
Abstract
Objective
A prospective, observational study to investigate how photoplethysmography (PPG) signals change during lumbar sympathetic blockade (LSB), and whether these changes can predict sympathetically mediated pain (SMP).
Methods
Patients with unilateral lower extremity pain and self-reported cold hyperalgesia underwent LSB. Bilateral temperature and PPG signals (AC and DC) were recorded. Power spectrum analysis (PSA) was performed.
Results
Of the total patient cohort (n = 38), eight patients (22.1%) had excellent pain-relief after LSB and were determined to have SMP. In all patients, the PPG AC signal changed immediately after drug administration, before any temperature change. DC signals decreased slowly in a linear fashion. PSA of DC signals showed significantly lower low-frequency/high-frequency (LF/HF) ratios in the SMP group than the sympathetically independent pain group, both before and after LSB. A cut-off value of 2.92 for LF/HF resulted in sensitivity, specificity and positive predictive values for SMP of 75.0%, 76.7% and 3.21 [1.5, 6.9], respectively.
Conclusions
PPG may be used as an early indicator of a successful LSB and could also be helpful in diagnosing SMP.
Keywords
Introduction
Lumbar sympathetic block (LSB) is a useful nonsurgical procedure to manage pain associated with medical conditions involving the lower extremities.1,2 Local anaesthetic is injected percutaneously around the lumbar sympathetic ganglia, resulting in temporary sympathectomy. 3 When this sympathetic blockade results in substantial pain relief, the presence of predominantly sympathetically mediated pain (SMP) is assumed.4–6 Sufficient pain relief can help patients to restore and improve their daily living functions, but it is difficult to predict the patient’s response to sympathetic blockade.
The success of LSB can be determined by evaluating vasodilatation2,7 via skin temperature monitoring of the plantar surface of the foot or other regions.8–12 Photoplethysmography (PPG) detects blood volume changes in the microvascular bed, 13 providing valuable information about the cardiovascular system (represented by a pulsatile AC waveform) and the autonomic function (represented by a slowly varying DC baseline).14,15 In particular, the DC component of PPG reflects sympathetic activity and thermoregulation. 15
Treatment guidelines published in 2010 recommend the use of LSB as a single component of the multimodal treatment of complex regional pain syndrome (CRPS), and state that its long-term use should be limited, especially in cases of non-CRPS neuropathic pain. 16 However, several medical conditions such as herpes zoster and postherpetic neuralgia involve neuropathic pain that comprises a clear sympathetically mediated component. 6 Because pain relief is subjective and individual, it is important to discriminate between SMP and sympathetically independent pain (SIP), unlike objective tests of blockade (including increasing skin temperature due to increased blood flow).12,17 This raises the question: should diagnostic sympathetic block always aim to identify SMP? 18
Although PPG signals are not fully understood, we hypothesized that signal changes in both the AC and DC components would occur around the onset of LSB. The aim of the present study was to investigate how PPG signals change during LSB, and whether such changes can predict SMP.
Patients and methods
Study population
The study recruited consecutive patients attending the Department of Anaesthesia and Pain Medicine, Seoul National University Hospital, Seoul, Republic of Korea, between December 2009 and April 2011, for diagnosis or treatment of unilateral lower extremity pain with self-reported cold hyperalgesia. Inclusion criteria were American Society of Anesthesiologist’s Physical Status Classification I or II, 19 and no significant cardiac, pulmonary or systemic disease. Patients aged <19 or >70 years, those who were not willing to participate, those with contraindications to regional anaesthesia, and those in whom it was not possible to monitor foot temperature and PPG signals (for example, patients with foot amputation) were excluded.
The study protocol was approved by the Institutional Review Board of the Seoul National University Hospital (IRB NO. H-0906-010-282), and all patients provided written informed consent prior to enrolment.
