
Abstract
Objective
To determine the association between body mass index (BMI), serum prostate-specific antigen (PSA) level and PSA density (PSAD) in patients with an elevated serum PSA level but a negative prostate biopsy.
Methods
This retrospective study enrolled men with a negative prostate biopsy but a serum PSA level of 3.0–10 ng/ml. All men underwent anthropometric measurements, serum PSA determination and transrectal ultrasound examination. BMI was grouped according to the Asia-Pacific obesity criteria: nonobese (<25 kg/m2) versus obese (≥25 kg/m2). Partial correlation and linear regression models between PSA, PSAD and BMI were conducted after adjusting for age.
Results
A total of 907 men were enrolled in this study. On multivariate analyses, PSA showed no significant correlation with age or BMI, whereas PSAD had a negative correlation with age and BMI. Similar results were obtained when patients were categorized as having low (3.0 < PSA ≤ 6.5 ng/ml) or high PSA (6.5 < PSA ≤ 10.0 ng/ml) levels.
Conclusion
PSAD, but not PSA, demonstrated a significant negative correlation with BMI. This indicates that a new strategy including PSAD rather than simple PSA levels should be adopted in the study of obesity-adjusted PSA cut-offs.
Introduction
Obesity has been shown to be associated with lower serum prostate-specific antigen (PSA) levels, mainly due to a haemodilution effect of increased plasma volume.1–13 Based on these findings, some investigators have suggested that the currently accepted cut-off point for serum PSA should be lowered when evaluating obese patients in order to increase the sensitivity of the test.3,5,12
However, most of these studies were performed in screened populations whose mean PSA levels were generally low (0.78–1.36 ng/ml).2–14 Many clinicians regard the threshold of PSA to trigger a biopsy to be 2.5–3.0 ng/ml,1,2 which is much higher than the mean PSA of the screened populations.2–14 Despite their statistical significance, the magnitude of the changes in PSA with increasing body mass index (BMI) were small in these screened populations.4–7 For example, a substantial 10-point increase in BMI was associated with a PSA decrease of only 0.03 ng/ml. 14 Accordingly, it is possible that this marginal effect of obesity-related haemodilution of serum PSA is not apparent in groups with relatively high PSA levels. It is thus important to identify whether an obesity-related decrease in PSA would be equally evident in the practical indicators of prostate biopsy, especially in men with a negative biopsy result. If the same phenomenon is not observed in this group, the practical applications of this new concept might be limited.
The purpose of this study was to determine the association between BMI, PSA levels and prostate-specific antigen density (PSAD) in men with a negative prostate biopsy and PSA levels in the range of 3.0–10 ng/ml.
Patients and methods
Study population
This retrospective study reviewed clinical data from consecutive Korean patients with serum PSA levels 3–10 ng/ml who underwent initial extended prostate biopsy in the Department of Urology, College of Medicine, Soonchunhyang University, Cheonan, Korea between March 2009 and September 2012. All men underwent detailed clinical evaluations at the time of their extended biopsy. Urologists in the Department of Urology, College of Medicine, Soonchunhyang University consider a PSA level ≥3 ng/ml to be an indication for biopsy. Patients who took medications that were likely to influence the PSA level such as 5α-reductase inhibitors, Serenoa repens or testosterone before the measurement of PSA, or those with a history of malignant neoplasm in the bladder, were excluded from the study. BMI was defined as weight (kg) divided by the square of height (m2). BMI was categorized according to the Asia-Pacific criteria of obesity as follows: nonobese (<25 kg/m2) versus obese (≥25 kg/m2). 15
The study was approved by Soonchunhyang University Hospital Institutional Review Board (no. 2012-054), Soonchunhyang University, Cheonan, Korea. Patient consent was not required because of the retrospective nature of the study.
Analysis of serum PSA concentration
Venous blood samples from each patient were collected in 10-ml BD SST™ vacutainer tubes (Becton, Dickinson and Co., Franklin Lakes, NJ, USA). The serum was separated rapidly by centrifugation for 10 min at 1300
Prostate examinations
The prostate was measured in three dimensions by transrectal ultrasonography using an 8.0 MHz rectal probe (LOGIQ P6 ultrasound system; GE Healthcare, Little Chalfont, UK). Prostate volume (PV) was estimated using a modification of the prolate ellipsoid formula and recorded in cm3 (0.523 [length (cm) × width (cm) × height (cm)]). PSAD was defined by calculating the quotient of PSA and PV. Patients underwent transrectal ultrasound-guided extended biopsies (10–12 cores) regardless of digital rectal examination findings.
