
Abstract
We report a case of a 43-year-old man with early stage (stage 1) avascular necrosis (AVN) of the femoral head treated with adipose tissue-derived stem cells (ASCs) and platelet-rich plasma (PRP). ASC-containing stromal vascular fraction was mixed with PRP and hyaluronic acid. This mixture was then injected into the diseased hip under ultrasound guidance. The affected hip was reinjected weekly with additional PRP for 4 weeks. The patient was followed-up with sequential magnetic resonance imaging (MRI) scans at 3, 18, and 21 months after treatment, together with Visual Analogue Scale (VAS) Walking Index, Functional Rating Index, Harris Hip Score, and Range of Motion (ROM) assessments. The patient’s severe hip pain was considerably improved at 3 months after treatment, with pain scores, ROM and MRI showing near complete resolution of AVN. Pain scores, ROM and MRI at 18 and 21 months after treatment indicated complete resolution of AVN. This case represents the first evidence of complete resolution of early stage AVN of the hip following treatment with ASCs/PRP.
Keywords
Introduction
Avascular necrosis (AVN, also known as osteonecrosis) is defined as cellular death of bone components due to interruption of the blood supply, and occurs most commonly in the hip.1,2 As a result of necrosis, bone structure collapses, leading to bone destruction, pain and loss of joint function.
The worldwide prevalence of AVN of the femoral head is unknown. There are an estimated 15 000–20 000 new cases in the US each year 3 and 2 500–3 300 cases in Japan. 4
The exact causal mechanism of the decreased blood circulation to the femoral head is unclear, but is highly correlated with trauma and alcohol or steroid use.5 In addition, venous occlusion, vessel wall injury, fat embolism, microfracture from trabecular insufficiency, intraosseous hypertension, intraosseous hemorrhage, vasculitis and intravascular coagulation are associated with AVN.6–12
Pathologically, AVN is characterized by empty lacunae in the osseous matrix and necrotic bone marrow of trabecular interstices. 13 The region of necrosis is surrounded by reparative tissues.13,14 Unfortunately, the healing process that has formed the reparative tissue does not overcome the necrotic process of the femoral head, resulting in further necrosis of the bone.15,16
Total hip replacement (THR) surgery is the only definitive cure for AVN of the hip, but THR surgery has several drawbacks. Hip implants usually fail after approximately 15 years17,18 and the surgery itself requires a prolonged period of postoperative recovery and physical therapy.
Several clinical studies have shown good results in treating hip AVN with bone marrow-derived mesenchymal stem cells (MSCs) or adipose tissue-derived stem cells (ASCs),5,19–24 but none of these reports showed complete resolution of AVN. In this report, we describe the first complete resolution of AVN of the hip by percutaneous injection of autologous ASCs along with platelet-rich plasma (PRP).
Case report
A 43-year-old Korean man with history of moderate alcohol use and smoking but no history of trauma presented to Stems Medical Clinic (Seoul, Republic of Korea) on 22 March 2012 with a chief complaint of right hip pain for 3 months. The patient was initially seen by an orthopaedic surgeon who ordered magnetic resonance imaging (MRI) and X-radiographs of the hip. X-radiography findings were normal, but MRI revealed stage 1 AVN of the right femoral head (Ficat classification system
25
). The Harris Hip Score (HHS
26
) pain subscale was 8, function subscale was 14, deformity subscale was 0, and motion subscale was 3 (total score 25/100 (Figure 1(A)). Pain scores (visual analogue scale [VAS]) were 6 at rest and 8 when standing and walking (VAS Walking Index Figure 1(A)). The patient’s functional rating index (FRI) score was 14 (Figure 1(A)) and range of motion (ROM) on physical therapy was limited (Figure 1(B) and (C)). Pain scores and ROM were measured as previously described.27,28 MRI of the affected hip showed diffuse T1 low signal intensity (Figures 2(A) to (D) and 4(A) to (D)) and T2 high signal intensity (Figures 3(A) to (D) and 5(A) to (D)) that were consistent with early stage AVN. The patient was given oral non-steroidal anti-inflammatory drugs (NSAIDs) along with acetaminophens, but this treatment did not improve the patient’s pain. The patient was reluctant to undergo THR due to known drawbacks and no other surgical treatment was offered. Being aware of the lack of noninvasive curative therapy for AVN, the patient elected to undergo autologous, non-cultured ASCs/PRP-based treatment for possible resolution of AVN.