Lumbar sympathetic blockade
Prior to LSB, venous blood samples were taken from each patient in order to evaluate possible haematological interference of lights absorption via the pulse oximetry sensor (including assessment of red blood cell count, haemoglobin, haematocrit, total bilirubin, albumin and total protein levels). 14 Pain intensity was measured using an 11-point numeric rating scale (NRS: 0,no pain; 10,worst imaginable pain) before LSB, repeated1 week later. 20 Unilateral LSB was performed at the upper third of the L3 vertebra without any premedication, as described.12,21 Patients were placed in a prone position with a pillow under the lower abdomen to reduce lumbar lordosis, and their backs were covered with sterile drapes to avoid the influence of the ambient temperature, which was constantly maintained within 23–24℃.22–24 Only the areas of skin required for the procedure remained exposed. The target lumbar vertebra was identified by anteroposterior fluoroscopic imaging (OEC® 9800 Plus; GE Medical Systems, Salt Lake City, UT, USA) and the fluoroscopic C-arm was then adjusted 30° laterally to avoid the transverse process over the needle pathway.
The skin entry point was infiltrated using 1% lidocaine. A curved 21-guage, 15-cm Chiba needle (Cook, Bloomington, IN, USA) was then advanced toward the anterolateral edge of the target lumbar vertebra under fluoroscopic guidance using the tunnel vision (coaxial) technique.21,25 After confirming the needle position with anteroposterior, lateral and oblique views, and verifying negative aspiration for blood, 3 ml of iopamidol (Iopamiro®, Bracco, Milan, Italy) was administered incrementally, followed by 10 ml of 0.25% levobupivacaine (Chirocaine®, Abbott, Elverum, Norway).
Temperature monitoring
As an index of the efficacy of sympathetic blockade, skin surface temperatures were monitored with small adhesive thermocouple probes (accuracy±0.1℃; Dash 4000; GE Healthcare, Milwaukee, WI, USA) attached bilaterally to the plantar surface of the feet using transparent patches (TegadermTM; 3 M Health Care, St Paul, MN, USA).2,12 The baseline temperature was obtained immediately after placement of sterile surgical drapes. Temperatures were measured at 1-min intervals and recorded automatically from the time of administration of the local anaesthetic onwards. 12 Assessments were continued for a maximum of 20 min.
The LSB procedure was considered successful when changes in temperature met the following two criteria: unilateral difference in temperature on the target side was >2℃ within 20 min after injection of local anaesthetic 26 ; and the rate of temperature change of the skin was 0.4℃/min at the onset of sympathetic block. 12
Photoplethysmography
A commercially available pulse oximetry sensor (DS-100A Nellcor® R-Cal; NellcorTM, Mansfield, MA, USA) was used at wavelength 890 nm with transmission mode. For PPG recording, a device of our own design was used. 27 The output signal from the pulse oximetry sensor was converted into a voltage and amplified, then filtered with a band-pass of 0.05–10 Hz to separate the pulsatile AC signal, with an analogue low-pass cut-off at 1 Hz to separate the DC signal. A constant current source circuit was used to drive the LED and the amplification ratio was kept constant. The PPG waveform was continuously collected from the right and left second toes. An electrocardiogram (ECG) was obtained simultaneously using a patient monitor (Dash4000). All analogue signals (AC and DC signals from PPG and ECG) were digitized at a sampling rate of 200 Hz with 12-bit resolution using a Biopac data acquisition system (Biopac; Biopac Systems, Goleta, CA, USA). At the end of the study, PPG waveforms were analysed blindly off-line by a technician (H.J.B.) using Matlab® 7.1 (The MathworksTM Inc., Natick, MA, USA).
Several timepoints were set according to events occurring during the procedure: surgical draping (event 1); local infiltration for skin anaesthesia (event 2); deep muscle infiltration (event 3); contrast medium injection (event 4); initiation of local anaesthetic injection at the target point (event 5); completion of local anaesthetic injection (event 6); cut-off point of temperature monitoring and needle withdrawal (event 7); end of study (event 8).