Statistical analyses
All statistical analyses were performed using the SAS statistical package, version 9.2 (SAS Institute, Cary, NC, USA). Mean ± SD, median (interquartile range) and n of patients (%) values were used as appropriate to describe the data. A partial correlation test was used to evaluate the association among BMI, PSA, PV and PSAD after adjusting for age. A linear regression model was used to test the regression of PSA or PSAD by BMI group while simultaneously adjusting for age and/or PV. The estimated effects with 95% confidence intervals (CI) for PSA and PSAD were evaluated for each BMI category. All statistical analyses were two-tailed and a P-value <0.05 was considered statistically significant.
Results
Demographic and clinical characteristics of a study population who had negative prostate biopsy results and serum prostate-specific antigen levels 3–10 ng/ml (n = 907).
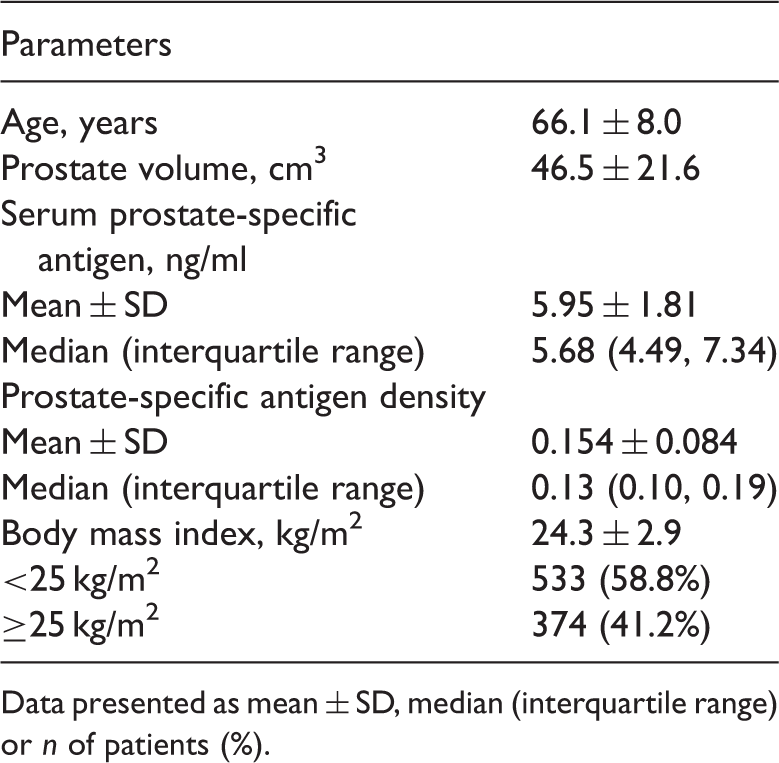
Data presented as mean ± SD, median (interquartile range) or n of patients (%).
Partial correlation between body mass index (BMI), prostate volume (PV), serum prostate-specific antigen (PSA), and PSA density (PSAD) after adjustment for age in a study population who had negative prostate biopsy results and serum prostate-specific antigen levels 3–10 ng/ml (n = 907).

Statistical significance at P < 0.05.
NS, no significant correlation (P ≥ 0.05).
Multivariate regression analysis between serum prostate-specific antigen (PSA) and age, prostate volume (PV) and body mass index (BMI) in a study population who had negative prostate biopsy results and serum prostate-specific antigen levels 3–10 ng/ml (n = 907) stratified according to their PSA levels.

Statistical significance at P < 0.05.
CI, confidence interval; SE, standard error; NS, no significant correlation (P ≥ 0.05).
Multivariate regression analysis between serum prostate-specific antigen density and age and body mass index (BMI) in a study population who had negative prostate biopsy results and serum prostate-specific antigen (PSA) levels 3–10 ng/ml (n = 907) stratified according to their PSA levels.