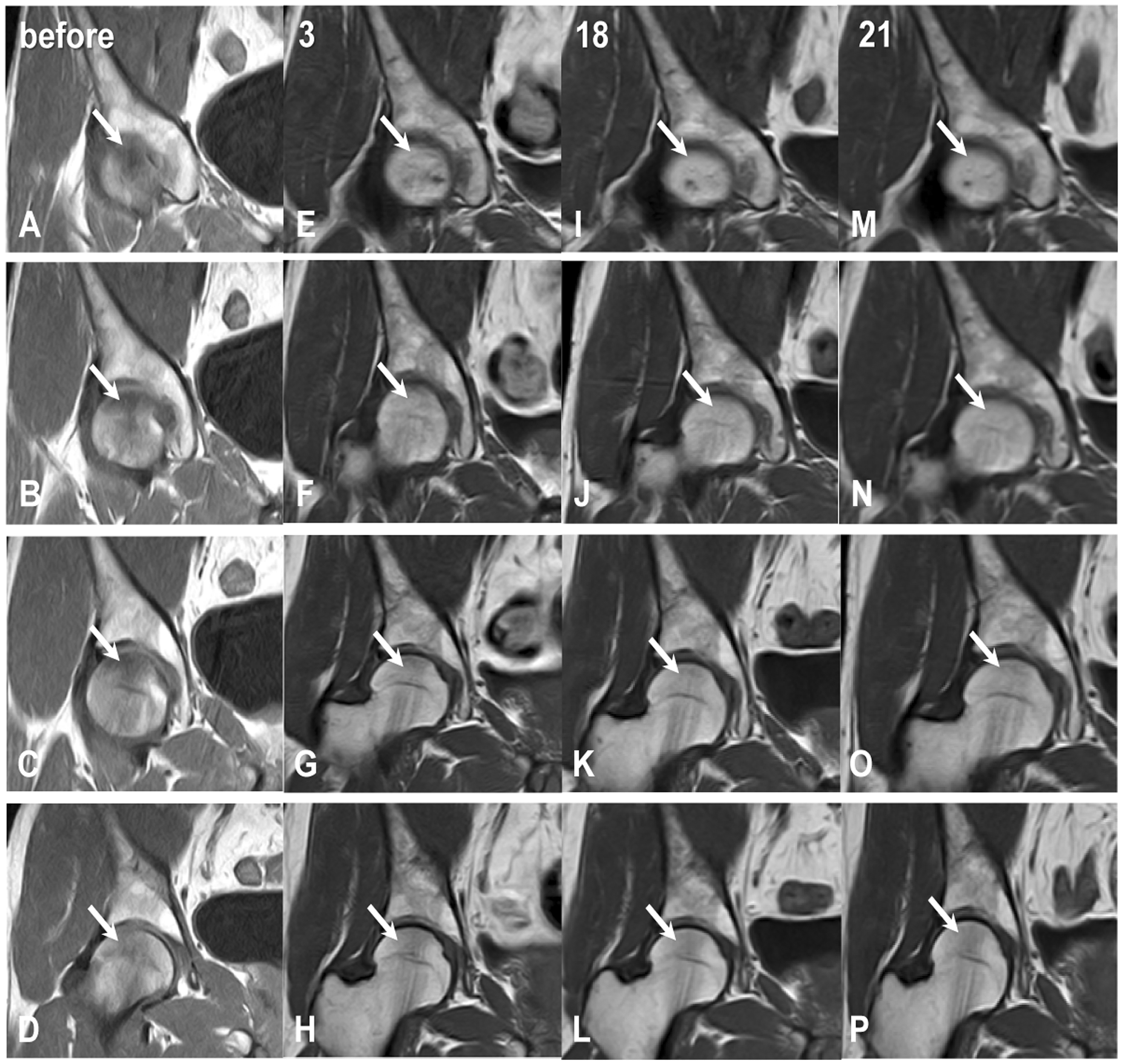
Pain (visual analogue scale [VAS]), Harris hip score and range of motion data for a 43-year-old male patient with avascular necrosis of the femoral head, before and after treatment with adipose tissue-derived stem cells and platelet-rich plasma. Data were collected before treatment and at 3, 18 and 21 months after treatment. Data presented as mean ± SD of 3 measurements. T1-weighted sequential axial magnetic resonance images of the right hip of a 43-year-old male patient with avascular necrosis (AVN) of the femoral head, before and after treatment with adipose tissue-derived stem cells and platelet-rich plasma. (A–D) Pretreatment scans show diffuse T1 low signal intensity (arrows) consistent with early stage AVN. (E–H) At 3 months after treatment, scans show dramatically decreased diffuse T1 low signal intensity (arrows). (I–L) At 18 months, and (M–P) 21 months after treatment there is a complete absence of diffuse T1 low signal intensity (arrows), indicating the complete resolution of AVN. Fat-suppressed T2-weighted sequential axial magnetic resonance images of the right hip of a 43-year-old male patient with avascular necrosis (AVN) of the femoral head, before and after treatment with adipose tissue-derived stem cells and platelet-rich plasma. (A–D) Pretreatment scans show diffuse T2 high signal intensity (arrows) consistent with early stage AVN. (E–H) At 3 months after treatment, scans show dramatically decreased diffuse T2 high signal intensity (arrows). (I–L) At 18 months, and (M–P) 21 months after treatment there is a complete absence of diffuse T2 high signal intensity (arrows), indicating the complete resolution of AVN. T1-weighted sequential coronal magnetic resonance images of the right hip of a 43-year-old male patient with avascular necrosis (AVN) of the femoral head, before and after treatment with adipose tissue-derived stem cells and platelet-rich plasma. (A–D) Pretreatment scans show diffuse T1 low signal intensity (arrows) consistent with early stage AVN. (E–H) At 3 months after treatment, scans show dramatically decreased diffuse T1 low signal intensity (arrows). (I–L) At 18 months, and (M–P) 21 months after treatment there is a complete absence of diffuse T1 low signal intensity (arrows), indicating the complete resolution of AVN. Fat-suppressed T2-weighted sequential coronal magnetic resonance images of the right hip of a 43-year-old male patient with avascular necrosis (AVN) of the femoral head, before and after treatment with adipose tissue-derived stem cells and platelet-rich plasma. (A–D) Pretreatment scans show diffuse T2 high signal intensity (arrows) consistent with early stage AVN. (E–H) At 3 months after treatment, scans show dramatically decreased diffuse T2 high signal intensity (arrows). (I–L) At 18 months, and (M–P) 21 months after treatment there is a complete absence of diffuse T2 high signal intensity (arrows), indicating the complete resolution of AVN.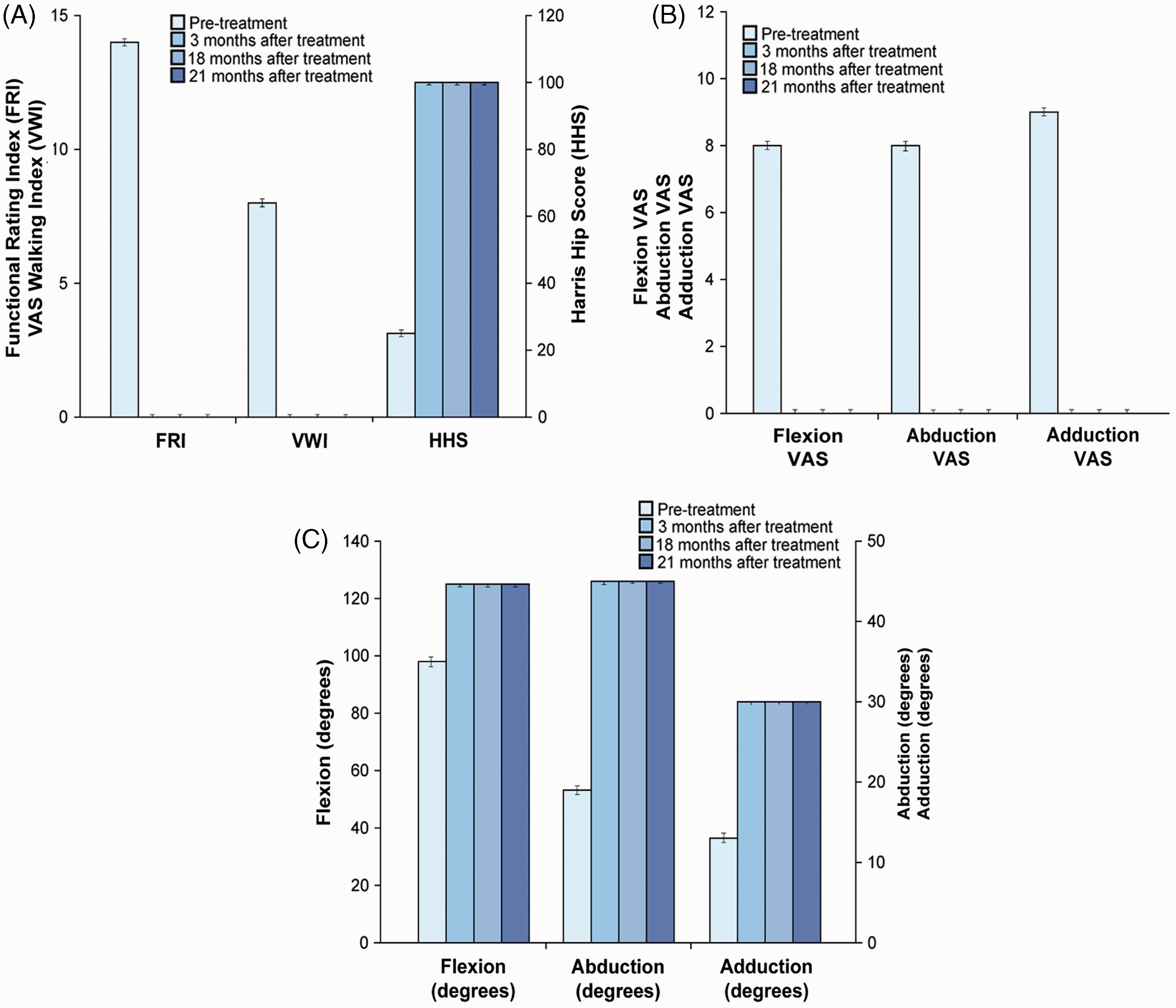



In June 2009, the Korean Food and Drug Administration (KFDA) allowed the use of non-cultured ASCs for autologous cell transplantation when obtained and processed within the same medical facility, employing minimal processing and manipulation, 29 allowing the use of adipose tissue as a source of ASCs. At that time, informed consent was obtained from the patient. Approval and consent to report single cases were waived by Myongji University Institutional Review Board committee (HSC) for case reports. This study is in compliance with the Declaration of Helsinki and regulation guidelines of the KFDA. According to Korean law, this study does not require approval by ethical and scientific committees. 29
Treatment
The patient was prevented from taking steroids, aspirin, NSAIDs and oriental herb medications for 1 week prior to the procedure. In the operating room, approximately 50 g of packed adipose tissue was obtained by liposuction of the subcutaneous part of the lower abdominal area of the patient using sterile techniques.23,30 ASCs were extracted as previously described, using 0.07% collagenase Type 1 and centrifugation.22,30,31 The total volume of solution containing ASCs was 8 ml. While preparing the ASCs, 30 ml of autologous blood was drawn and mixed with 2.5 ml citrate dextrose solution. 