
Abstract
Objective
To investigate the relationship between expression of matrix metalloproteinase (MMP)-9 and expression of adenylyl cyclase-associated protein (CAP)-1 in chronic obstructive pulmonary disease (COPD).
Methods
Patients with possible respiratory disease were recruited into the study and divided into a COPD group and a non-COPD group on diagnosis. Pulmonary function tests were performed and serum concentrations of MMP-9 were measured using an enzyme-linked immunosorbent assay. MMP-9 and CAP1 expression were analysed in lung tissue and bronchoalveolar lavage fluid in all available samples using immunohistochemistry and Western blot, respectively. In addition, expression of MMP-9 and CAP1 in vitro was investigated using immunofluorescence. Expression of CAP1 in response to MMP-9 was measured in the human alveolar epithelial cell line HP-AEpiC, using Western blot.
Results
A total of 90 patients were included in the study: 52 were in the COPD group and 38 in the non-COPD group. Serum MMP-9 concentrations were significantly higher in the COPD than in the non-COPD group. MMP-9 serum concentrations were negatively correlated with forced expiratory volume in 1 s (FEV1), FEV1 as a percentage of the normal predicted value and the ratio of FEV1 to forced vital capacity, and were positively correlated with residual volume (RV), total lung capacity (TLC) and RV/TLC values. In lung tissue and bronchoalveolar lavage fluid samples, MMP-9 and CAP1 expression were inversely related. This relationship was confirmed in HP-AEpiC cells. High expression of MMP-9 and low expression of CAP1 was demonstrated in the COPD group compared with the non-COPD group.
Conclusions
This study demonstrated an inverse relationship between CAP1 and MMP-9 expression, and high expression of MMP-9 and low expression of CAP1 in those with COPD compared with the non-COPD group. Overexpression of MMP-9 in lung tissue and its interaction with CAP1 is likely to play a major role in airway obstruction in COPD.
Keywords
Introduction
Chronic obstructive pulmonary disease (COPD) is a major cause of respiratory morbidity and mortality, worldwide. The incidence of the disease is increasing and it has been estimated that by 2020 COPD will be the fourth largest cause of death in the world.1,2 However, the pathogenesis of COPD is unclear.
Chronic obstructive pulmonary disease is an inflammatory disease characterized by extracellular matrix remodelling and collagen deposition. Collagen homeostasis is known to be controlled by matrix metalloproteinases (MMPs) and tissue inhibitors of metalloproteinases (TIMPs).3,4 MMP-9, which is also known as gelatinase B and is 92 kDa in size, is typically activated during injurious conditions, plays various roles in growth, development, inflammation and remodelling, and is produced by different cell types, including airway epithelial cells. 5 MMP-9 has been shown to be associated with airway remodelling, which can impact the dynamic assembly of microfilaments and interfere with the repair of cytoarchitecture, as well as with cell migration.5,6 Some studies have provided evidence that MMP-9 is a biomarker that predicts COPD progression,7,8 but the role of MMP-9 in COPD is largely unknown.
Adenylyl cyclase-associated protein (CAP) is a highly conserved, widely distributed protein that is involved in cytoskeleton remodelling. 9 It consists of two parts, with the N-terminal domain providing a binding site for adenylyl cyclase and the C-terminal domain possessing actin-binding activity, and is activated by nutritional response signals. 9 CAP is diffusely distributed throughout the cytoplasm and is concentrated at the cell membrane and lamellipodia of migrating fibroblasts. 9 Among the subtypes of CAP, CAP1 is an actin monomer-binding protein coded by the CAP1 gene, which was originally cloned from budding yeast and is located downstream of the ras gene. 10 The human homologue of CAP1 was identified in the early 1990s. 11 Both mammalian and yeast CAPs have been shown to interact with actin 12 and to play a role in actin turnover. 13 It has been reported that airway epithelial cells produce CAP1, which has been linked to cell migration and MMP-9 regulation. 14 Given the critical role of actin filament reorganization in cytoplasm and the regulatory role of CAP1 in such reorganization, changes in CAP1 expression may be associated with MMP-9 expression in COPD.
The purposes of the present study were to evaluate the expression of MMP-9 and CAP1 in COPD, and to examine the expression of CAP1 in vitro, in response to MMP-9 in a human alveolar epithelial cell line.
