
Abstract
Objective
To investigate emergence times with different fresh gas flow rates, following desflurane anaesthesia.
Methods
Patients undergoing surgery with desflurane anaesthesia were randomly assigned to receive fresh gas flow rates of 100% oxygen during emergence of 2 l/min (group D2), 4 l/min (group D4) or 6 l/min (group D6). Time to eye opening, spontaneous movement and extubation (emergence time) were assessed after desflurane discontinuation. The end-tidal concentration of desflurane and bispectral index were recorded at each of these timepoints.
Results
A total of 105 patients were included in the study, with 35 in each of the three groups. Mean times to extubation were 17.6 min, 9.9 min and 9.1 min in groups D2, D4 and D6, respectively. Times to eye opening, spontaneous movement and extubation in group D2 were significantly longer than in groups D4 and D6.
Conclusions
These results suggest that there is the potential to predict emergence time based on fresh gas flow rate following desflurane anaesthesia. It should therefore be possible to use a low-flow technique during the emergence period, in addition to the maintenance period, without delaying recovery if the inhaled anaesthetic is stopped at the predicted time before the end of surgery.
Introduction
Reducing the fresh gas flow rate during anaesthesia could reduce both costs and the emission of environmental contaminants. The use of ‘low-flow’ anaesthesia during induction is problematic, because initial delivery of the anaesthetic gas to the lungs and the brain must be rapid. 1 However, low-flow techniques have been introduced successfully during the maintenance of anaesthesia, and have had substantial economic benefits.2–7 As a result, the use of low flow rates (2 l/min or below) has increased. 8 To achieve fast recovery of consciousness, ventilation with high flow rates of oxygen (5 l/min or more) during the emergence phase is common. 9 However, the administration of inhaled anaesthetics is generally continued until the surgery is complete.
Despite the potential economic and environmental advantages of terminating the administration of inhaled anaesthetics early during emergence,1,10 no study to date has investigated the time to emergence in this context or evaluated the economic benefits of early cessation of inhaled anaesthesia. In low-flow anaesthesia, the alveolar concentration of inhaled anaesthetics changes very slowly; therefore, after their administration is terminated, their concentration decreases only gradually. The consumption of inhaled anaesthetics could theoretically be reduced by stopping their administration at a calculated point before the end of the surgery, with the patient remaining under anaesthesia. The aim of the present study was to investigate the emergence time after the termination of desflurane using different fresh gas flow rates.
Patients and methods
Patients
Patients aged 18–64 years and classified as American Society of Anesthesiologists class I or II, scheduled to undergo elective surgery under general anaesthesia using desflurane in the Department of Anaesthesia and Pain Medicine, Hanyang University School Hospital, Seoul, Republic of Korea, between October 2012 and April 2013 were recruited to the study. Exclusion criteria included cardiovascular disease with a left ventricular ejection fraction of <40%, surgery time of >5 h, pregnancy or lactation, tonsillectomy, nasal surgery, dental surgery, surgery in a prone or lateral position, heart surgery and lung surgery.
The methods and aims of the study were explained to the patients, all of whom provided written informed consent. The study protocol was approved by the Institutional Review Board of Hanyang University Seoul Hospital (approval number 2012-07-012-005, approval date September 25, 2012) and was registered in a public trial registry at the Clinical Research Information Service (http://cris.nih.go.kr/cris/index.jsp) (KCT0000603).
General anaesthesia conditions
All patients fasted and did not take any analgesics or sedatives for 12 h before surgery. In the operating room, the patient’s vital signs were monitored using electrocardiography, a noninvasive blood pressure monitor and pulse oximetry. The patient’s level of consciousness was monitored using a bispectral index (BIS) sensor attached to the forehead and connected to a BIS monitor (2000A, Aspect Medical Systems, Norwood, MA, USA).