22 Following centrifugation of blood, 4 m PRP with buffy coat was obtained. To this mixture, 2 ml of 0.5% (w/v) hyaluronic acid was added as a scaffold. 32 After cleaning with betadine and sterile draping, the injection site of the right hip was anaesthetized with 2% lidocaine. Then, the ASCs/PRP mixture (14 ml) was injected into the femoral head anteriorly, using a 15-gauge, 3 1/2 inch bone aspiration needle under ultrasound guidance. The patient returned to the clinic for PRP injections every week for 4 weeks, using a 22-gauge 3 1/2 inch needle under ultrasound guidance.
The inclusion criteria, exclusion criteria and outcome endpoints for stem cell transplantation are as follows. Inclusion criteria: MRI evidence of AVN of the hip; orthopedic evaluation determined to be negative candidacy for a unipolar or bipolar hip prosthesis; males or females; age under 60; unwillingness to proceed with hip prosthesis; failure of conservative management; and ongoing disabling pain. Exclusion criteria: active inflammatory or connective tissue disease thought to impact pain condition (i.e., lupus, rheumatoid arthritis, fibromyalgia); active endocrine disorder that might impact pain condition (i.e., hypothyroidism, diabetes); active neurologic disorder that might impact pain condition (i.e., peripheral neuropathy, multiple sclerosis); active cardiac disease; and active pulmonary disease requiring medication usage. Outcome endpoints (obtained after 3 months, 18 months, and 21 months): pre- and post-treatment HHS, VWI, FRI, ROM, and MRI.
The patient reported a reduction in hip pain within 2 weeks following the ASCs/PRP injection. At the 3-month follow-up appointment the patient reported complete resolution of symptoms, based on pain scores (VWI, 0; FRI, 0; HHS, 100) and ROM (Flexion VAS, 0; Flexion, 125°; Abduction, VAS 0; Abduction, 45°; Adduction VAS, 0; Adduction, 30°) (Figure 1(A) to (C)). MRI findings at month 3 showed dramatically decreased diffuse T1 low signal intensity (Figures 2(E) to (H) and 4(E) to (H)) and T2 high signal intensity (Figures 3(E) to (H) and 5(E) to (H)).