Patients and methods
Patients
Patients with possible respiratory disease referred to the Department of Respiratory Medicine, Tenth People’s Hospital, Tongji University, Shanghai, China, between May 2012 and January 2014 were enrolled in the study. On diagnosis, they were divided into a COPD group, defined according to the Global Initiative for Chronic Obstructive Lung Disease guidelines, 15 and a non-COPD group. Patients diagnosed with lung cancer, pneumonia or asthma were excluded from the study.
All study participants provided written informed consent and the study protocol was approved by the Ethics Committee of the Shanghai Tenth People’s Hospital, Tongji University, Shanghai, China.
Pulmonary function tests
Pulmonary function tests were carried out on all study participants in the morning of examination; patients had not received any medication in the previous 24 h. 16 Forced expiratory volume in 1 s (FEV1), FEV1 as a percentage of the normal predicted value (FEV1%), forced vital capacity (FVC), the FEV1/FVC ratio, residual volume (RV), total lung capacity (TLC) and the RV/TLC ratio were measured before and 30 min after inhalation of 400 µg salbutamol. All tests were performed according to European Respiratory Society guidelines. 17 Airflow limitation was defined as a FEV1/FVC ratio of < 70% and a FEV1 of < 80% of the normal predicted value after inhalation of a bronchodilator. Bronchodilator reversibility was defined as an increase of > 12% or 200 ml, respectively, in either the FEV1 or FVC from the prebronchodilator baseline after inhalation of salbutamol. Patients with bronchodilator reversibility were considered to have asthma rather than COPD and were excluded from the study. Postbronchodilator results from all study participants were used for further analysis.
Serum, bronchoalveolar lavage fluid and lung tissue samples
Blood samples were obtained from all study participants for the measurement of serum MMP-9 levels using an enzyme-linked immunosorbent assay (ELISA). When bronchoscopic examination was required for diagnostic purposes, bronchoalveolar lavage fluid was obtained for the measurement of MMP-9 and CAP1 expression using Western blot. In addition, when lung tissue was obtained on bronchoscopic examination for diagnostic purposes, samples were assessed for the expression of MMP-9 and CAP1 using immunohistochemical analysis.
ELISA analysis of serum MMP-9 concentration
Blood samples (5 ml) were obtained from all study participants and left at room temperature for 30 min. After centrifugation for 15 min at 1000
The total concentration of free and complexed MMP-9 was measured in serum by ELISA using the MMP-9 Biotrak Activity Assay (GE Healthcare, Little Chalfont, UK) according to the manufacturer’s instructions. 18 Absorbance at 450 nm was measured using an ELx800® absorbance microplate reader (BioTek, Winooski, VT, USA). 18 Intra- and interassay coefficients of variation were < 10% and < 15%, respectively. The limits of detection of the assay were 0.08–128 ng/ml.
Western blot analysis of MMP-9 and CAP1 expression
After collection, bronchoalveolar lavage samples were immediately homogenized in homogenization buffer containing 1 M Tris–HCl (pH 7.5), 1% Triton X™-100, 1% Nonidet™ P-40, 10% sodium dodecyl sulphate (SDS), 0.5% sodium deoxycholate, 0.5 M ethylenediaminetetra-acetic acid, 10 mg/ml leupeptin, 10 mg/ml aprotinin and 1 mM phenylmethane sulphonyl fluoride, then centrifuged at 10 000 g for 30 min at 4℃ and the supernatant collected. The resulting proteins were mixed with two times loading buffer consisting of 100 mmol/l Tris–HCl (pH 6.8), 200 mmol/l dithiothreitol, 4% SDS, 20% glycerol and 0.2% bromophenol blue, heated in boiling water for 5–10 min and then cooled in ice. Total protein concentrations were determined using a Bio-Rad protein assay (Bio-Rad Laboratories, Hercules, CA, USA), according to the manufacturer’s instructions. Samples containing 30 µg of protein were loaded onto 10% polyacrylamide-SDS gels, separated by electrophoresis and blotted onto polyvinylidene fluoride membranes using the semidry transfer method. Membranes were blocked with 5% non-fat dry milk (Bio-Rad Laboratories) in Tris-buffered saline (20 mM Tris/HCl, pH 7.6, 137 mM NaCl) containing 0.1% Tween-20 for 1 h. Anti-CAP1 (1 : 800), anti-MMP-9 (1 : 800) and antiactin (1 : 1500) antibodies (Sigma, St Louis, MO, USA) were then hybridized to the membranes overnight at 4℃. After washing three times for 8 min with 1000 ml 1 × PBS with 1 ml 0.1% Tween-20, membranes were incubated with horseradish peroxidise-conjugated secondary goat antimouse antibody (1 : 1500) (Jackson ImmunoResearch, West Grove, PA, USA) at room temperature for 90 min. After washing three times for 8 min with 1000 ml 1 × PBS with 1 ml 0.1% Tween-20, proteins were visualized by exposure to X-radiography films using the ECL Western Blotting System (GE Healthcare).
