
Abstract
Objectives
To investigate the correlation between preoperative anxiety and emergence delirium (ED), and to identify other factors that contribute to ED (such as invasiveness of surgery), in preschool-age paediatric patients undergoing strabismus surgery.
Methods
This prospective observational study enrolled Korean children (aged 2–5 years), scheduled for strabismus surgery. After completing the modified Yale Preoperative Anxiety Scale, general anaesthesia was induced. Postoperatively, Pediatric Anesthesia Emergence Delirium (PAED) scores (used as an index of the degree of ED) and a four-point delirium scale (ED incidence), were collected and measured every 5 min. Patients were categorized according to the degree of surgical invasiveness: group U-S, single-muscle correction in a unilateral eye; group U-M, multiple-muscle correction in a unilateral eye; group B-S, single-muscle correction in bilateral eyes; group B-M, multiple-muscle correction in bilateral eyes.
Results
A total of 90 paediatric patients participated in the study. Maximum PAED scores did not correlate with the presence of preoperative anxiety. The maximum PAED score of group B-M was significantly higher than scores observed in other groups.
Conclusions
Preoperative anxiety was not related to ED in preschool-age paediatric patients undergoing strabismus surgery. The incidence and severity of ED was higher in patients who underwent more complicated strabismus surgery, compared with those undergoing simpler procedures.
Introduction
Emergence delirium (ED) is one of the most common complications in children after general anaesthesia; it is a disturbance in a child’s awareness of (and attention to) his or her environment with disorientation and perceptual alterations, including hypersensitivity to stimuli and hyperactive motor behaviour, in the immediate postanaesthesia period.1–5 ED occurs within 30 min of recovery from anaesthesia and is usually a self-limiting phenomenon.6,7 However, ED may cause injury in paediatric patients, necessitating extra recovery nursing, and is associated with decreased satisfaction scores in parents. 8 Although various risk factors for ED have been reported in a large number of published studies,1–8 its aetiology and pathogenesis remain unclear.
Young age, especially between 2–5 years old, is a well-known risk factor for ED;2,5,9–11 consequently, many studies on ED have focused on that age range.2,3,12–14 Ophthalmological procedures, such as strabismus surgery, are also associated with an increased incidence of ED.2,4,5,9–11,14–18 Strabismus surgery, which is one of the most commonly undertaken surgeries in paediatric patients, may cause visual disturbance in the recovery phase, which can result in ED.5,17,18
A child’s preoperative anxiety level is another well-known risk factor for ED;5,9,16,17,19,20 several studies have reported that heightened preoperative anxiety is associated with heightened incidence of ED.16,18–20 Additionally, ED was reported to be associated with the level of invasiveness of the procedure. 21
However, in our experience of anaesthesia in children receiving strabismus surgery, preoperative anxiety does not appear to be correlated with ED. Furthermore, children who are less anxious preoperatively are often observed showing more ED (and, indeed, vice versa) during recovery from general anaesthesia. Considering that invasiveness may affect the occurrence of ED, this would suggest that binocularity and the number of muscles involved in strabismus surgery might influence ED.
The Pediatric Anesthesia Emergence Delirium Scale 10

Items 1, 2, and 3 are reverse-scored, as follows: 4, not at all; 3, just a little; 2, quite a bit; 1, very much; 0, extremely. Items 4 and 5 are scored as follows: 0, not at all; 1, just a bit; 2, quite a bit; 3, very much; 4 extremely. Scores for each item are summed to obtain the total PAED scale score. Degree of emergence delirium increases directly with total score.
Patients and methods
Study population
This prospective observational study enrolled consecutive American Society of Anesthesiologists physical status 1 and 2 South Korean children, aged 2–5 years, scheduled for strabismus surgery in the Department of Anaesthesiology and Pain Medicine, Seoul St Mary’s Hospital, College of Medicine, The Catholic University of Korea, Seoul, Republic of Korea, between September 2010 and August 2011. All patients were allowed to take solid food up to 6 h before surgery and water up to 2 h before surgery. Children with pre-existing neurological disorders and those whose parents refused to enrol them were excluded. This study was approved by the Ethical Committee of Seoul St Mary’s Hospital, Catholic University of Korea (ID: KIRB-00353_26-003) and was registered at http://www.cris.nih.go.kr (ID: KCT0000304). Written informed consent was obtained from the parents of each patient.