Data analysis
Time domain
To investigate changes in PPG signal amplitude during LSB, data collected after event 6 were selected and normalized with respect to subject-specific values by dividing the selected PPG signal by the mean value. The beat-to-beat amplitude of the AC signal was derived by detection of normalized PPG pulse peaks and valleys, and their differences during each heart cycle. The difference between successive peak-valley pairs was considered the peak-to-peak pulse amplitude of the PPG AC signal. Then, the mean beat-by-beat amplitude within 1-min time windows was determined. The amplitude of the DC signal was calculated by taking the mean of normalized DC signal samples within 1-min time windows. Data were compared between the target and control (contralateral without pain symptoms) sides.
Frequency domain
The DC signals in PPG are composed of low-frequency (LF, 0.04–0.15 Hz), and high-frequency bands (HF, 0.15–0.40 Hz), which vary according to sympathetic activities controlling the peripheral circulation (LF) and parasympathetic activities mostly related to respiratory consequence to cardiac output (HF). The LF/HF ratio reflects the balance between sympathetic and parasympathetic tone.28–32
Power spectral density was derived using the nonparametric method, periodogram function in Matlab for investigating how the power of a time series signal is distributed with frequency. The periodogram is the Fourier transformation of the autocorrelation sequence. Consider the signal Xn(R) of finite length N, the estimate of power spectrum can be determined by taking the Fourier transformation of the autocorrelation sequence and applying the convolution theorem. The input of the periodogram function was the PPG DC signal and the pre-processed RR-interval signal of ECG.
Spectral parameters, total power (TF; ≤0.4 Hz), LF (0.04–0.15 Hz) and HF (0.15–0.40 Hz) were obtained by the sum of the power in the relevant frequency range in the spectrum. Spectral parameters were also extracted from heart rate variability for comparison. Regularly sampled data are required to obtain the power spectrum, but RR-interval data from ECG is irregularly sampled. Therefore, RR-interval data were interpolated using the cubic spine method and resampled at 4 Hz, which adequately satisfies the Nyquist theory. 33 PSD was calculated using the periodogam method.
To avoid interference due to the transition period of sympathetic blockade, the periods between event 1 and 5 and between events 7 and 8 were considered the pre- and postphase of LSB, respectively. Data were compared between phases (pre/post) and sides (target/control). The differences between pre- and postphase spectral parameters of PPG DC and ECG (including TF, LF, HF and LF/HF) were determined.
Statistical analyses
Data were presented as n, mean ± SD, or mean ± 95%CI. Statistical comparisons of parametric data were performed using paired t-test, and comparisons of nonparametric data were performed using χ2-test, Fisher’s exact test, or Mann–Whitney U-test. Patients were stratified between two groups according to the reported degree of pain relief: sympathetically mediated pain (SMP; NRS pain score decreased to <2 for at least 1 week) and sympathetically independent pain (SIP). A receiver operator characteristic (ROC) curve was constructed using a pre-phase LF/HF ratio of the target side as a diagnostic test to predict SMP. Data were analysed using SPSS® version 19.0 (IBM SPSS Statistics, CA, USA) for Windows®. P-values < 0.05 were considered statistically significant.
Results
Demographic and clinical characteristics of patients with unilateral lower extremity pain and self-reported cold hyperalgesia, included in a study to investigate the diagnosis of sympathetically mediated pain via photoplethysmography during unilateral lumbar sympathetic blockade, stratified according to the reported degree of pain relief: sympathetically mediated pain (SMP; pain intensity decreased below 2 for ≥1 week); sympathetically independent pain (SIP).
Data presented as n (%) or mean ± SD.
P < 0.01, SMP group vs SIP group; Mann–Whitney U-test.
Numeric rating scale (0, no pain; 10, worst pain possible).
Postherpetic neuralgia, herniated nucleus pulposus, diabetic peripheral neuropathy, paraplegia and Raynaud disease.