Immunohistochemical analysis of MMP-9 and CAP1 expression
Lung tissue samples were fixed in formalin for 24 h, washed in water, dehydrated in graded ethanol, dewaxed in xylene and embedded in paraffin wax. Sections 4 µm in thickness were then dewaxed in xylene and rehydrated in graded ethanol for immunohistochemical analysis. Cells from the human alveolar epithelial cell line HP-AEpiC (ATCC, Manassas, VA, USA) were used as positive controls. Endogenous peroxidase activity was blocked by soaking in 0.3% hydrogen peroxide. The sections were then incubated in 10 mmol/l citrate buffer (pH 6.0) and heated to 121℃ for 20 min, for antigen retrieval. After washing three times for 5 min in PBS (pH 7.2), sections were blocked with 10% goat serum for 1 h at room temperature. They were then incubated overnight at 4℃ with mouse anti-CAP1 monoclonal antibody (1 : 500; provided by Dr Zhou, University of Pennsylvania School of Medicine, Philadelphia, USA) or mouse anti-MMP-9 antibody (1 : 150) (Sigma). Slides were processed using the peroxidase–antiperoxidase method (Dako, Hamburg, Germany) according to the manufacturer’s instructions. After rinsing with PBS, the peroxidase reaction was visualized by incubating the sections with diaminobenzidine tetrahydrochloride in 0.05 mol/l Tris buffer (pH 7.6) containing 0.03% hydrogen peroxide. After rinsing in water, sections were counterstained with haematoxylin, dehydrated, cover-slipped and examined under a light microscope. At least 10 high-power fields were randomly chosen and at least 400 cells/field were counted for each sample.
Staining results were assessed independently by two pathologists who were blind to the source of the specimen. The immunoreactive intensity in the specimens was graded by comparing it to the staining intensity of endothelial cells in the positive control group; each specimen was given a score of 0 (negative; no staining), 1 (weak; weaker than epithelial cells), 2 (moderate; same as epithelial cells) or 3 (strong; stronger than epithelial cells). A staining score of 0 or 1 was considered to indicate low expression of CAP1, whereas a score of 2 or 3 was considered to indicate high expression. At least three specimens were examined from each study participant.
Immunofluorescence analysis of MMP-9 and CAP1 expression
The HP-AEpiC cells were grown to confluence on coverslips or 8-well Nunc™ chamber slides (Thermo Scientific, Waltham, MA, USA). After incubation for 24 h, the cells were rinsed twice with PBS, fixed in 4% paraformaldehyde/PBS for 15 min, and blocked with 2% dry milk/PBS/0.1% Triton X™ for 45 min. Cells were probed with MMP-9 mouse monoclonal antibody (1 : 150) (Oncogene, Cambridge, MA, USA) and CAP1 rabbit polyclonal antibody (1 : 150) (Santa Cruz Biotechnology, Santa Cruz, CA, USA) in 2% bovine serum albumin/PBS/Triton X™ for 1 h at 37℃, washed twice with PBS, and then incubated with secondary antibodies Alexa Fluor 568 goat antimouse immunoglobulin G antibody (1 : 500) (Molecular Probes, Thermo Scientific) and goat antirabbit immunoglobulin G antibody (1 : 500) (Jackson ImmunoResearch) in 2% bovine serum albumin/PBS for 1 h at 37℃. After two washes with PBS, the nuclei were stained with Sytox® green (Life Technologies, Grand Island, NY, USA) (1 : 10 000 in PBS) for 5 min. After a final wash in PBS, slides were imaged using an Olympus BX50 confocal laser scanning microscope with LaserSharp2000 software (Bio-Rad Laboratories).