Study protocol
The patients visited a day surgery centre (DSC) at Seoul St Mary’s Hospital on the operation day, with their parents. One designated DSC nurse who was trained in the use of the modified Yale Preoperative Anxiety Scale (m-YPAS) 22 administered the m-YPAS upon the child’s admission to the DSC. The resulting m-YPAS scores were not provided to other researchers or to medical personnel until data analysis. Next, intravenous (i.v.) access was established with a 22-gauge angio catheter. Approximately 10 min prior to entering the operating room, 0.1 mg/kg midazolam i.v. 23 was administered as a premedication, and the patient was transferred to the operating room, by medical personnel, on becoming drowsy.
Electrocardiogram, noninvasive blood pressure, heart rate, and pulse oximetry were measured using standard techniques continuously at 5-min intervals, starting from the patient’s arrival in the operating room. General anaesthesia was induced with 2 mg/kg propofol i.v. bolus and 0.6 mg/kg rocuronium i.v. bolus. After tracheal intubation, anaesthesia was maintained with 2 vol% sevoflurane, 50% N2O, and 50% O2, keeping the end-tidal CO2 between 30 and 35 mmHg. Strabismus surgeries were performed by one surgeon . In patients who had strabismus surgery in one eye, the treated eye was protected with gauze and a transparent eye shield after applying eye ointment . In patients who had strabismus surgery in both eyes, after eye ointment was applied to both eyes, the eye that had a greater reaction to exudate was protected with gauze and a transparent eye shield; the other eye was protected only with a transparent eye shield.
At the end of surgery, sevoflurane was discontinued; 75 µg/kg ondansetron i.v., 0.9 mg/kg ketorolac i.v., 0.2 mg/kg pyridostigmine i.v. and 0.08 mg/kg glycopyrrolate i.v. were administered. After extubation, each patient was brought to the postanaesthetic care unit (PACU).
On arrival in the PACU, one of the parents or caregivers was called to be with the child. A designated PACU nurse was trained in the administration of the PAED scale before beginning this study. This trained nurse administered the PAED scale 10 at 5-min intervals, from arrival in the PACU until discharge to the DSC, to evaluate the degree of ED. The highest PAED score, indicating most symptoms of ED, was deemed the final score for each patient. The nurse also graded clinically observed delirium at 5-min intervals on the four-point delirium scale also designed to measure ED, described above. 2
If the ‘face, legs, activity, crying, consolability’ scale score was >3 for >5 min , the PACU nurse notified the anaesthesiologist and then administered 1 µg/kg fentanyl i.v.. When patients showed signs of retching or vomiting, 0.15 mg/kg metoclopramide i.v. was administered as a rescue antiemetic. 0.1 mg/kg midazolam i.v. was administered when scores on the four-point ED scale were ≥3 for >5 min.
The following were also recorded: duration of surgery; duration of anaesthesia (from induction to extubation); time to awakening (time from arrival at the PACU to the first response to a verbal command); duration of stay in the PACU (from admission to the PACU following surgery to the time of discharge to the DSC); fentanyl administration; duration of DSC stay (from the time of postoperative DSC admission to the time of discharge from the DSC).
After study completion, the correlation between m-YPAS and PAED scores was examined. Patients were classified into a high-anxiety group if their m-YPAS scores were >40, and a low-anxiety group if their scores were ≤40.24,25 The incidence of ED in the high- and low-anxiety groups was compared.
Patients and their data were also assigned to the following groups according to the invasiveness of the surgery: group U-S, single-muscle correction in a unilateral eye; group U-M, multiple-muscle correction in a unilateral eye; group B-S, single-muscle correction in bilateral eyes; and group B-M, multiple-muscle correction in bilateral eyes. Then, the maximum PAED score and incidence of ED in each group were compared.
