUV for primary tumours and focal axillary regions is a highly significant prognostic factor that is independent of the influence of clinical tumour size (T stage) and lymph node status (N stage) in multivariate analyses. SUV of the metastatic lymph nodes may be an independent prognostic factor for disease recurrence in patients with breast cancer. 11 In the present study, higher FDG uptakes in lymph nodes were associated with advanced N stage, M stage and overall clinical stage; in addition, SUV1, SUV2 and RI values were statistically significant. Similar results were reported in other research, but in that work only the SUV1 and SUV2 of lymph nodes were significantly correlated with N stage. 18
The ER are found inside cells and are activated by the hormone, oestrogen. Once activated, ER are able to translocate into the nucleus and bind to DNA, to regulate the activities of different genes. The administration of tamoxifen, an ER antagonist, has been one of the most successful hormone treatments for ER-positive breast cancer. 39 Controversial results regarding the relationship between FDG uptake and ER expression status have been noted in the literature, however.12–14,40–42 A significant correlation was demonstrated between ER negativity and higher SUV in a prospective study that examined 132 patients with breast cancer. 40 Some other studies have reported similar results.13,41,42 However, some reports using dual-phased FDG PET provided contrary results.12,14 In the present study, although not meeting statistical significance, SUV1, SUV2 and RI of the ER-negative tumours were higher than those of the ER-positive tumours, which is consistent with the results that have been reported by others.16,17
Like ER, PR is a protein that is located inside the cell. PR is activated by the steroid hormone, progesterone. After activation, a dimerized complex enters the nucleus and binds to DNA. Further proteins are then produced. The correlation between PR expression and FDG uptake is also a subject of controversy. Kim and Sung, 15 and Heudel et al., 43 demonstrated a significant correlation between PR negativity and SUV of the breast tumour. In contrast, others found no statistically significant correlation.14,42 In the present study, SUV and RI of PR-negative tumours were higher than those of PR-positive tumours, but the differences were not statistically significant.
C-erbB-2 is a protein that, in humans, is encoded by the human epidermal growth factor 2 (ERBB2) gene. This protein has become an important biomarker and a target of cancer therapy. Amplification of this oncogene or upregulation of the protein have been shown to play important roles in promoting breast cancer growth. For example, c-erbB-2-positive breast tumours tend to have a more aggressive clinical behaviour than other types of breast cancer, and c-erbB-2 positivity independently predicts decreases in disease-free survival and lower overall survival rates. 44 In the present study, nine patients (28.1%) had tumours with positive c-erbB-2 staining. A significant correlation was noted between tumour RI values and c-erbB-2 positivity (P = 0.0437). The result is similar to that reported by García Vicente et al. 17 To the best of our knowledge, only one report has mentioned the correlations between biological prognostic markers and metabolic parameters of axillary lymph nodes; this study reported that PR negativity of breast cancer correlated significantly with FDG uptake in lymph nodes. 18 In the present study, tumour c-erbB-2 status was significantly associated with FDG uptake in axillary lymph nodes (P = 0.0327 for RI). This phenomenon may be explained by the sustained elevation of glycolysis in c-erbB-2-positive tumour cells, particularly when they have metastasized. However, this hypothesis requires confirmation. Based on the present study, patients with higher RI values in the tumour and axillary lymph nodes tended to have more c-erbB-2 protein on tumour cells. The clinical importance may be that the tumour and lymph node RI values are correlated with patients who have a poorer prognostic outcome.
The triple-negative phenotype is a relatively uncommon subtype of breast cancer. In the present study, this subtype comprised 12.5% of the tumours examined (four patients). Although no significant relationship between FDG uptake and presence of triple negativity was present, higher FDG uptakes were noted in triple-negative tumours, which is a similar finding to other reports. 16
The present study had a number of limitations. First, although the SUV is generally accepted as the most practical index for assessing the disease activity of cancer, many factors can influence the reliability of SUV measurements: these include the time interval between injection and imaging, patient weight and body habitus, partial volume effects, and the reconstruction algorithm utilized. 45 Secondly, the technique of counting the ER, PR, c-erbB-2 and p53 scores reflects the percentage of tumour cells that are stained without including nontumour cells. This method can correct for the stromal fraction. However, the FDG PET/CT scan does not correct for this fraction. This discordance can be minimized by recording the immunohistochemical scores under the microscopic area with the highest tumour fraction and the pixel with the maximal SUV from the tumour volume, at the PET scan. Thirdly, the present study had a small number of patients and a retrospective design. Only four patients with triple-negative tumours were enrolled and this may have affected the statistical results. Further prospective studies examining larger patient populations should be conducted.
In conclusion, FDG uptakes of primary tumours and lymph nodes have biological importance and appear to be correlated with some prognostic parameters in patients with newly diagnosed breast cancer. Among the biological prognostic parameters, the most notable correlations found in the present study were between c-erbB-2 protein positivity and FDG uptake in tumours and lymph nodes.
Footnotes
Acknowledgements
We thank Dr Shiou-Fu Lin at the Department of Pathology, Kaohsiung Medical University Hospital, Kaohsiung, Taiwan, and Dr Sheau-Fang Yang at the Department of Pathology, Kaohsiung Municipal Ta-Tung Hospital, Kaohsiung, Taiwan, for their efforts to review the pathological slides and define the scores of the immunohistochemical stains.
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.