CAP1 expression in response to MMP-9 in vitro
The HP-AEpiC cells were cultured in RPMI 1640 medium (BioWhittaker, Verviers, Belgium) supplemented with 10% fetal calf serum (Invitrogen, Carlsbad, CA, USA). Experiments were performed in 6-, 12 - or 24-well plates (Corning Inc., Corning, NY, USA). Samples of 10 000 HP-AEpiC cells were incubated with recombinant human MMP-9 (r-MMP-9) (Abcam, Cambridge, MA, USA) at a concentration of 4 nM for 1.5 h, 4.5 h, 12 h or 24 h. In addition, HP-AEpiC cells were incubated with r-MMP-9 at concentrations of 0.2 nM, 0.8 nM, 4 nM, 20 nM or 100 nM for 4.5 h.
The resulting samples were homogenized and expression of CAP1 was then measured in aliquots containing 30 µg of protein using Western blotting, as described above.
Statistical analyses
Results were expressed as mean ± SD. The nonparametric Mann–Whitney U-test or the χ2-test were used to assess differences between the groups. Spearman’s rank correlation coefficient was used to assess correlations between data sets. A P-value < 0.05 was considered to be statistically significant. All statistical analyses were performed using SPSS® version 20.0 (IBM, Somers, NY, USA).
Results
A total of 90 patients with possible respiratory disease were recruited to the study. Of these, 52 were diagnosed with COPD; the remaining 38 had other respiratory diseases (including foreign bodies in the trachea and bronchi [n = 5]), miscellaneous disorders requiring bronchoscopy (n = 7) or bronchoalveolar lavage (n = 15) to make a definite diagnosis, or were found to be normal (n = 11).
Pulmonary function tests
Pulmonary function test results in patients with chronic obstructive pulmonary disease (COPD) group and those not diagnosed with COPD (non-COPD group).

Data presented as mean ± SD.
FEV1, forced expiratory volume in 1 s; FEV1%, FEV1 as a percentage of the normal predicted value; FVC, forced vital capacity; RV, residual volume; TLC, total lung capacity.
Mann–Whitney U-test.
Serum MMP-9 levels and correlation with pulmonary function test results
Serum samples were available from all study participants. The serum concentration of MMP-9 was significantly higher in the COPD group (3.02 ± 0.77 ng/ml) than in the non-COPD group (0.96 ± 0.48 ng/ml) (Z = −8.030, P < 0.01).
Relationships between serum MMP-9 levels and pulmonary function test results were analysed. Negative correlations were found between MMP-9 levels and FEV1, FEV1% and FEV1/FVC (P < 0.01 for all) (Figure 1). In addition, the serum level of MMP-9 was also positively correlated with RV, TLC and RV/TLC values (P < 0.01 for all) (Figure 1).
Correlations between the serum concentration of matrix metalloproteinase (MMP)-9 and pulmonary function test results in both patients with orthose with and without chronic obstructive pulmonary disease (COPD) (n = 90) using Spearman’s rank test; the line corresponds to the fitted regression equation. (A) Serum MMP-9 versus forced expiratory volume in 1 s (FEV1); (B) serum MMP-9 versus FEV1 as a percentage of the normal predicted value (FEV1%); (C) serum MMP-9 versus FEV1 as a percentage of forced vital capacity (FEV1/FVC%); (D) serum MMP-9 versus residual volume (RV); (E) serum MMP-9 versus total lung capacity (TLC); (F) serum MMP-9 versus RV/TLC.
MMP-9 and CAP1 expression in bronchoalveolar lavage fluid
Bronchoalveolar lavage fluid samples available from 30 patients (20 in the COPD group and 10 in the non-COPD group) were analysed for MMP-9 and CAP1 expression using Western blot. Samples from the COPD group highly expressed MMP-9 protein compared with those from the non-COPD group (Figure 2). In contrast, the expression of CAP1 was higher in the non-COPD group than in the COPD group (Figure 2).