Statistical analyses
All statistical analyses were performed using the SPSS® statistical package, version 18.0 (SPSS Inc., Chicago, IL, USA) for Windows®. To estimate the sample size needed, a two-sided test with a significance level of α = 0.05 and β = 0.80 was used to detect a correlation of 0.30 between m-YPAS and PAED. Thus, the study required a minimum of 84 patients. To allow for the exclusion of some patients, the study enrolled 90 paediatric patients.
Bivariate correlation analysis between m-YPAS, age, sex, invasiveness of surgery, duration of surgery and anaesthesia, and maximum PAED score was performed using Spearman’s rank correlation coefficient. Then, stepwise multiple regression analysis was conducted for those factors that were shown to correlate with maximum PAED score. All parametric data were compared using one-way analysis of variance with post hoc Bonferroni’s correction for multiple comparisons, and presented as mean ± SD. Nominal data were analysed with χ2-test or Fisher’s exact test were expressed as numbers or percentages. A P-value < 0.05 was considered statistically significant. A receiver operating characteristic (ROC) curve method was employed to identify the appropriate cut-off maximum PAED score for the presence of ED following strabismus surgery in paediatric patients.
Results
This study enrolled 90 paediatric patients (mean ± SD age, 4.0 ± 1.3 years; mean ± SD weight, 18.2 ± 4.4 kg). The mean ± SD m-YPAS and mean ± SD maximum PAED scores were 46.1 ± 20.9 and 14.7 ± 3.2, respectively. The m-YPAS and the maximum PAED score were not significantly correlated (r = −0.018; Figure 1). Of the 90 patients, 41 showed low anxiety and 49 showed high anxiety, based on their preoperative m-YPAS scores. Demographic data were similar between the low- and high-anxiety groups (Table 2). In total, 21 patients (51.2%) in the low-anxiety group and 23 patients (46.9%) in the high-anxiety group showed ED; this difference was not statistically significant. The area under the ROC curve for PAED scores >16 was 0.98, with a true-positive rate (sensitivity) of 0.94 and a false-positive rate (1 – specificity) of 0.03, thereby demonstrating that a threshold score of 16 was optimal to discriminate between the presence and absence of ED (Figure 2).
Receiver operating characteristic curve for sensitivity (true positive) and 1 – specificity (false positive), for scores on the Pediatric Anesthesia Emergence Delirium scale.