CRPS, complex regional pain syndrome; CRPS–NOS, complex regional pain syndrome not otherwise specified. 32
In the total patient group, mean time to onset of LSB was 5.11 ± 2.56 min after injection of local anaesthetic. Mean temperature of the target side was significantly lower than the control side until 3 min after drug administration (P < 0.01), and significantly higher than control from 1 min after onset (P < 0.01) (Figure 1a). There were no differences at 1 min before onset, or at onset.
Time course of temperature and photoplethysmography (PPG) signals after administration of local anaesthetic in unilateral lumbar sympathetic blockade for patients with unilateral lower extremity pain and self-reported cold hyperalgesia (n = 38). (a) Changes at target side; (b) changes in AC signals of PPG in both target and control (contralateral) sides; (c) changes in DC signals of PPG in both sides. Data presented as mean ±95% confidence intervals. The colourversion of this figure is available at http://imr.sagepub.com.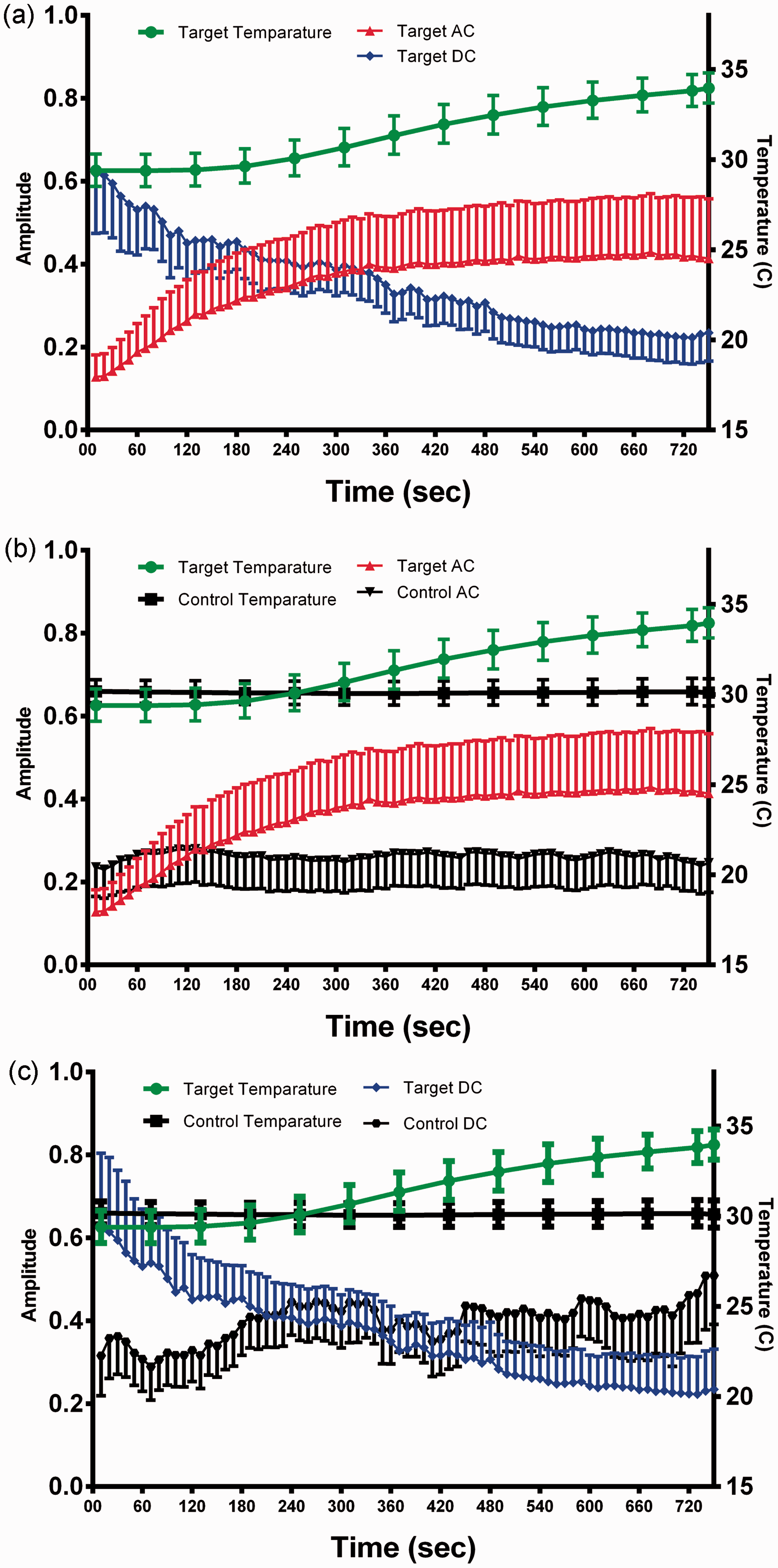
Data regarding AC amplitude of target and control are shown in Figure 1b. Target AC amplitude was significantly lower than control until 60 s after drug administration (P < 0.018), and significantly higher than control from 240 s after drug administration (P < 0.037; Figure 1b). Control AC amplitude was unchanged during LSB. The DC amplitude of the target was significantly higher than control until 120 s after drug administration (P < 0.039; Figure 1c), and gradually decreased over time (becoming significantly lower than control at 480 s after drug administration [P < 0.027]). Control DC amplitude increased slightly but not significantly during LSB. Changes in both DC and AC PPG signals occurred more rapidly than changes in temperature after drug administration.
Photoplethysmography low frequency/high frequency (LF/HF) ratio before (prephase) and after (postphase) administration of local anaesthetic in unilateral lumbar sympathetic blockade, for patients with unilateral lower extremity pain and self-reported cold hyperalgesia, stratified according to the reported degree of pain relief: sympathetically mediated pain (SMP; pain intensity decreased below 2 for ≥1 week); sympathetically independent pain (SIP).