Anaesthesia was induced by an intravenous injection of propofol (1.5 mg/kg), followed by rocuronium (0.6 mg/kg) to facilitate intubation and remifentanil (0.25 µg/kg) as an analgesic. During the operation, anaesthesia was maintained with desflurane in oxygen (inspiratory fraction 0.5 at a flow rate of 2 l/min) in the presence of remifentanil, using a Dräger Cato anaesthetic machine (Dräger, Lubeck, Germany). Desflurane administration was maintained to give an end-tidal concentration of 5–6 vol% until termination of inhaled anaesthesia. The infusion of remifentanil was adjusted for each patient during the operation, depending on their vital signs and BIS values.
Emergence conditions
Approximately 20 min before the termination of desflurane administration, pyridostigmine and glycopyrrolate were administered to reverse muscle relaxation, indicated by a train of four ≥90% (measured using MiniStim®, Life-Tech, TX, USA). Remifentanil was maintained at 0.05 µg/kg per min until the patient gained consciousness and responded to verbal commands. Desflurane administration was terminated at the end of the surgery.
Patients were randomly assigned, using a computerized randomization program, to receive fresh gas flow rates of 100% oxygen after discontinuation of desflurane of 2 l/min (group D2), 4 l/min (group D4) or 6 l/min (group D6). One anaesthetist woke the patients after surgery, while a second anaesthetist simultaneously recorded all emergence-related data.
If no spontaneous ventilation was observed at the termination of desflurane administration, the ventilator was switched to synchronised intermittent mandatory ventilation mode. If spontaneous ventilation was present, manually assisted ventilation was performed, keeping pace with the spontaneous ventilation. The partial pressure of end-tidal carbon dioxide was maintained at 30–40 mmHg. No stimulation or suction was provided until the patient opened their eyes or moved. Once the patient had responded to a verbal command, the administration of remifentanil was terminated. Deep breathing with 100% oxygen (6 l/min) was then administered to patients in all three groups. After suction of the endotracheal secretions, the endotracheal tube was removed. The patient was monitored for excessive agitation during emergence and recovery (for up to 60 min), indicated by an inability to communicate or the need for medication or restraints due to overexcitement.
Monitoring during emergence
Patients were asked to open their eyes 3 min and 6 min after the termination of desflurane and every 1 min after that. The time to eye opening, time to spontaneous movement and time to extubation (emergence time) were recorded. The end-tidal desflurane concentration and BIS were also recorded at each of these time points. From the end of desflurane administration until the endotracheal tube was removed, mean arterial pressure and heart rate were recorded every 3 min, then at 1 min after extubation. The patient’s memory of the surgery was tested by verbal questioning 30 min after transfer to a recovery room and then 24 h after surgery.
Statistical analyses
In a pilot study of 35 patients (unpublished data), times to extubation were 17.4 ± 4.3 min, 8.8 ± 1.8 min and 9.8 ± 2.1 min in groups D2, D4 and D6, respectively; extubation times were significantly longer in group D2 than group D4 (P = 0.017) and group D6 (P = 0.025), but there was no significant difference between groups D4 and D6. In order to detect a 1-min difference between the groups at a 5% level of significance and 80% power, at least 33 patients would be required in each group. To allow for dropouts, a group size of 35 patients was chosen.
Data were reported as either the mean ± SD or n. Fisher’s exact test was used to analyse differences according to sex. The three groups were compared via one-way analysis of variance followed by a post-hoc Dunnett’s test for multiple comparisons. Pearson’s correlation analysis was performed to assess relationships between the demographic variables and emergence time (time to extubation). A P-value <0.05 was considered to be statistically significant. All statistical analysis were performed using SAS software version 9.2 (SAS Institute, Cary, NC, USA).
Results
Demographic and operation characteristics for patients given 100% oxygen at 2 l/min (group D2), 4 l/min (group D4) or 6 l/min (group D6) following desflurane anaesthesia.