10
For scores of >16, a sensitivity of 0.94 and a 1 – specificity of 0.03 were observed Demographic and clinical characteristics of low- and high-anxiety groups of paediatric patients (aged 2-5 years) scheduled to undergo strabismus surgery, classified according to their preoperative modified Yale Preoperative Anxiety Scale (m-YPAS) score Data presented as mean ± SD or n (%) of patients. Low-anxiety group, m-YPAS scores ≤ 40; high-anxiety group, m-YPAS scores >40. Incidence of emergence delirium (ED) was based on a four-point delirium scale score ≥3 (1, calm; 2, not calm, but could be easily calmed; 3, not easily calmed [moderately agitated or restless]; 4, combative, excited or disoriented). No significant between-group differences (P ≥ 0.05).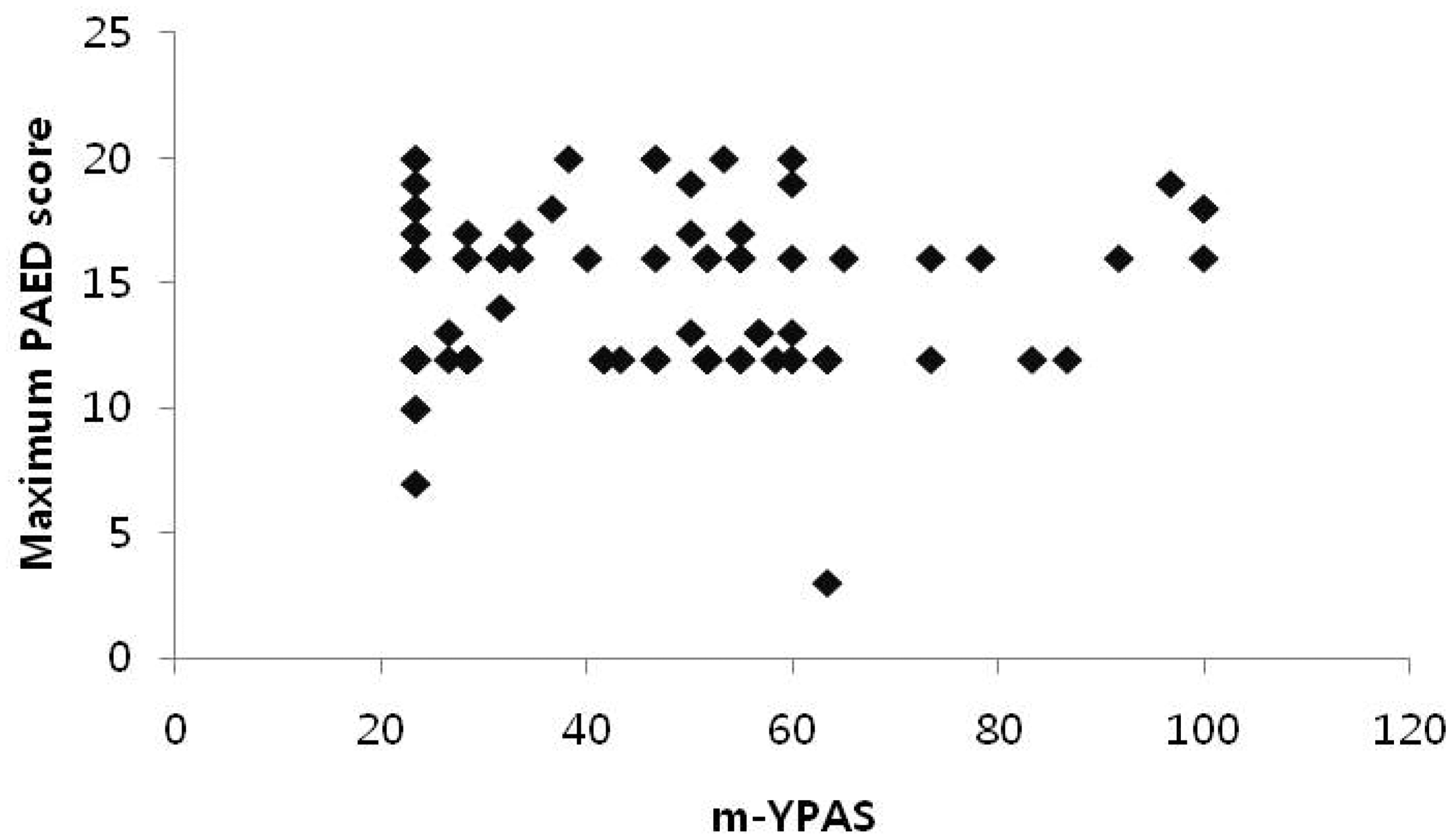


Demographic and clinical characteristics were similar in the four surgical groups (Table 3). Group B-M had significantly longer mean ± SD surgery times (37.2 ± 7.9 min) and mean ± SD anaesthesia times (52.5 ± 8.7 min) compared with the other three groups (P < 0.05 for all comparisons; Figure 3). Group U-M and group B-S had similar mean ± SD surgery times (21.9 ± 3.8 and 20.3 ± 3.7 min, respectively) and similar anaesthesia times (36 ± 4.3 and 33.6 ± 5.0 min, respectively); and both groups had significantly longer surgery and anaesthesia times compared with group U-S (11.0 ± 2.2 min for surgery, 24.1 ± 2.4 min for anaesthesia, P < 0.05; Figure 3).
Differences in duration of surgery and duration of anaesthesia in four surgical groups of paediatric patients (aged 2–5 years) scheduled to undergo strabismus surgery. Group U-S (n = 21), single-muscle correction in a unilateral eye; group U-M (n = 22), multiple-muscle correction in a unilateral eye; group B-S (n = 28), single-muscle correction in bilateral eyes; group B-M (n = 19), multiple-muscle correction in bilateral eyes. *P < 0.05 versus group U-S, †P < 0.05 versus group U-M, ‡P < 0.05 versus group B-S Demographic and clinical characteristics of the four surgical groups of paediatric patients scheduled to undergo strabismus surgery Data presented as mean ± SD or n of patients. Group U-S, single-muscle correction in a unilateral eye; group U-M, multiple-muscle correction in a unilateral eye; group B-S, single-muscle correction in bilateral eyes; group B-M, multiple-muscle correction in bilateral eyes. m-YPAS, modified Yale Preoperative Anxiety Scale.