After 18 months, the patient returned to the clinic for follow-up. At this time, VWI and FRI scores were 0, HHS score was 100 (Figure 1(A)) and ROM was normal (Figure 1(B) and (C)). Repeat MRI showed a total absence of diffuse T1 low signal intensity (Figures 2(I) to (L) and 4(I) to (L)) and T2 high signal intensity (Figures 3(I) to (L) and 5(I) to (L)).
The patient was followed-up again at 21 months, and VWI and FRI scores were 0, HHS score was 100 (Figure 1(A)) and ROM was normal (Figure 1(B) and (C)). The patient reported no hip pain, and symptoms were completely resolved. MRI showed no sign of T1 low signal intensity (Figures 2(M) to (P) and 4(M) to (P)) or T2 high signal intensity (Figures 3(M) to (P) and 5(M) to (P)), indicating the complete resolution of AVN.
Discussion
Several clinical studies have shown good, but not curative, results for bone marrow transfer in the treatment of AVN of the hip.5,19–24 We report the first case of complete resolution of early stage AVN of the hip by percutaneous injection of autologous ASCs/PRP. The difference in outcome between our case and others19–21,24 may be due to several factors, including the number of MSCs injected into the hip. Lipoaspirate (liposuctioned adipose tissue) includes many different types of cells including red blood cells, fibroblasts, endothelial cells, smooth muscle cells, pericytes and preadipocytes that have yet to adhere to a tissue culture substrate. 33 Lipoaspirate-derived adipose tissue can yield approximately 2 × 106 cells/g, with 10% thought to be ASCs (around 200 000/g). This is considerably higher than the number of MSCs in bone marrow transfers (6 000–60 000/g).33,34
An alternative reason for the complete resolution of AVN in this case report may be the number of PRP doses injected. PRP contains a high concentration of autologous growth factors, including transforming growth factor-β (TGF-β), insulin-like growth factor (IGF), fibroblast growth factor (FGF) and platelet-derived growth factor (PDGF),35,36 and is used to provide multiple potentially necessary factors for ASCs to grow and differentiate into bone.37–39 In AVN, the region of necrosis is usually surrounded by reparative tissues, including neovasculature and bone formation.13,14 The large numbers of MSCs and concentrations of growth factors injected in the present case may have allowed the reparative process to overcome the necrotic process.
The third reason for the complete resolution in this case may be the fact that AVN was at an early stage (stage 1). In other studies, patients treated with ASCs/PRP had more advanced stages of AVN (stage 3 or 4).5,22,23
Magnetic resonance imaging was chosen for diagnosis and follow-up in the present case because it has 88% sensitivity, 100% specificity and 94% accuracy for detecting AVN of the hip. 40 Based on MRI findings, the patient was found to have AVN of the right hip, and no biopsy of the lesion was performed. Although it is likely that the diagnosis of AVN is correct in this case, the true nature of the disease cannot be ascertained without a biopsy. Likewise, post-ASCs/PRP-treatment MRIs could show only a high probability of bone-like tissue regeneration. Further, with resolution of the hip pain, the patient was reluctant to undergo a biopsy procedure to ascertain the true nature of the bone-like tissue. The T1 sequence provided information regarding bony anatomical lesion, size, and location, and the T2 sequence with fat suppression indicated the extent of bone inflammation and edema. The differences in signal changes between pre- and post-treatment MRIs can also be normalized to the surrounding acetabulum of the hip. In the present case, the significant MRI signal changes were apparent in both the T1 and T2 views of the femoral head before and after ASCs/PRP treatment. These significant signal changes could be translated into probable, persistent, regeneration of bone lasting at least 21 months. Again, without the biopsy, the true nature of the newly formed tissue could not be clearly determined, but based on comparison with surrounding acetabulum, the tissue was assumed to be hydroxyapatite in nature.
Studies with a larger number of cases and possibly randomized controlled trials are required to determine whether this case report has clinical merit. It is possible that this simple, minimally invasive procedure with ASCs/PRP may hold a great promise for patients with AVN of the femoral head.
Conclusion
This case report demonstrates the first evidence of complete resolution of AVN of the hip following ASCs/PRP treatment. The patient was fortunate to have early diagnosis of AVN of the hip. Compared with studies using bone marrow transplant or ASCs, this case suggests that treatment with a large number of ASCs together with PRP may help young individuals if the disease is detected in the early stage.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received funding from the 2013 Research Fund of Myongji University. This funding source had no role in the writing of the report or the decision to submit it for publication.