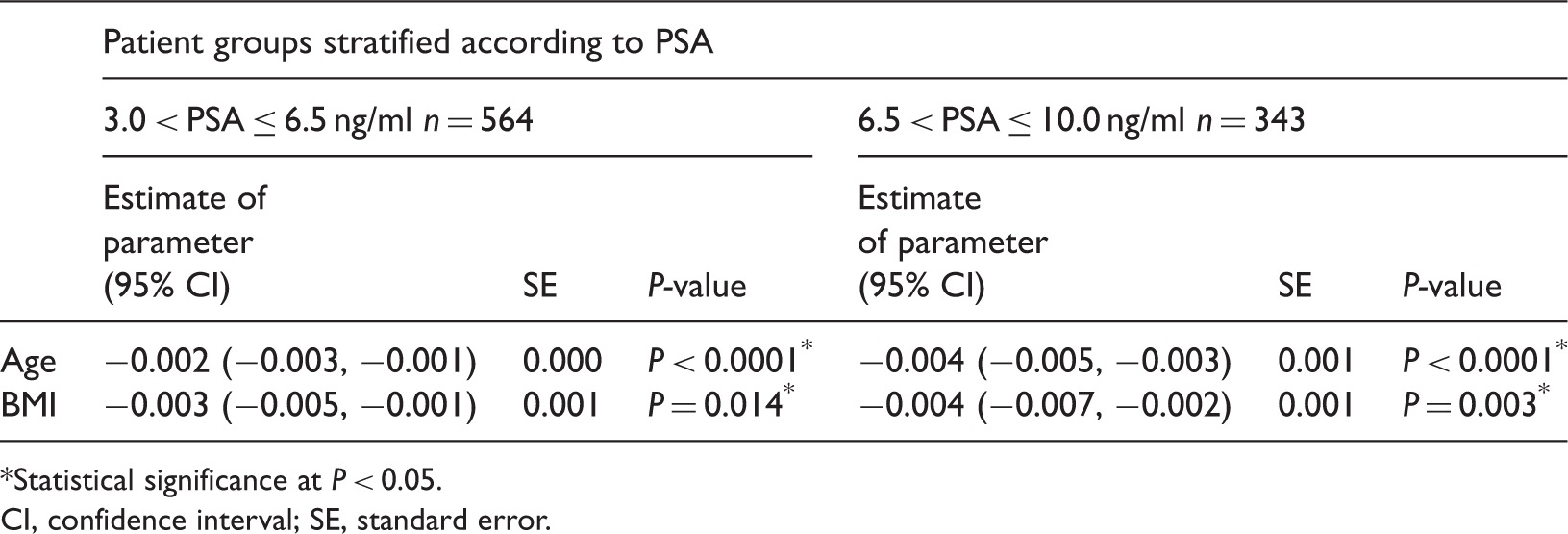
Statistical significance at P < 0.05.
CI, confidence interval; SE, standard error.
Discussion
There are few data on the association between obesity and PSA in a biopsy-indicated population, and these have not shown a clear relationship.16,17 Fowke et al. 16 demonstrated an association between obesity, PV, PSA and PSAD among men referred for prostate biopsy. In a relatively small number of men with a negative biopsy (n = 380), PSAD generally decreased with increasing BMI, although statistical significance was not reached. 16 PSA alone showed no correlation with BMI and the authors concluded that, among biopsy-negative subjects, BMI was associated with PV, leading to a lower PSAD with greater body size. 16 In another study of men with negative biopsies, obesity was significantly associated with a larger PV, but there was no correlation with PSA. 17 There was no information on the association between obesity and PSAD. 17
Likewise, this present study showed that PSAD had a significant negative correlation with BMI while PSA alone showed no correlation with BMI. A recent growing body of evidence suggests that obese men may have lower serum PSA,2–13 mainly due to a haemodilution effect. In contrast, obesity has been positively correlated with PV in multiple study populations10–13 and it is well known that a larger PV is associated with a higher serum PSA level. Therefore, obesity has conflicting influences on serum PSA level. The effect of PV on increasing PSA might be greater than the dilutional effect of obesity on decreasing PSA. In fact, some recent studies have revealed that obesity is correlated with higher serum PSA,17,18 in contrast to former studies.2–13
These current findings of a significant negative correlation between PSAD and BMI indicate that the haemodilution effect also existed in this population with high PSA levels (i.e. with practical biopsy indicators); however, this is expressed only after compensating for the enlarged PV by using PSAD. This indicates that a new strategy for PSA measurement that includes PSAD rather than simple PSA alone should be adopted in the study of obesity-adjusted PSA cut-offs.
This present study also showed no significant correlation between age and PSA, probably because the cohort of men with a negative prostate biopsy was a highly selected group that differed from the normal population because they presented with an abnormal PSA that indicated the need for a biopsy. The patients in this current study generally had a large PV (mean = 46.5 cm3). Overall, the association between BMI and PSAD appears to be attributable to the relationship between BMI and PV. The negative biopsy group favours men who may be most susceptible to prostate enlargement, and it is possible that the effects of obesity on PV may be more easily detected within this group.
The International Association for the Study of Obesity proposed a criterion for obesity of BMI ≥ 30 kg/m2 based on data from a Caucasian population. 19 However, for people from the Asia-Oceania region, whose main form of energy intake is carbohydrate, obesity has been defined as a BMI ≥ 25 kg/m2. 15 This difference in BMI cut-off is quite large and could have influenced the study results. If this present study had used the Western criteria for obesity, only 2.4% (22 of 907) of the participants would have been classified as obese. Therefore, these current results might not be applicable to populations in other countries.
In summary, obesity-related haemodilution of serum PSA was found among men with a negative biopsy with PSA levels in the range of 3–10 ng/ml. However, this phenomenon can be demonstrated only after compensating for the enlarged PV by using PSAD. This indicates that a new strategy for PSA measurement that includes PSAD rather than simple PSA levels should be adopted in the study of obesity-adjusted PSA cut-offs.
Footnotes
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This work was supported in part by the Soonchunhyang University Research Fund.