Representative Western blots of matrix metalloproteinase (MMP)-9 and adenylyl cyclase-associated protein 1 (CAP1) expression in bronchoalveolar lavage fluid samples from the chronic obstructive pulmonary disease (COPD) group and the non-COPD group.
MMP-9 and CAP1 expression in lung tissue samples
Lung tissue samples available from 57 patients (35 in the COPD group and 22 in the non-COPD group) were analysed for MMP-9 and CAP1 expression by immunohistochemistry. MMP-9 expression was higher and CAP1 expression was lower in lung tissue from the COPD group compared with the non-COPD group (Figure 3).
Expression of matrix metalloproteinase (MMP)-9 and adenylyl cyclase-associated protein 1 (CAP1) in lung tissue samples: (A) MMP-9 expression, chronic obstructive pulmonary disease (COPD) group; (B) CAP1 expression, COPD group; (C) MMP-9 expression, non-COPD group; (D) CAP1 expression, non-COPD group. The colour version of this figure is available at: http://imr.sagepub.com.
Expression of matrix metalloproteinase (MMP)-9 and adenylyl cyclase-associated protein 1 (CAP1) in lung tissue samples from patients with chronic obstructive pulmonary disease (COPD) group and those not diagnosed with COPD (non-COPD group).
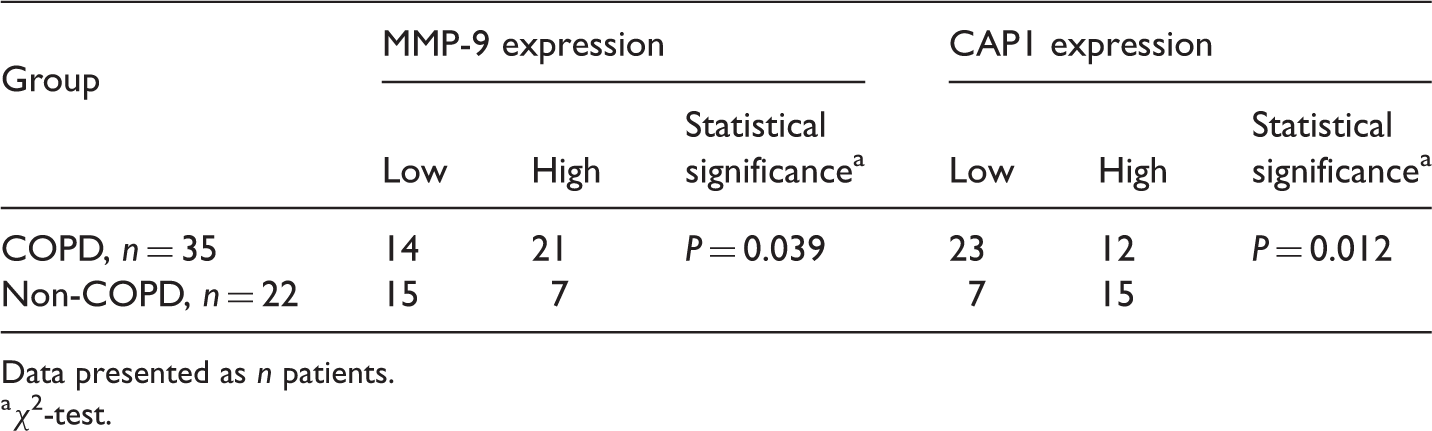
Data presented as n patients.
χ2-test.
Correlations between MMP-9 and CAP1 expression and pulmonary function tests
Pulmonary function test results according to expression of matrix metalloproteinase (MMP)-9 in lung tissue samples from patients with chronic obstructive pulmonary disease (COPD group; n = 35) and those not diagnosed with COPD (non-COPD group; n = 22).

Data presented as mean ± SD.
FEV1, forced expiratory volume in 1 s; FEV1%, FEV1 as a percentage of the normal predicted value; FVC, forced vital capacity.
Mann–Whitney U-test.
Pulmonary function test results according to expression of adenylyl cyclase-associated protein 1 (CAP1) in lung tissue samples from patients with chronic obstructive pulmonary disease (COPD group; n = 35) and those not diagnosed with COPD (non-COPD group; n = 22).

Data presented as mean ± SD.