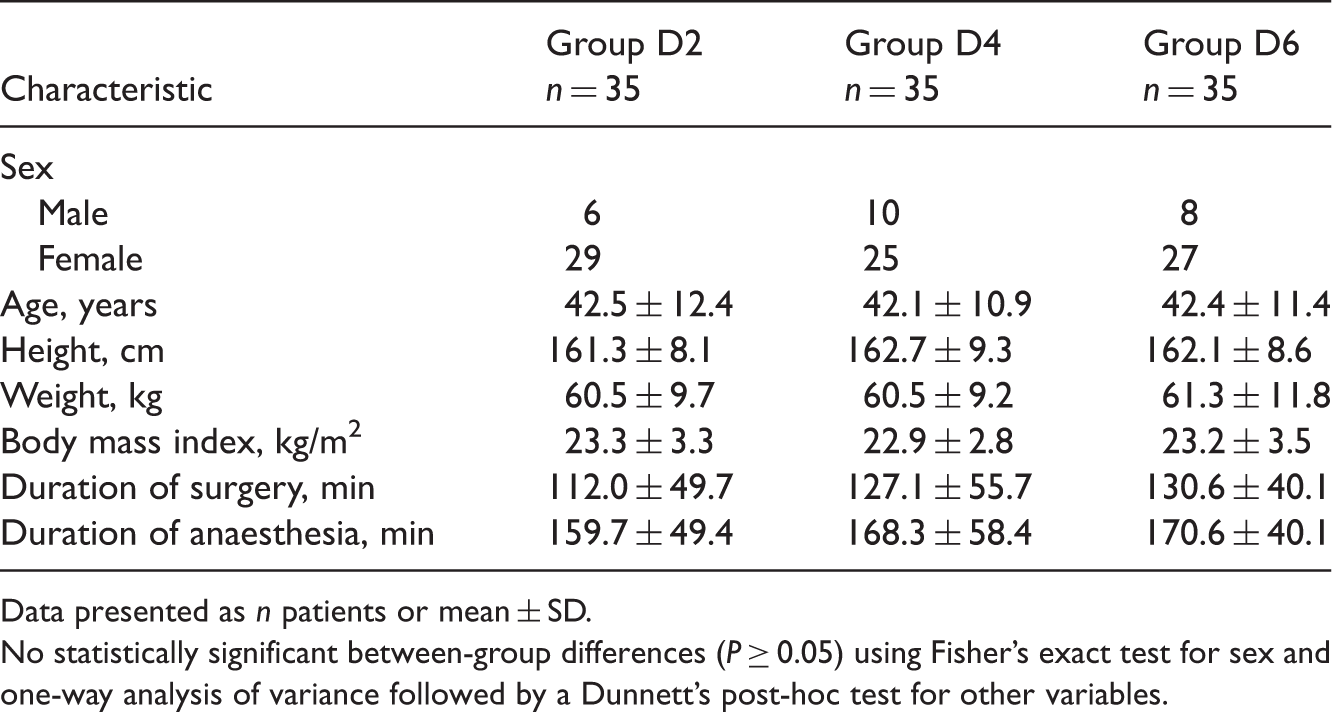
Data presented as n patients or mean ± SD.
No statistically significant between-group differences (P ≥ 0.05) using Fisher’s exact test for sex and one-way analysis of variance followed by a Dunnett’s post-hoc test for other variables.
Time to eye opening, spontaneous movement and extubation in patients given 100% oxygen at 2 l/min (group D2), 4 l/min (group D4) or 6 l/min (group D6) following desflurane anaesthesia.

Data presented as mean ± SD.
P < 0.001 compared with group D4.
P < 0.001 compared with group D6 (one-way analysis of variance followed by a post-hoc Dunnett’s test).
End-tidal concentrations of desflurane at various timepoints in patients given 100% oxygen at 2 l/min (group D2), 4 l/min (group D4) or 6 l/min (group D6) following desflurane anaesthesia.

Data presented as mean ± SD.
P < 0.001 compared with group D4.
P < 0.001 compared with group D6 (one-way analysis of variance followed by a post-hoc Dunnett’s test).