22
No significant between-group differences (P ≥ 0.05).

Characteristics of emergence delirium and recovery in four surgical groups of paediatric patients (aged 2–5 years) scheduled to undergo strabismus surgery
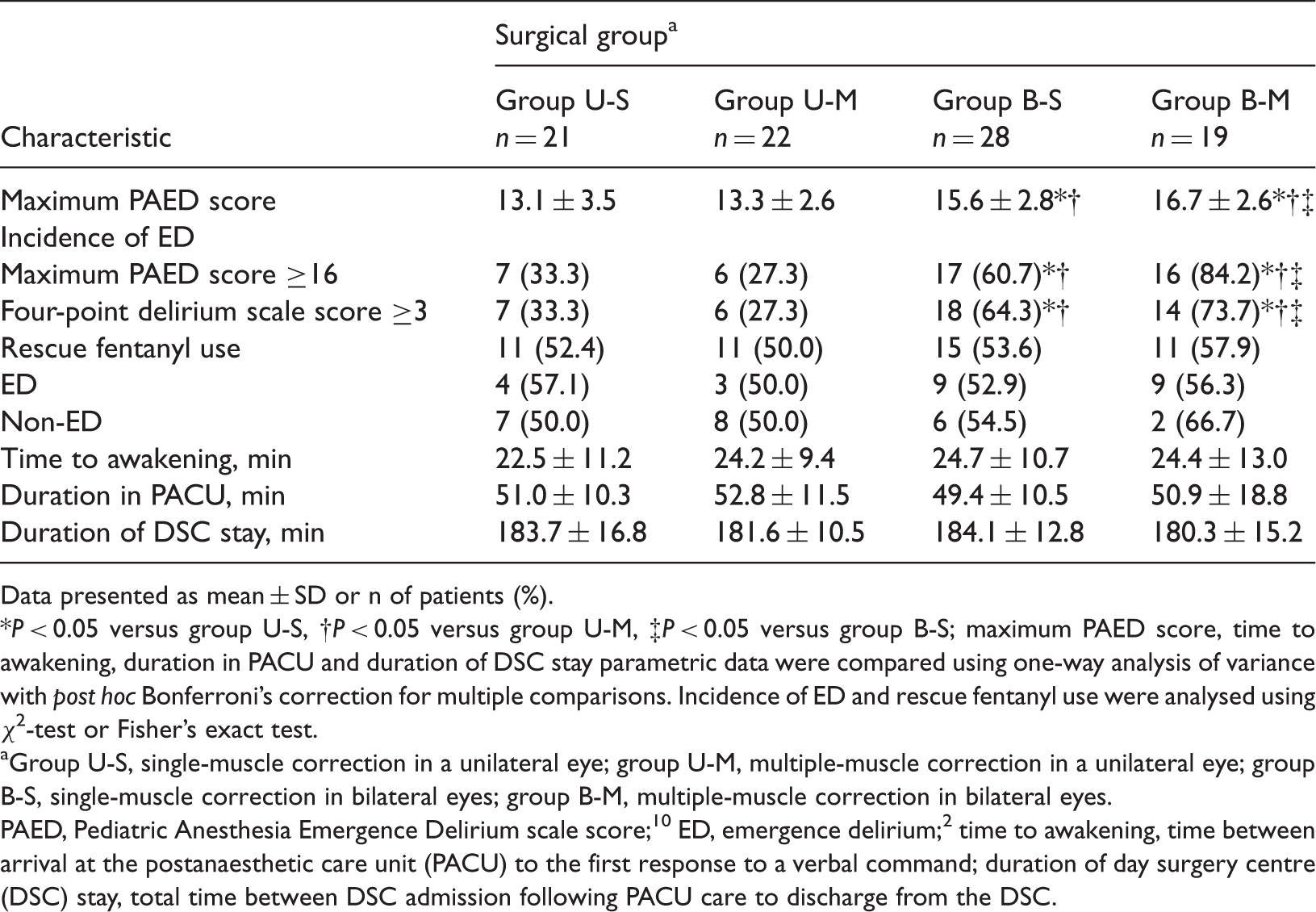
Data presented as mean ± SD or n of patients (%).