FEV1, forced expiratory volume in 1 s; FEV1%, FEV1 as a percentage of the normal predicted value; FVC, forced vital capacity.
Mann–Whitney U-test.
Correlation between MMP-9 and CAP1 expression
Analysis of correlation between the expression of adenylyl cyclase-associated protein 1 (CAP1) and the expression of matrix metalloproteinase (MMP)-9 in lung tissue samples from patients with chronic obstructive pulmonary disease (COPD group; n = 35) and those not diagnosed with COPD (non-COPD group; n = 22).

Spearman’s rank correlation test.
MMP-9 and CAP1 expression in HP-AEpiC cells
On immunofluorescence analysis of HP-AEpiC cells, CAP1 and MMP-9 were both detected mainly in the perinuclear cytoplasm (Figure 4A and Figure 4B, respectively). On merged images, CAP1 and MMP-9 were co-localized to the leading edge of the lamellipodium (Figure 4C).
Subcellular localization of adenylyl cyclase-associated protein 1 (CAP1) and matrix metalloproteinase (MMP)-9 expression detected using immunofluoresence: (A) HP-AEpiC cells probed with anti-CAP1 antibody; (B) HP-AEpiC cells probed with anti-MMP-9 antibody; (C) merged images. The colour version of this figure is available at: http://imr.sagepub.com.
CAP1 expression in response to r-MMP-9 in vitro
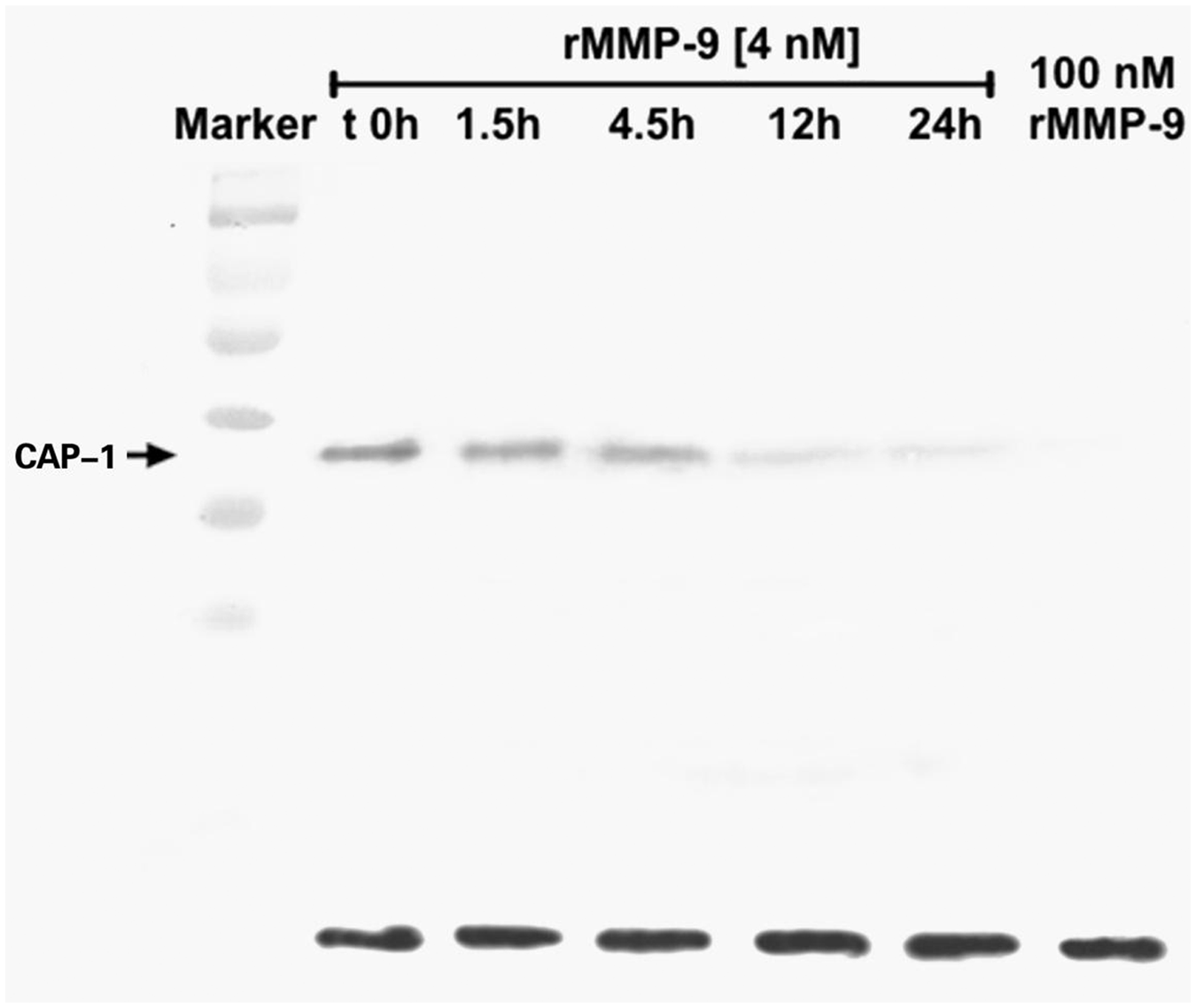
Western blot analysis of CAP1 expression in HP-AEpiC cells treated with r-MMP-9 showed that incubation for 4.5 h with increasing concentrations of r-MMP-9 was associated with decreasing expression of CAP1 (Figure 5). In addition, incubation of HP-AEpiC cells treated with r-MMP-9 at a concentration of 4 nM for increasing periods of time was again associated with decreasing expression of CAP1 (Figure 6).
Representative Western blots of adenylyl cyclase-associated protein 1 (CAP1) expression following incubation for 4.5 h in the presence of various concentrations of recombinant human matrix metalloproteinase-9 (rMMP-9). Representative Western blots of adenylyl cyclase-associated protein 1 (CAP1) expression following incubation for different times in the presence of recombinant human matrix metalloproteinase-9 (rMMP-9) at a concentration of 4 nM.
Discussion
The results of the present study demonstrated high expression of MMP-9 and low expression of CAP1 in patients with COPD. This overexpression of MMP-9 in lung tissue in COPD may contribute to the destruction and reconstitution of the bronchial and/or alveolar wall through interaction with CAP1, and is likely to play a major role in airway obstruction.