Bispectral index at various timepoints in patients given 100% oxygen at 2 l/min (group D2), 4 l/min (group D4) or 6 l/min (group D6) following desflurane anaesthesia.

Data presented as mean ± SD.
No statistically significant between-group differences (P ≥ 0.05) using one-way analysis of variance followed by a post-hoc Dunnett’s test.
Mean arterial pressure and heart rate measured at desflurane discontinuation, eye opening, spontaneous movement or extubation did not differ significantly between the groups (Figure 1).
Changes in mean arterial pressure and heart rate in patients given 100% oxygen at 2 l/min (group D2), 4 l/min (group D4) or 6 l/min (group D6) following desflurane anaesthesia. T1, eye opening on verbal command; T2, spontaneous movement; T3, just before extubation; T4, 1 min after extubation. Data presented as mean ± SD. There were no statistically significant between-group differences (P ≥ 0.05; repeated measures analysis of variance followed by a Dunnett’s post-hoc test).
Pearson correlation analysis between time to extubation and other variables following desflurane anaesthesia (n = 105).
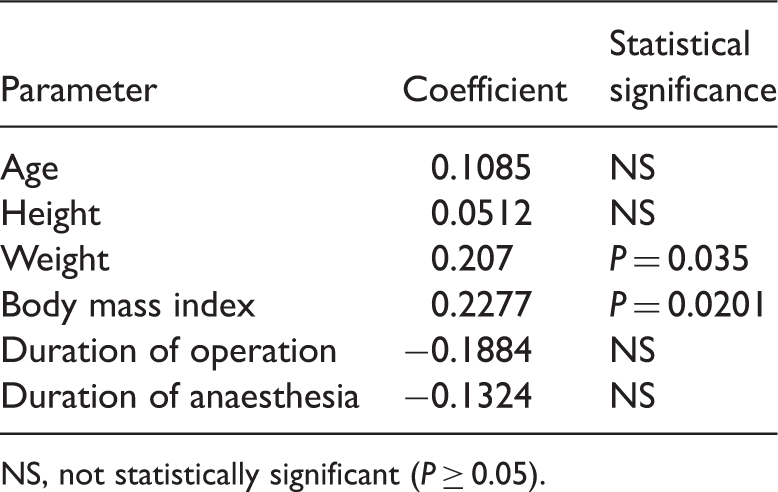
NS, not statistically significant (P ≥ 0.05).
Discussion
In the present study, the times from desflurane discontinuation to extubation were 17.6 ± 5.6 min, 9.9 ± 2.8 min and 9.1 ± 3.2 min in groups D2, D4 and D6, respectively, which are in good agreement with the results of the pilot study (17.4 ± 4.3 min, 8.8 ± 1.8 min and 9.8 ± 2.1 min, respectively). These results suggest that it is possible to predict emergence time based on fresh gas flow rate following desflurane anaesthesia.
As expected, the time to extubation increased with decreasing fresh gas flow rate; with a low gas flow rate the proportion of inhaled anaesthetic in the patient's body and the anaesthetic circuit that is discharged through the vacuum pump system is small during emergence, and the patient’s rebreathing rate will be increased. As a result, the anaesthetic concentration will decline very gradually. Therefore, if desflurane administration is terminated at a predetermined time before the end of surgery, a low-flow rate can be continued until emergence.
Contrary to expectations, there were no statistically significant differences in time to eye opening, time to spontaneous movement or time to extubation between groups D4 and D6. Likewise, no significant difference was detected between end-tidal desflurane concentrations measured at these times (except at time to spontaneous movement). This could be because fresh gas flow rates of 4 l/min or above matched the minute ventilation very closely, such that little or no gas was reused in the system. 11 Therefore, it is likely that a rate of 4 l/min is sufficient to wake patients. As oxygen and anaesthetic gases are expensive, increasing the flow rate to more than 5 l/min may not be economical, especially if it is unlikely to improve outcomes.