P < 0.05 versus group U-S, †P < 0.05 versus group U-M, ‡P < 0.05 versus group B-S; maximum PAED score, time to awakening, duration in PACU and duration of DSC stay parametric data were compared using one-way analysis of variance with post hoc Bonferroni’s correction for multiple comparisons. Incidence of ED and rescue fentanyl use were analysed using χ2-test or Fisher’s exact test.
Group U-S, single-muscle correction in a unilateral eye; group U-M, multiple-muscle correction in a unilateral eye; group B-S, single-muscle correction in bilateral eyes; group B-M, multiple-muscle correction in bilateral eyes.
PAED, Pediatric Anesthesia Emergence Delirium scale score; 10 ED, emergence delirium; 2 time to awakening, time between arrival at the postanaesthetic care unit (PACU) to the first response to a verbal command; duration of day surgery centre (DSC) stay, total time between DSC admission following PACU care to discharge from the DSC.
Factors associated with the development of emergence delirium, as determined using the Pediatric Anesthesia Emergence Delirium (PAED) Scale 10

Bivariate correlation analysis between age, sex, invasiveness of surgery, duration of surgery, duration of anaesthesia, and maximum PAED score.
Discussion
Various studies have established the relationship between preoperative anxiety and emergence delirium in paediatric patients.16,18–20 Although many studies have stated that preoperative anxiety is associated with postoperative delirium, several reports failed to find such a relationship. For example, Faulk et al. 26 reported that preoperative anxiety as assessed by the m-YPAS had no significant effect on the PAED score in children aged between 1 and 12 years, undergoing outpatient dental procedures. Przybylo et al. 9 also failed to demonstrate a relationship between preanaesthetic psychosocial factors and postanaesthetic behavioural abnormalities in children aged between 2 and 9 years, scheduled for strabismus surgery. However, the small size of the study population (27 patients) and the fact that the study included school-age children limited the scope of their conclusions. Unlike school-age children, preschool children are psychologically immature 2 and are easily confused and frightened by unexpected and unpredictable experiences. 11 Therefore, both studies may have resulted in spurious relationships being reported between preoperative anxiety and ED, as opposed to other studies that included predominantly school-age children (who have a better understanding of the situation that they are facing and are more readily controllable). In contrast, the present study focused only on preschool children, aged 2–5 years, who are known to be a high-risk group for ED.
The m-YPAS is reported to be an appropriate tool for assessing children's anxiety during the preoperative period. 22 The PAED score allows for a more complex evaluation of ED, based on actual psychiatric definitions of delirium, and has the highest reliability and validity in examining ED in paediatric patients. 10 The maximum PAED score was not correlated with m-YPAS scores in this present study. The correlation between the incidence of preoperative anxiety and the incidence of ED was also analysed in this present study, but was found to be nonsignificant. The present study employed two methods to evaluate ED: PAED scores that equated to the degree of ED; and a four-point delirium scale that related to the presence, and degree, of ED. 2 The present results indicate that preoperative anxiety and ED were not correlated in preschool-age paediatric patients receiving strabismus surgery.