The airway epithelium provides a protective barrier against inhaled environmental toxins and micro-organisms, and epithelial injury initiates a number of processes designed to restore the integrity of the barrier, including activation of MMPs, such as MMP-9. 6 Overexpression of MMP-9 in the lung results in the accumulation of inflammatory cells, which release various inflammatory factors that could damage the normal lung structure. 19 In addition, increased expression of MMP-9 in lung tissue may contribute to the destruction and reconstitution of the bronchial or/and alveolar wall, which is likely to play a major role in airway obstruction. 20 MMPs in general, and MMP-9 in particular, cleave extracellular structural (such as gelatins) and functional substrates (such as chemokines). 21
It has been shown that CAP1 plays a key role in cytoskeleton remodelling and in the migration of alveolar cells. 14 As CAP1 is the biological target of MMP-9, it has been hypothesized that CAP1 would bind to an MMP-9 exosite. 14 CAP1 has been shown to be released on cytolysis into the extracellular milieu in vitro, and thus becomes a highly efficient MMP-9 substrate. 14
The aim of the present study was to investigate the relationship between MMP-9 and CAP1 expression in patients with COPD compared with a non-COPD group. The study demonstrated a significant correlation between high expression of MMP-9 and low expression of CAP1. This was confirmed using Western blot and immunohistochemistry in bronchoalveolar lavage fluid and lung tissue samples. In addition, expression of MMP-9 in serum was shown to be increased in the COPD group compared with the non-COPD group. A potential weakness of the study was that expression of MMP-9 was not analysed in sputum as comprehensively as it was in serum. The mechanism of the interaction between MMP-9 and CAP1 in COPD requires further investigation.
In conclusion, the present study findings show a significant inverse relationship between the expression of MMP-9 and the expression of CAP1 in COPD. Overexpression of MMP-9 in lung tissue and its interaction with CAP1 may contribute to the destruction and reconstitution of the bronchial and/or alveolar wall and is likely to play a major role in airway obstruction, in COPD.
Footnotes
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This study was funded by the National Natural Science Foundation of China (no. 81172229, 81100018).