Data presented as mean ± SD.
P < 0.05 vs SMP group; Mann–Whitney U-test.
P < 0.001 vs target pre-phase; paired t-test.
P < 0.01 vs control post-phase; paired t-test.
Eight patients (21.1%) were stratified into the SMP group. There were no differences in temperature change over time (initial temperature, onset time and final temperature; data not shown) or haematological parameters between patients with SMP and those with SIP. There were significant between-group differences in LF/HF ratio at prephase in both target and control, and postphase in target (P < 0.05 for each comparison; Table 2). There were no between-group differences between the pre- and postphase TF, LF, or HF at the target or at the control side.
Figure 2 shows the ROC curve for LF/HF in predicting SMP. At a cut-off value of 2.92, the area under the curve (AUC) was 0.742. The sensitivity, specificity and positive predictive value were 75.0%, 76.7% and 3.21 [1.5, 6.9], respectively.
Receiver operating characteristic (ROC) curve for photoplethysmography low frequency/high frequency (LF/HF) ratio in predicting sympathetically mediated pain in patients with unilateral lower extremity pain and self-reported cold hyperalgesia. At an LF/HF ratio cut-off value of 2.92, the area under the ROC curve = 0.742.
Discussion
The present study found that PPG signals are more useful than temperature monitoring for early assessment of successful LSB. PPG signals were useful for predicting the involvement of SMP and therefore the success of LSB. SMP was diagnosed in eight of 38 patients (21.1%) in the present study, a similar proportion to others using quantitative sensory testing after sympathetic blockade (25%). 18
In PPG, the pulsatile AC signal is related to the pumping action of the heart and the mean blood flow within the sample.14,15 Before administration of anaesthetic, temperature and AC amplitude were lower in the symptomatic limb than the control limb in the present study. This may be related to decreased blood volume due to vasoconstriction derived from high sympathetic tone. After initiation of LSB, blood volume increases as a consequence of vasodilatation in both arteries and veins. 34 The time between the initiation of AC signal change and temperature change was ∼180 s in the present study.