What, therefore, explains the present results, especially as they pertain to strabismus surgery? First, it has been suggested that visual disturbances may be involved in ED to a greater extent than preoperative anxiety. 7 Secondly, the discomfort associated with wearing the eye shield and gauze patch following application of eye ointment may have played an important role. Finally, administration of midazolam as a premedication may have also influenced the discordance between preoperative anxiety and ED, 26 despite the controversies surrounding its use.3,27,28
Although the PAED scale is the most comprehensive and well-validated scale used to measure the degree of ED, the appropriate cut-off value to denote the presence of ED is still subject to conjecture. In the original study describing the PAED scale, the authors reported that a PAED score of ≥10 was associated with the greatest degree of sensitivity (0.64) and specificity (0.86) for ED. 10 Several other studies also performed ROC curve analysis and reported identical results to those of the original study.12,29 Conversely, in other research, a PAED score of ≥16 was deemed to be an appropriate cut-off value for ED because the PACU nurses and evaluators did not believe that all patients with a PAED score of ≥10 displayed problematic emergence behaviour.14,17 In the present study, a ROC curve analysis was undertaken and demonstrated that a PAED score of >16 was associated with the greatest degree of sensitivity (0.94) and specificity (0.98) for ED, and is therefore the most appropriate cut-off score. This higher cut-off score that we observed (compared with other studies) might be due to visual disturbances resulting from the wearing of the eye patch, such that eye contact (a scoring criterion in the PAED scale), between the child and the PACU nurse, might be difficult. In addition, differences in anaesthetic management, surgical procedures and the age range of the study groups might have influenced this result.
Patients who underwent strabismus surgery in both eyes showed higher maximum PAED scores than did those who received strabismus surgery in one eye, which is consistent with other research. 12 Furthermore, in the present study, the incidence of ED was even increased in those patients receiving bilateral surgery. In bilateral strabismus surgery, patients who received multiple-muscle corrections showed higher maximum PAED scores, and incidence of ED, than did those who received single-muscle correction. Despite the fact that the duration of surgery and anaesthesia were significantly different between groups, it appears unlikely that this would influence ED, considering that the invasiveness of surgery itself was the only factor affecting the occurrence of ED (as demonstrated by the stepwise multiple regression analysis). Moreover, this group difference in ED implies that covering the eyes in different ways had a minimal impact. Another study found that the level of invasiveness of dental surgery was related to ED. 20 Therefore, it seems that binocularity, in combination with the number of muscles involved in surgery, increases the invasiveness of surgery, resulting in an increased incidence and severity of ED.
Pain is considered to be one of the confounding factors in the majority of studies on ED, but it is difficult to fully discriminate pain-related behavioural agitation from ED in preschool-age children. 8 In an attempt to eliminate postoperative pain, 0.9 mg ketorolac i.v. was administered to each patient after surgery, because ketorolac given at 0.5–0.9 mg/kg has been shown to be effective in preventing postoperative pain following strabismus surgery.30,31 However, in this present study the paediatric patients who were obviously in pain did not exhibit ED, although it was difficult to exclude the presence of pain in patients with ED. In our study, postoperative pain was managed using fentanyl and there were no significant differences in fentanyl administration between the four groups, or according to the presence of ED within each group. Therefore, postoperative pain was unlikely to have influenced the PAED scores, but one cannot exclude pain as a possible confounder.
This present study also administered midazolam to every patient, because parents were not permitted to enter the operating room, in contrast to previous studies.19,20 Premedication with midazolam has controversial effects on ED.3,27,28 The preoperative anxiety of patients was assessed prior to midazolam premedication, which might have affected the relationship between preoperative anxiety and ED. However, the fact that midazolam was universally administered, and the large size of the study population, is likely to have reduced the likelihood of this being the case.
There were two main limitations in this present study. First, the PAED scores, and scores pertaining to the incidence and degree of ED, were measured by a single individual working in the PACU. As such, the possibility exists that subjective judgements may have acted as a bias. Secondly, patients were not distributed equally among the four surgical groups; because the primary purpose was to investigate the correlation between preoperative anxiety and ED, patients were not enrolled according to the type of surgery to which they were subjected.
In conclusion, preoperative anxiety was not related to ED in preschool-age paediatric patients undergoing strabismus surgery. A higher incidence and degree of ED occurred in patients receiving bilateral strabismus surgery. In turn, a higher incidence and degree of ED occurred in bilateral strabismus surgery patients receiving multiple-muscle corrections, compared with those who received a single-muscle correction. Therefore, concerted efforts toward prevention and management of ED should be made for preschool-age paediatric patients who are subjected to more complex types of strabismus surgery.
Footnotes
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.