In group D2, the end-tidal desflurane concentration was significantly higher than that of the other groups at eye opening, spontaneous movement and extubation. Because the BIS values did not differ between the low-flow group and the other treatment groups, inadequate emergence did not seem to occur. All the end-tidal desflurane concentrations were lower at these timepoints than the minimum alveolar concentrations at which an anaesthetized patient responds appropriately to spoken commands reported by Song et al. 12 and Chortkoff et al. 13 This is likely to be due to the effect of remifentanil, as opioids can reduce minimum alveolar concentration values via interaction with inhaled anaesthetics.14–16
Because the administration of inhaled anaesthetic should be terminated early in clinical applications, there was concern about whether patients would be more aware than would usually be expected. However, none of the patients reported having any memory of the surgery.
As the anaesthetic concentration decreased slowly in the low-flow group during emergence, the difference in concentration between the brain and the lungs was small. Because the rates of emergence agitation, and of increased mean arterial pressure and heart rate, are likely to be lower than in high-flow groups, a more stable and smooth emergence was originally expected in the low-flow group. However, in the present study there was no particular advantage in terms of emergence agitation, mean arterial pressure or heart rate in the low-flow group, possibly because remifentanil was also used.
In the present study, body weight and the associated characteristic of body mass index were both significantly correlated with time to extubation, whereas age, sex and height were not. However, since patients aged ≥ 65 years were excluded from the study, these results cannot be generalised to those in this age group.
The lowest fresh gas flow rate used in the present study was 2 l/min. However, it may be necessary to study emergence at even lower flow rates. The results of the present study allow prediction of the emergence time with fresh gas flow rates of 2, 4 or 6 l/min, a mean end-tidal desflurane concentration of 5.4 vol% at the termination of desflurane administration for an approximately 3-h surgical procedure using desflurane and remifentanil. Many factors can affect the recovery pattern.17–22 The rate of recovery is faster with desflurane anaesthesia than with sevoflurane, and is faster with sevoflurane anaesthesia than with isoflurane. Furthermore, it is also delayed with a prolonged operation time, lower fresh gas flow rate and higher fraction of inhalation anaesthetic. Thus, adjustments will be required according to the individual situation. The development of devices for automatically controlling the end-tidal inhalation anaesthetic concentration has allowed the maintenance of the targeted end-tidal volatile anaesthetic concentration at a low fresh gas flow with small amounts of inhalation anaesthetic.23,24 If this strategy is used during the emergence period, patients can be awakened more comfortably and cost effectively, compared with other strategies.
The findings of the present study failed to clarify the economic benefits of a rate of 2 l/min during emergence. While the economic benefits of low flow rates have been reported previously,1,2,4,6 they are extremely difficult to estimate during the emergence phase alone. Using the computer simulation program Gas Man® version 4.2 (http://www.gasmanweb.com/software.html), with a low fresh gas flow of 2 l/min during surgery and emergence and an end-tidal desflurane concentration of 5.4 vol% (patient body weight 60 kg), about 1 l of desflurane can be saved compared with a high flow rate of 6 l/min, giving a cost saving of $1.6 at a liquid desflurane cost of $35.5/100 ml. If anaesthesia is maintained at 4 l/min, about 1.9 l of delivered desflurane can be saved, resulting in a cost saving of $3.2. The savings in terms of cost and volume of inhalation agent used are small, and the cost of anaesthesia is much lower than the cost of surgery, suggesting that, if only emergence was considered, the economic benefits would be minor. However, even if the economic benefit in each individual patient is small, the cumulative savings could be large.
In conclusion, it is possible to use a low-flow technique during the emergence period as well as the maintenance period without delaying recovery if the inhaled anaesthetic is stopped at a predicted time before the end of surgery. This may help to reduce anaesthetic consumption, with potential global environmental and economic benefits. Further clinical trials to investigate low-flow rates during emergence are warranted.
Footnotes
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.