The onset time of LSB in the present study was similar to that shown in our earlier report using temperature monitoring (5 min), 12 but AC signals began to increase within 60 s after drug injection and amplitude inversions occurred ∼3 min before the onset of LSB (based on temperature changes). Although sympathetic denervation can increase blood influx and affect PPG signals by decreasing resistance of arterioles and increasing venous volume, the time gap between changes in PPG signals and temperature elevation (due to blood perfusion) may be explained by the fact that sympathetic nerve fibres are not distributed to capillaries. 35 The findings of the current study suggest that PPG AC signals may be used as an early indicator of successful LSB.34,36
The slowly varying PPG DC signals in the 0.01–0.40 Hz range are related to sympathetic nervous system activities, including relative vascularization and blood pooling within the sampling site. 14 In the present study, DC signal amplitude was greater in the target than in the control side, but it decreased gradually after anaesthetic administration and ultimately became lower than control values. Although amplitude inversion of DC signals progressed slowly, it occurred around the time of temperature change, suggesting that sympathetic activity decreased unilaterally as LSB progressed. In addition, the LF/HF ratio was significantly reduced in the target limb after the onset of LSB in the current study. The LF/HF ratio is used to indicate balance between sympathetic and parasympathetic tone,28,30 and a decrease may indicate a reduction in sympathetic tone. Our findings suggest that PPG DC signals may also be used as a tool for determining the success of LSB. However, the EEG-derived LF/HF ratio was not statistically significant, indicating that unilateral lumbar sympathetic blockade did not affect heart rate in the patients with normal cardiac function included in the present study.
The reduction in patient-reported pain intensity in the present study was 33.5% (mean scores, 7.13 before treatment and 4.74 at 1 week after treatment), suggesting that LSB was not always effective for managing pain in these patients. Generally, the efficacy of LSB is assessed on basis of at least a 50% reduction in pain relief.16,37,38 It is likely that preprocedural pathophysiological conditions are related to individual responses to LSB. In the present study, the preprocedural LF/HF ratio was paradoxically lower in the target limb than the control limb, in spite of lower temperatures and AC signal amplitudes. In other words, blood flow was reduced even though sympathetic activities were maintained at a lower level on the affected side. This phenomenon was observed in the entire patient population, but was especially notable in patients in the SMP group, who had a lower LF/HF ratio at the affected side than those in the SIP group. This finding may be related to a local compensatory mechanism of blood flow.
Blood flow is usually regulated according to tissue requirements, and is separated into acute control and long-term control. 39 In the acute phase of disease, local vascularity is increased to favour the healing process. Angiogenesis causes this increased blood flow to persist after healing, inducing local heat loss. This phenomenon encourages proximal vasoconstriction to decrease blood flow influx, ultimately promoting a vicious cycle in which distal sympathetic activities are decreased and local heat loss is increased. 38 In ischaemic pain, sympathetic blockade increases tissue blood flow, facilitating oxygen delivery and removal of pain-mediating substances. Because the effect of this artificial acute control by local anaesthetic diminishes over time, repetitive sympathetic blockades may be required for such patients.
It has been shown that there are no specific signs or symptoms that can be used to predict effective sympathetic blockade. 40 In the present study, 78.9% of patients (SIP group) did not respond to LSB sufficiently, and appeared to have an abnormal compensatory circulatory mechanism. In such cases, sympathetic blockade should be used as an accessory treatment option, since not even spinal cord stimulation can guarantee increased blood flow. 41
The present study had several limitations, including the nonrandomized analysis of PPG signals. A double-blinded process between independent signal analysis and statistical investigation could counterbalance this limitation, however. The study was also limited by the small sample size, which hindered the definition of a clear cut-off HF/LF value for diagnosis. Notwithstanding the need for further studies with larger sample sizes, we suggest that sympathetic blockade is helpful for pain relief when the LF/HF ratio on the affected side is below 2.92, approximately half that of the contralateral side.
In conclusion, PPG AC signal changes can be used as an early indicator for successful LSB, and could also be helpful in distinguishing between sympathetically mediated pain and sympathetically independent pain. Further studies should focus on finding the cut-off value for the diagnosis of sympathetically mediated pain.
Footnotes
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.